Oncology Department, Xi'an International Medical Center Hospital, Xi'an, China. Sapporo High Functioning Radiotherapy Center, Sapporo Kojinkai Memorial Hospital, Sapporo, Japan
Rhabdomyosarcoma (RMS) is a common malignant soft tissue tumor in children and adolescents. Usually, the incidence of mediastinal RMS is extremely low. Traditional radiotherapy causes great damage to normal tissues around the tumor. Proton beams have a unique Bragg peak that can significantly reduce damage to the surrounding normal tissues while ensuring sufficient dose of the tumor. We report a case of a 33-year-old Chinese female with primary mediastinal RMS, and introduce a treatment plan involving photon radiotherapy and proton beam therapy (PBT) for this rare and interesting case. The patient started to have chest tightness and shortness of breath two months prior to presentation at the local hospital. The cardiac color ultrasound showed pericardial effusion and pericardiocentesis was performed. She was discharged after the procedure. She had a Positron Emission Tomography (PET)/ Computerized Tomography (CT) examination and the results suggested mediastinal tumor and enlarged mediastinal lymph nodes and her puncture pathology through bronchoscopy showed RMS. The following month, the patient developed chest tightness and shortness of breath again. In our hospital a multidisciplinary treatment was conducted to formulate a plan for radiotherapy of the mediastinal RMS. She received the photon and proton beam therapy. After PBT, the tumor had significantly decreased in size. PBT may improve the tumor control and the patient’s quality of life with symptomatic mediastinal RMS. The present case illustrates that PBT may be also useful for cases that are difficult to treat with photon radiotherapy and surgery.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Mediastinal Rhabdomyosarcoma, Radiotherapy, Proton Beam Therapy, Case Report
1. Introduction
Primary mediastinal and cardiac tumors are rare
[1]
Suehiro S, Matsuda M, Hirata T, et al. Primary cardiac rhabdomyosarcoma developed after receiving radiotherapy for left breast cancer 18 years prior. J Cardiol Cases. 2017; Mar; 15(6): 181-183.
Chu WP. Anterior mediastinal alveolar rhabdomyosarcoma in an infant: rare site for a common paediatric tumour. Hong Kong Med J. 2013; Oct; 19(5): 458-459.
Suehiro S, Matsuda M, Hirata T, et al. Primary cardiac rhabdomyosarcoma developed after receiving radiotherapy for left breast cancer 18 years prior. J Cardiol Cases. 2017; Mar; 15(6): 181-183.
. Treatment mainly includes chemotherapy, surgery, radiotherapy, and others. Usually the treatment of RMS arising or involving the mediastinum and heart requires a multidisciplinary approach. The main treatment method is complete surgical resection, and as completely resection as possible is the main factor for a better prognosis. However, when the tumor invades surrounding vital tissues and organs, or is close to large blood vessels, it is impossible to remove it completely. Radiotherapy may be a safe and effective treatment for the mediastinal RMS that is inoperable. Conventional radiotherapy requires a dose of 40-60Gy, and usually used hyper-fractionation (1.1-Gy twice daily fractions) or standard fractionation (1.8-Gy daily fractions)
[4]
Donaldson SS, Meza J, Breneman JC, et al. Results from the IRS-IV randomized trial of hyperfractionated radiotherapy in children with rhabdomyosarcoma-a report from the IRSG. Int J Radiat Oncol Biol Phys. 2001; 51: 718-728.
. We report a case of a young patient with an unresectable large mediastinal RMS and dyspnea caused by tumor invasion of the heart. Conventional photon radiotherapy resulted in excessive doses to organs at risk (OAR) and low tumor control. Since PBT is a particle radiotherapy with excellent dose localization because of the spread-out of Bragg peak
[5]
Hsieh CE, Venkatesulu BP, Lee CH, et al. Predictors of Radiation-Induced Liver Disease in Eastern and Western Patients With Hepatocellular Carcinoma Undergoing Proton Beam Therapy. Int J Radiat Oncol Biol Phys. 2019; Sep; 105(1): 73-86.
