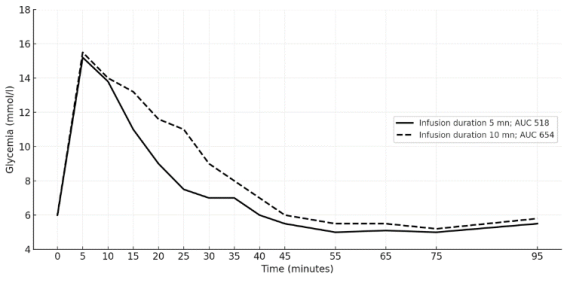
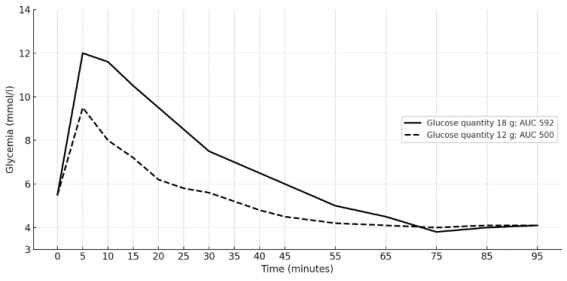
Introduction: The intravenous glucose tolerance test (IVGTT) is acknowledged as the gold standard for assessing insulin sensitivity, as it provides the glucose clearance rate (Kg) from the bloodstream. The ICARUS panel expert protocol for the implementation of the IVGTT involves the administration of a high dose of glucose over a brief bolus period, which is risky and may result in discomfort. This study aimed to demonstrate the feasibility of a heparin-assisted IVGTT with a lower glucose infusion rate and to determine the glucose clearance rate from blood (Kg) for healthy black African adults using a modified ICARUS protocol. Methods: In a modified ICARUS protocol, heparin was administered to six healthy black African volunteers to prevent clotting in an indwelling catheter. Then, an infusion of 0.33 g/kg glucose was administered over 5–10 min instead of the usual 0.50 g/kg over 3 min. Blood sampling was performed every 5–10 min for up to 95 min. Blood glucose levels were determined using the glucose oxidase method. Timed blood glucose curves were plotted, and the following parameters were determined: area under the curve (AUC), baseline return time, and glucose clearance rate (Kg). Results: No bleeding symptoms or other adverse events were observed. The blood glucose peak ranged from 9.4 to 15.3 mmol/L. The baseline returned time ranged from 45 to 55 minutes. Kg ranged from 1.6 to 2.7, depending on the amount of infused glucose. The AUC varied with the amount of infused glucose and infusion duration. The Staub effect was not observed in this study. The features of the curves were all plausible compared to those obtained in healthy subjects using the original Icarus protocol. Conclusion: Under our experimental conditions, we achieved IVGTT using a heparin-assisted IVGTT protocol with reduced glucose infusion rates, and determined the glucose clearance rate. This protocol is feasible and can potentially be used to assess insulin sensitivity. The protocol can be applied on a larger scale to determine its statistical features.