. PBT is theoretically a better treatment option compared with photon treatment. However, the patient was in critical condition when the patient was seen. Therefore a combined photon and proton radiotherapy were used. Finally, the patient achieved a good local control. We hypothesized that if this patient had received proton therapy throughout the course, there might have a better local control. Next, we describe the clinical course of the patient here after PBT and photon treatment.
2. Case Presentation
2.1. History of Present Illness
A 33-year-old Chinese female started to have chest tightness and shortness of breath two months prior to presentation at the local hospital on September 23, 2022. The cardiac color ultrasound showed pericardial effusion and pericardiocentesis was performed. She was discharged after this procedure. On November 14, 2022, she developed symptoms of chest tightness and shortness of breath again and went back to the same hospital for puncture and drainage of pericardial effusion. She had a Positron Emission Tomography (PET)/ Computerized Tomography (CT) examination and the results suggested mediastinal tumor and enlarged mediastinal lymph nodes. On November 22, 2022, her puncture pathology through bronchoscopy showed RMS. The following month, this patient developed chest tightness and shortness of breath again. The local hospital recommended treatment by a specialized physician. The patient was referred to Sapporo Kojinkai Memorial Hospital for further treatment. A consultant in our hospital reviewed the patient's pathological slides and it was revealed RMS. A multidisciplinary treatment was conducted to formulate a plan for radiotherapy of the mediastinal RMS. This was the first patient in our hospital to receive PBT for mediastinal RMS.
2.1.1. Past Medical History
The patient had no history of smoking or alcohol consumption. When she came to our hospital, the coronavirus disease-19 (COVID-19) test was positive and she had a fevers. She denied systemic symptoms of night sweats, or unintentional weight loss.
2.1.2. Family History
The patient denied cancer in her family.
2.1.3. Physical Examination
Cardiac auscultation revealed weakened heart sounds and had no pathological murmurs. Lung auscultation revealed decreased breath sounds in the left lung and normal breath sounds in the right lung. No obvious abnormalities were found in other organs to physical examination.
2.1.4. Pathological Examination
The bronchoscopy pathological findings of the local hospital showed RMS. The pathological consultation in our hospital was also RMS. Immunohistochemical analysis showed that the tumor cells were positively stained for myogenin as well as desmin, muscle actin, myoD1 and vimentin. Immunohistochemical analysis of the tumor cells were negatively stained for CK, NapsinA, CK7, CD3, CD5, and so on. These histopathological and immunohistochemical analyses provided the tumor diagnosis as supportive of RMS.
2.1.5. Imaging Examinations
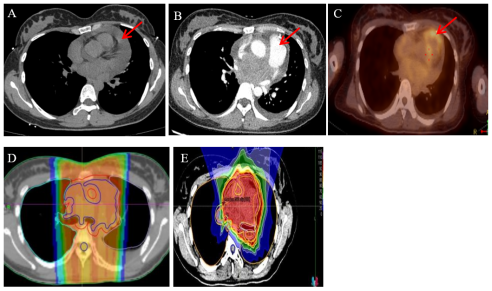
A chest CT scan performed on September 21, 2022, revealed a large tumor fused to the middle mediastinum (adjacent to the trachea and aortic arch). The fat spaces in the blood vessels around the above lesions disappeared, the right pulmonary artery and inferior vena cava were compressed, and there was severe stenosis. Moderate pericardial effusion (Figure 1A). A chest CT scan with contrast examination showed that the large tumor was fused in the middle mediastinum (around the trachea and aortic arch) that lesion was slightly larger than before and massive pericardial effusion (Figure 1B).
PET/CT revealed massive pericardial effusion, space-occupying mediastinal lesions, and high accumulation of fluorodeoxyglucose uptake. Multiple enlarged lymph nodes were observed in the anterior superior mediastinum, along with mixed-absorption shadowes and plaques in both lungs (Figure 1C). PET-CT in our hospital showed that massive pericardial effusion and a massive mediastinal tumor (red arrow Figure 1C).