| Published in | Advances in Biochemistry (Volume 14, Issue 2) |
| DOI | 10.11648/j.ab.20261402.13 |
| Page(s) | 34-42 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Glucose, IVGTT, Glucose Clearance Rate, Insulin Sensitivity, Heparin
Subject parameters | Mean | Standard deviation | Units |
|---|---|---|---|
Age | 31.2 | 3.6 | year |
Weight | 66.7 | 16.9 | kg |
Height | 173.6 | 12.7 | cm |
Body mass index | 22.1 | 2.5 | cm/kg2 |
Fasting duration | 11.9 | 0.9 | hour |
Icarus protocol | Our Protocol | |
|---|---|---|
Number of volunteers | 20 | 6 |
Diet | 3 days (at least 150 g daily of carbohydrate) | |
Physical activity | Normal | |
Fasting (hours) | 10 - 16 | |
Tests time | 6.30 - 10.30 | |
T0 (min) | Start of glucose infusion | |
Infused glucose concentration (g/kg) | 0.50 | 0.33 |
Infusion duration | 3 min ± 15 sec | 5 - 10 min |
Arm for perfusion and blood collection | same arm | opposite arm |
Anticoagulant | none | heparin |
Mean | Standard deviation | Minimum value | Maximum value | |
|---|---|---|---|---|
Glycemia peak (mmol/l) | 12.84 | 2.17 | 9.38 | 15.26 |
Glucose disappearance rate (%/min) | 2.1 | 0.4 | 1.6 | 2.7 |
Baseline time return (minute) | 55 | 5.8 | 45 | 65 |
AUC | Area Under the Curve |
IVGTT | Intravenous Glucose Tolerance Test |
| [1] | Hieronimus B, Medici V, Lee V, Nunez MV, Sigala DM, Bremer AA, et al. Effects of Consuming Beverages Sweetened with Fructose, Glucose, High-Fructose Corn Syrup, Sucrose, or Aspartame on OGTT-Derived Indices of Insulin Sensitivity in Young Adults. Nutrients. 2 janv 2024; 16(1): 151. |
| [2] | Borai A, Livingstone C, Kaddam I, Ferns G. Selection of the appropriate method for the assessment of insulin resistance. BMC Med Res Methodol. 23 nov 2011; 11(1): 158. |
| [3] | Chiu KC, Chuang LM, Yoon C. Comparison of Measured and Estimated Indices of Insulin Sensitivity and β Cell Function: Impact of Ethnicity on Insulin Sensitivity and β Cell Function in Glucose-Tolerant and Normotensive Subjects 1. [cité 11 mars 2026]. Disponible sur: |
| [4] | Koh HCE, Patterson BW, Reeds DN, Mittendorfer B. Insulin sensitivity and kinetics in African American and White people with obesity: Insights from different study protocols. Obesity. 2022; 30(3): 655-65. |
| [5] | Bingley PJ, Colman P, Eisenbarth GS, Jackson RA, McCulloch DK, Riley WJ, et al. Standardization of IVGTT to Predict IDDM. Diabetes Care. 1 oct 1992; 15(10): 1313-6. |
| [6] | Coté CJ, Greenhow DE, Marshall BE. The Hypotensive Response to Rapid Intravenous Administration of Hypertonic Solutions in Man and in the Rabbit. Anesthesiology. 1 janv 1979; 50(1): 30. |
| [7] | Molinari A, Castagnola E, Mazzola C, Piacentino M, Fratino G. Thromboembolic complications related to indwelling central venous catheters in children with oncological/haematological diseases: a retrospective study of 362 catheters. Support Care Cancer. 1 oct 2001; 9(7): 539-44. |
| [8] | Burke LM, Cox GR, Cummings NK, Desbrow B. Guidelines for Daily Carbohydrate Intake. Sports Med. 1 avr 2001; 31(4): 267-99. |
| [9] | Vicini P, Cobelli C. The iterative two-stage population approach to IVGTT minimal modeling: improved precision with reduced sampling. American Journal of Physiology-Endocrinology and Metabolism. janv 2001; 280(1): E179-86. |
| [10] | Lott JA, Turner K. Evaluation of Trinder’s Glucose Oxidase Method for Measuring Glucose in Serum and Urine. Clin Chem. 1 nov 1975; 21(12): 1754-60. |
| [11] | Farkas GJ, Gordon PS, Trewick N, Gorgey AS, Dolbow DR, Tiozzo E, et al. Comparison of Various Indices in Identifying Insulin Resistance and Diabetes in Chronic Spinal Cord Injury. Journal of Clinical Medicine. 27 nov 2021; 10(23). |
| [12] | Godsland IF, Johnston DG, Alberti K, Oliver N. The importance of intravenous glucose tolerance test glucose stimulus for the evaluation of insulin secretion. Sci Rep. 28 mars 2024; 14(1): 7451. |
| [13] | Colman PG, Stewart V, Kean J, Koschmann M, Alford F, Ward G, et al. Comparison of Two Commonly Used Standard IVGTTs. Diabetes Care. 1 août 1992; 15(8): 1053-5. |
| [14] | McCulloch DK, Bingley PJ, Colman PG, Jackson RA, Gale EAM, The ICARUS Group. Comparison of Bolus and Infusion Protocols for Determining Acute Insulin Response to Intravenous Glucose in Normal Humans. Diabetes Care. 1 juin 1993; 16(6): 911-5. |