Figure 1. CT scan of the chest with contrast examination showed huge mediastinal tumor and massive pericardial effusion (A&B, red arrow). PET/CT revealed massive pericardial effusion, high accumulation of FDG (C, red arrow). D and E show the planning schematic diagrams of the planned target volume using photon and proton therapy, respectively.
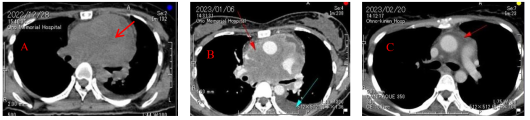
Figure 2. CT images of A and B showed before treatment, the mediastinal tumors (red arrows) were larger and compressed the great vessels of the thoracic cavity. After treatment, the tumors (C, red arrows) shrank significantly and the compression of large blood vessels in the chest was completely relieved.
2.3. Table
Table 1. Summary of case reports of rhabdomyosarcoma of the chest.
Authors
Age/Sex
Histological subtype
Treatment
Clinical course
Outcome
SatomiSuehiro, et al. 2017, Journal of Cardiology Cases
68/F
ERMS
Surgical chemotherapy radiotherapy (photon therapy) after the surgery.
The tumor growth and metastasis eight months later.
Progression disease.
SimonC. Y. Chow, et al. 2015.
Journal of Medical Case Reports
4-month/M
ARMS
Surgery chemoradiotherapy (photon therapy).
Tumor recurrence at week 39 of chemotherapy.
Died at the age of 3.
Xiang Zhou, et al. 2022, J Card Surg.
63/F
ARMS
Surgical resection, adjuvant therapy after surgery (No specific in detail).
This patient diagnosed to have mediastinal RMS. It had been 2 months since the onset of the disease. The examination revealed pericardial effusion. Since there was no adequate treatment in China, the patient and his family members sought a better treatment as soon as possible. When this patient came to our hospital, the COVID-19 test was positive, and imaging showed that massive pericardial effusion. The patient was accompanied by symptoms such as obvious chest tightness, shortness of breath and dyspnea. After admission, she was admitted to the intensive care unit (ICU) and underwent pericardial effusion puncture and drainage surgery. The pathology of the pericardial effusion showed RMS. At that time, the patient's condition was urgent and there was no indication for surgery. Palliative radiotherapy was necessary as soon as possible to relieve the patient's dyspnea and other symptoms. Because PBT in our hospital requires multidisciplinary consultation and the planning time of PBT was relatively long. In order to relieve the patient's symptoms as soon as possible, we first performed spiral tomographic radiotherapy (TOMO RT) for 3Gy per fraction x10 fractions while we were discussing multidisciplinary approach and formulating a PBT plan. After TOMO RT of 3Gy per fraction x10 fractions, the proton plan of the patient was completed and PBT of 2.3Gy ( relative biological effectiveness, (RBE)) per fraction x10 fractions were performed.