| [15] | Kurahashi K, Inoue S, Yoshida S, Ikeda Y, Morimoto K, Uemoto R, et al. The Role of Heparin Cofactor Ⅱ in the Regulation of Insulin Sensitivity and Maintenance of Glucose Homeostasis in Humans and Mice. Journal of Atherosclerosis and Thrombosis. 2017; 24(12): 1215-30. |
| [16] | Hansen HR, Wolfs JL, Bruggemann L, Sommeijer DW, Bevers E, Hauer AD, et al. Hyperglycemia accelerates arterial thrombus formation and attenuates the antithrombotic response to endotoxin in mice. Blood Coagulation & Fibrinolysis. oct 2007; 18(7): 627. |
| [17] | Ascaso JF, Pardo S, Real JT, Lorente RI, Priego A, Carmena R. Diagnosing Insulin Resistance by Simple Quantitative Methods in Subjects With Normal Glucose Metabolism. Diabetes Care. 1 déc 2003; 26(12): 3320-5. |
| [18] | Bonuccelli S, Muscelli E, Gastaldelli A, Barsotti E, Astiarraga BD, Holst JJ, et al. Improved tolerance to sequential glucose loading (Staub-Traugott effect): size and mechanisms. American Journal of Physiology-Endocrinology and Metabolism. août 2009; 297(2): E532-7. |
| [19] | Toffolo G, Cobelli C. The hot IVGTT two-compartment minimal model: an improved version. American Journal of Physiology-Endocrinology and Metabolism. févr 2003; 284(2): E317-21. |
APA Style
Ahiboh, H., Koffi, J. A., Kouakou, H. F., Yao-Yapo, C., Ankotche, A., et al. (2026). Feasibility and Outcomes of a Modified Intravenous Glucose Tolerance Test: Implications for Glucose Clearance Rate in Euglycemic Black Adults. Advances in Biochemistry, 14(2), 34-42. https://doi.org/10.11648/j.ab.20261402.13
ACS Style
Ahiboh, H.; Koffi, J. A.; Kouakou, H. F.; Yao-Yapo, C.; Ankotche, A., et al. Feasibility and Outcomes of a Modified Intravenous Glucose Tolerance Test: Implications for Glucose Clearance Rate in Euglycemic Black Adults. Adv. Biochem. 2026, 14(2), 34-42. doi: 10.11648/j.ab.20261402.13
@article{10.11648/j.ab.20261402.13,
author = {Hugues Ahiboh and Joelle Akissi Koffi and Henri Francisk Kouakou and Carine Yao-Yapo and Amos Ankotche and Edwige Siransy-Balayssac and Dagui Monnet and Marie-Laure Hauhouot-Attoungbre},
title = {Feasibility and Outcomes of a Modified Intravenous Glucose Tolerance Test: Implications for Glucose Clearance Rate in Euglycemic Black Adults},
journal = {Advances in Biochemistry},
volume = {14},
number = {2},
pages = {34-42},
doi = {10.11648/j.ab.20261402.13},
url = {https://doi.org/10.11648/j.ab.20261402.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ab.20261402.13},
abstract = {Introduction: The intravenous glucose tolerance test (IVGTT) is acknowledged as the gold standard for assessing insulin sensitivity, as it provides the glucose clearance rate (Kg) from the bloodstream. The ICARUS panel expert protocol for the implementation of the IVGTT involves the administration of a high dose of glucose over a brief bolus period, which is risky and may result in discomfort. This study aimed to demonstrate the feasibility of a heparin-assisted IVGTT with a lower glucose infusion rate and to determine the glucose clearance rate from blood (Kg) for healthy black African adults using a modified ICARUS protocol. Methods: In a modified ICARUS protocol, heparin was administered to six healthy black African volunteers to prevent clotting in an indwelling catheter. Then, an infusion of 0.33 g/kg glucose was administered over 5–10 min instead of the usual 0.50 g/kg over 3 min. Blood sampling was performed every 5–10 min for up to 95 min. Blood glucose levels were determined using the glucose oxidase method. Timed blood glucose curves were plotted, and the following parameters were determined: area under the curve (AUC), baseline return time, and glucose clearance rate (Kg). Results: No bleeding symptoms or other adverse events were observed. The blood glucose peak ranged from 9.4 to 15.3 mmol/L. The baseline returned time ranged from 45 to 55 minutes. Kg ranged from 1.6 to 2.7, depending on the amount of infused glucose. The AUC varied with the amount of infused glucose and infusion duration. The Staub effect was not observed in this study. The features of the curves were all plausible compared to those obtained in healthy subjects using the original Icarus protocol. Conclusion: Under our experimental conditions, we achieved IVGTT using a heparin-assisted IVGTT protocol with reduced glucose infusion rates, and determined the glucose clearance rate. This protocol is feasible and can potentially be used to assess insulin sensitivity. The protocol can be applied on a larger scale to determine its statistical features.},
year = {2026}
}
TY - JOUR T1 - Feasibility and Outcomes of a Modified Intravenous Glucose Tolerance Test: Implications for Glucose Clearance Rate in Euglycemic Black Adults AU - Hugues Ahiboh AU - Joelle Akissi Koffi AU - Henri Francisk Kouakou AU - Carine Yao-Yapo AU - Amos Ankotche AU - Edwige Siransy-Balayssac AU - Dagui Monnet AU - Marie-Laure Hauhouot-Attoungbre Y1 - 2026/05/14 PY - 2026 N1 - https://doi.org/10.11648/j.ab.20261402.13 DO - 10.11648/j.ab.20261402.13 T2 - Advances in Biochemistry JF - Advances in Biochemistry JO - Advances in Biochemistry SP - 34 EP - 42 PB - Science Publishing Group SN - 2329-0862 UR - https://doi.org/10.11648/j.ab.20261402.13 AB - Introduction: The intravenous glucose tolerance test (IVGTT) is acknowledged as the gold standard for assessing insulin sensitivity, as it provides the glucose clearance rate (Kg) from the bloodstream. The ICARUS panel expert protocol for the implementation of the IVGTT involves the administration of a high dose of glucose over a brief bolus period, which is risky and may result in discomfort. This study aimed to demonstrate the feasibility of a heparin-assisted IVGTT with a lower glucose infusion rate and to determine the glucose clearance rate from blood (Kg) for healthy black African adults using a modified ICARUS protocol. Methods: In a modified ICARUS protocol, heparin was administered to six healthy black African volunteers to prevent clotting in an indwelling catheter. Then, an infusion of 0.33 g/kg glucose was administered over 5–10 min instead of the usual 0.50 g/kg over 3 min. Blood sampling was performed every 5–10 min for up to 95 min. Blood glucose levels were determined using the glucose oxidase method. Timed blood glucose curves were plotted, and the following parameters were determined: area under the curve (AUC), baseline return time, and glucose clearance rate (Kg). Results: No bleeding symptoms or other adverse events were observed. The blood glucose peak ranged from 9.4 to 15.3 mmol/L. The baseline returned time ranged from 45 to 55 minutes. Kg ranged from 1.6 to 2.7, depending on the amount of infused glucose. The AUC varied with the amount of infused glucose and infusion duration. The Staub effect was not observed in this study. The features of the curves were all plausible compared to those obtained in healthy subjects using the original Icarus protocol. Conclusion: Under our experimental conditions, we achieved IVGTT using a heparin-assisted IVGTT protocol with reduced glucose infusion rates, and determined the glucose clearance rate. This protocol is feasible and can potentially be used to assess insulin sensitivity. The protocol can be applied on a larger scale to determine its statistical features. VL - 14 IS - 2 ER -
Faculty of Pharmaceutical and Biological Sciences, Félix Houphouët-Boigny University, Abidjan, Ivory Coast
Biography: Hugues Ahiboh, PharmD, PhD, is an Associate Professor within the Faculty of Pharmacy and Biological Sciences at Felix Houphouet-Boigny University, specializing in biochemistry and molecular biology. With a career spanning over three decades, Dr. Ahiboh currently serves as the Head of the Biochemistry and Clinical Chemistry Unit at the Centre for Diagnosis and Research in Health of the Treichville Teaching Hospital in Abidjan. His professional expertise is underpinned by advanced certifications in General and Medical Immunology, alongside previous experience as a medical laboratory scientist at the Institut Pasteur of Ivory Coast. Beyond his clinical and pedagogical responsibilities, he contributes to international capacity building as a member of the scientific and teaching board for the Afro Advanced Course on Diagnostics (ACDx), a collaborative initiative by the Merieux Fondation and the Institut Pasteur of Senegal.