The TOMO RT for the mediastinal large vein lesion area was started on January 5, 2023. The gross target volume (GTV) included tumor that lesions visible in imaging, the clinical target volume (CTV) was defined as GTV margins of 0.2 cm, the planned target volume (PTV) was defined as CTV margins of 0.3 cm, the completed median dose for 95% PTV was 30Gy/10 fractions. On January 19, 2023, the first course of radiotherapy was finished. After completing the first course of TOMO RT, a follow-up chest CT revealed partial remission (PR) of the mediastinal lesion compared to the previous CT image scan. On January 23, 2023, radiotherapy was given to the residual mediastinal large vein lesion area, using PBT. The RBE of the PBT was assumed to be 1.1. We used the spot scattering method for PBT and the completed median dose for 95% PTV was 23Gy (RBE)/10 fractions, and a dose of 2.3Gy (RBE) every fraction. The patient underwent 4 dimension CT for respiratory motion management. The internal target volume (ITV) was contoured on the 4 dimension CT, and the PTV was defined as ITV margins of 0.5 cm. The 130 to 245 MeV proton beam generated by the linear accelerator and synchrotron was projected into the target area to ensure that the beam conforms to the treatment planning data. PBT finished on February 3, 2023 (Figure 1 D&E). The tumor showed a good PR after radiotherapy, with only mild acute reactions occurred, including grade 1 radiation pneumonitis and dermatitis. After PBT, the patient went to another hospital for chemotherapy. Then after chemotherapy, the patient returned to her place of residence. Follow-up in March, 2023 in Sapporo Kojinkai Memorial Hospital, mediastinal RMS evaluated as PR (Figure 2). Follow-up was conducted via telephone. During a telephone consultation in July 2023, the patient reported that a follow-up chest CT performed at a local hospital demonstrated complete remission (CR) of the lesion. However, as this was a telephone follow-up, imaging data were not available. In December 2023, the patient experienced a recurrence of the mediastinal lesion and underwent immunotherapy and systemic chemotherapy, the chemotherapy regimen included epirubicin and PD-1 inhibitors. Unfortunately, the patient passed away in September 2024 due to a myocardial infarction. The local hospital considered the myocardial infarction to be primarily related to the use of multi-cycle chemotherapy and immunotherapy drugs, such as: epirubicin, and so on.
All procedures performed in this case were in accordance with the ethical standards of the institutional and/or national research committee and the Declaration of Helsinki (revised in 2013). Written informed consent was obtained from the legally authorized representative to publish the anonymous patient information in this article. The reporting of this study conforms to CARE guidelines
[7]
Gagnier JJ, Kienle G, Altman DG, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. Headache. 2013; 53: 1541-1547.
The present case report describes a rare case of mediastinal RMS in adult. Given the rarity of the condition worldwide, and particularly in our setting in China. The incidence of soft tissue sarcomas in children and adolescents younger than 20 years of age is represented 7.4% of cancer cases for this age group
[8]
Ries LAG, Smith MA, Gurney JG, et al. Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975-1995, National Cancer Institute, SEER Program. 1999, NIH Pub. No. 99-4649.
[9]
Takizawa D, Oshiro Y, Mizumoto M, et al. Proton beam therapy for a patient with large rhabdomyosarcoma of the body trunk. Ital J Pediatr. 2015; Nov; 41: 90.
. RMS is the most common soft tissue sarcoma in children aged 0-14 years. But its incidence rate in adults is relatively low. The incidence of RMS within primary mediastinal tumors is very low
[3]
Blondeau P. Primary cardiac tumors-French studies of 533 cases. Thorac Cardiovasc Surg. 1990; 38(Suppl. 2): 192-195.
. In this report, we discuss the rarity of this particular condition, the literature surrounding similar reports, and the many challenges that arise in the management of adult mediastinal RMS. Given the rarity of adult RMS, clear guidelines for management are lacking.
Multimodality therapy including chemotherapy, radiotherapy, surgery and others, may be available, but the efficacy has not been optimistic. Radiotherapy may be a safe and effective treatment for the mediastinum RMS. Conventional photon radiotherapy causes greater damage to surrounding normal tissues. Considering that the patient's tumor is located in the mediastinum area, proton beams have unique physical advantages: Bragg peak, releases less energy when passing through normal tissues then releases a large amount of energy instantly when reaching the tumor, and the dose drops rapidly after the tumor target. PBT can ensure that a large dose of radiation is delivered to the tumor while reducing the radiation dose to normal tissues. Therefore, compared with photon radiotherapy, PBT can greatly reduce the dose to surrounding normal tissues while ensuring the same radiation dose to the tumor target. Based on these advantages of PBT, some radiotherapy centers treated many patients with liver, prostate and lung cancers. Several studies
[10]
Mizumoto M, Ogino H, Okumura T, et al. Proton Beam Therapy for Hepatocellular Carcinoma: Multicenter Prospective Registry Study in Japan. Int J Radiat Oncol Biol Phys. 2024; Mar; 118(3): 725-733.