Research Fields: Metabolic biochemistry, molecular genetics of infectious pathogens, Non-infectious diseases biomarkers in tropical socio-genetic contexts, Pharmacological and toxicological biochemistry of vegetal drugs

Center for Health Diagnosis and Research (CeDReS), Treichville University Hospital, Abidjan, Ivory Coast
Biography: Joelle Akissi Koffi, is a pharmacist and biologist working in the biochemistry unit of Centre for Diagnosis and Research in Health of the Treichville Teaching Hospital in Abidjan. She is also a teacher-research within the Faculty of Pharmacy and Biological Sciences at Felix Houphouet-Boigny University, specializing in biochemistry and molecular biology. Holder of a PhD, her work focuses on the interactions between of genetic factors, nutritional status and infectious diseases with a particular interest in iron metabolism. She is a member of the Ivorian Society of Clinical Biochemistry. Her professional expertise is underpinned by advanced certifications in General and Medical Immunology, Hematology, biochemistry, by a Master Biotechnology, biosafety, bioresource.
Research Fields: Metabolic biochemistry, molecular genetics of infectious pathogens (microbiome), Non-infectious diseases biomarkers in tropical socio-genetic contexts, pharmacological biochemistry

Center for Health Diagnosis and Research (CeDReS), Treichville University Hospital, Abidjan, Ivory Coast
Biography: Henri Francisk Kouakou is a pharmacist and biologist at the biochemistry laboratory of the Centre for Diagnosis and Research in Health of the Treichville University Hospital. Dr. KOUAKOU was a hospital intern (top of the 2018 competition) and he obtained his doctorate in pharmacy at the University Felix Houphouet Boigny in 2020, then his Diploma of Higher Studies in Clinical Biology in the same institution in 2022. In addition, he holds a certification on technical verification and biological validation in clinical biochemistry in accordance with ISO 15189. For two years, he was a biochemistry practical work instructor at the University Felix Houphouet Boigny. Dr. KOUAKOU has participated in research projects in recent years on haptoglobin and prostate cancer. He is currently preparing a Master in Reproduction and Development co-accredited by the universities of Paris Cite and Paris-Saclay.
Research Fields: Metabolic biochemistry, molecular genetics, clinical biochemistry, pharmacological biochemistry, reproductive biology, developmental biology

Faculty of Pharmaceutical and Biological Sciences, Félix Houphouët-Boigny University, Abidjan, Ivory Coast
Biography: Carine Yao-Yapo is a pharmacist biologist, assistant professor in the Department of Biochemistry of the UFR of Pharmaceutical and Biological Sciences of the University Felix Houphouet Boigny in Abidjan, Ivory Coast. She obtained her PhD in Biochemistry in 2024 from the University Félix Houphouet Boigny in Abidjan and a master’s degree in Biochemistry – Biosafety – Bioresources from the said university. She is a member of the Ivorian Society of Clinical Biochemistry and the French Society of Clinical Biology. She has participated in research work in collaboration with international teams mainly on the biological management of chronic kidney disease and its complications.
Research Fields: Diagnosis of chronic kidney disease in black Africans, PTH cut-off values of black African hemodialysis, vitamin D characteristics of black African hemodialysis, biological management of bone complications, hygienic and dietary prevention of cardiovascular diseases

Diabetes Clinic, Treichville University Hospital, Abidjan, Ivory Coast
Biography: Amos Ankotche is a distinguished Ivorian endocrinologist and former Head of the Diabetes Clinic at Treichville University Hospital in Abidjan. Dedicated to managing metabolic diseases, he is especially recognized for his commitment to pediatric care. As Coordinator for the Changing Diabetes in Children (CDIC) project, he has been instrumental in providing free insulin and essential monitoring equipment to diabetic youth aged 0 to 25. Under his leadership, the initiative established 22 specialized care centers nationwide and trained hundreds of healthcare professionals. A deeply engaged clinical practitioner, Dr. Ankotche organizes annual educational summer camps to foster self-management and autonomy among young patients. By tirelessly advocating for reduced insulin costs, he demonstrates an unwavering dedication to enhancing both the quality of life and life expectancy of diabetic youth in Ivory Coast.
Research Fields: Endocrinology, diabetology, pediatric, social education

Faculty of Medical Sciences, Félix Houphouët-Boigny University, Abidjan, Ivory Coast
Biography: Edwige Siransy-Balayssac is a medical doctor, tenured professor of medical physiology (2022, LAFPT-CAMES) at the Faculty of Medicine and Physiology of Felix Houphouët-Boigny University (Abidjan). She is the head of the UFR SMA's Research and Prevention Center in Medical Physiology and Pathophysiology and the head of the Functional Explorations Department at the Yopougon University Hospital (Abidjan). She obtained her master's degree in physiology (2011, Cheick Anta Diop University of Dakar, Senegal) and her PhD in Tropical Human Biology with a specialization in Physiology (2014, Felix Houphouet-Boigny University). She is a specialist in Cardiology (2004, Felix Houphouet-Boigny University), Sports Biology and Medicine (2005, Felix Houphouet-Boigny University), and Cardiovascular Prevention and Rehabilitation (medical option, 2018, Paris Descartes University,). She was awarded the UNESCO-L’OREAL Fellowship for Women in Science in 2003. She is Vice-President of the African Society of Physiology and Pathophysiology.
Research Fields: Cardiovascular physiology in Black Africans, Nutrition and blood pressure (salt, cocoa), Respiratory physiology (tobacco, capnography), Exercise physiology (exercise tests, physical rehabilitation), Body composition (fat and lean mass, Black Africans)

Faculty of Pharmaceutical and Biological Sciences, Félix Houphouët-Boigny University, Abidjan, Ivory Coast
Biography: Dagui Monnet, PharmD, PhD, is a Professor of Biochemistry and Molecular Biology at the University of Abidjan, having earned his doctorate from Paris XI in 1985. A distinguished pharmacist-biologist and hospital chief pharmacist with advanced credentials in public health and clinical biology, Professor Monnet was the directorate of the “École Préparatoire aux Sciences de la Santé d’Abobo-Abidjan” (1998–2001) and the Pharmacy of Public Health of Ivory Caost (2001–2004). he has participated in the creation of the Diploma of Specialized Studies in Clinical Biology, which he oversaw from 2010 to 2021. An active contributor to the international scientific community. He also supervises numerous PhD candidates. He serves as a judge for the CAMES competitive examinations for the aggregation of pharmacy professors.
Research Fields: Clinical Diagnostics: Nephrology, and clinical biochemistry, Metabolic & Nutritional Science, Biomarkers of inflammatory pathologies, Public health strategy and implementation in Africa

Faculty of Pharmaceutical and Biological Sciences, Félix Houphouët-Boigny University, Abidjan, Ivory Coast
Biography: Marie-Laure Hauhouot-Attoungbre, is a Pharmacist Biologist, Tenured Professor and Head of the Department of Biochemistry, Molecular Biology, and Reproductive Biology at the Faculty of Pharmacy and Biological Sciences of Félix Houphouët-Boigny University. She earned her doctorate in pharmacy in 1991 from the University of Cocody (Abidjan, Ivory Caost) and her PhD in 2002 from Lyon 1 University (France). Ms. Hauhouot is the Head of the Medical Biology Laboratory at the Abidjan Institute of Cardiology since 1998. She is a founding member and current president of the Ivorian Society of Clinical Biochemistry and a founding member of the Ivorian Fertility Working Group (GEFCI). She has participated in numerous national and international research projects in medical biology.
Research Fields: Clinical Biology, Molecular Biology, Reproductive Biology, sickle cell disease, nutrition, cardiovascular risks, biomarkers of renal function in Ivorians

Information