Iwata H, Ogino H, Hattori Y, et al. A Phase 2 Study of Image-Guided Proton Therapy for Operable or Ablation-Treatable Primary Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys. 2021; Sep; 111(1): 117-126.
have reported the advantages of PBT compared with photon radiotherapy (including Intensity-Modulated Radiation Therapy (IMRT)). Zhongxing liao et al. found that proton beams significantly reduced heart exposure in terms of both radiation dose and heart volume, and its influence on cardiac toxicity and overall survival was under active investigation, compared to IMRT in radiotherapy for lung cancer
[12]
Zhongxing Liao, J. Jack Lee, Komaki R, et al. Adaptive Randomization Trial of Passive Scattering Proton Therapy and Intensity-Modulated Photon Radiotherapy for Locally Advanced Non-Small-Cell Lung Cancer. J Clin Oncol. 2018; Jun; 36(18): 1813-1822.
. After reviewing the relevant literatures, there were few reports of adult mediastinal RMS, and most of them were case reports. There were no reports on the use of PBT for adult mediastinal RMS, and only a few cases have been reported using surgery, chemotherapy, or photon radiotherapy. We only found four reports on mediastinal RMS, which are summarized in Table 1.
[1]
Suehiro S, Matsuda M, Hirata T, et al. Primary cardiac rhabdomyosarcoma developed after receiving radiotherapy for left breast cancer 18 years prior. J Cardiol Cases. 2017; Mar; 15(6): 181-183.
Nishii Y, Sasaki J, Sudou M, et al. Pazopanib for treating rhabdomyosarcoma in adult patients with poor performance status: A case report. Thorac Cancer. 2022; Nov; 13(21): 3080-3083.
Chow SC, Wong RH, Wan IY, et al. Alveolar rhabdomyosarcoma of the anterior mediastinum with vessel invasion in a 4-month-old boy: a case report. J Med Case Rep. 2015; Jul; 9: 157.
One case involved an infant, while three cases involved adults. There was a retrospective report on PBT for RMS in pediatric patients, in this report there were only 10 cases of pediatric RMS occurring in the chest. The unique depth-dose characteristics of protons can be exploited to achieve significant reductions in normal tissue doses and may allow an escalation of tumor doses and greater sparing of normal tissues, thus potentially improving local control while at the same time reducing toxicity and improving quality of life
[16]
Vennarini S, Colombo F, Mirandola A, et al. Clinical Insight on Proton Therapy for Paediatric Rhabdomyosarcoma. Cancer Manag Res. 2023; Oct; 15: 1125-1139.
Martin-Giacalone BA, Li H, Scheurer ME, et al. Germline Genetic Testing and Survival Outcomes Among Children With Rhabdomyosarcoma: A Report From the Children's Oncology Group. JAMA Netw Open. 2024; Mar; 7(3): e244170.
Yock T, Schneider R, Friedmann A, et al. Proton radiotherapy for orbital rhabdomyosarcoma: clinical outcome and a dosimetric comparison with photons. Int J Radiat Oncol Biol Phys. 2005; Nov; 63(4): 1161-1168.
. PBT has better efficacy and lower complications than photon therapy in pediatric RMS. RMS among children is more radiosensitive compared with RMS among adults. Our hospital conducted a multidisciplinary discussion. The result was that the patient was a young female and the pathological type was mediastinal RMS, which was very rare. Currently, in order to resolve the patient's main symptoms, palliative radiotherapy can be performed to relieve the patient's symptoms. We believed that PBT is correct and may be effective in this case, although we have not used this combined therapy approach before for mediastinal RMS, which extensively invades the aorta and large veins. In this case, we used a combined approach of photon and proton therapy due to the reality at that time. For the comparison of the two radiotherapy methods, we found that spot scanning PBT was more tolerated for mediastinal RMS and showed that IMRT plans were inferior to PBT. The specific doses for PBT and IMRT will be elaborated in the following section. Therefore, PBT can reduce the dose to the volume around the target, thereby reducing the risk of secondary cancers. In a phase II study comparing PBT and IMRT, Ladra et al. reported favorable disease control and dose distribution
[19]
Ladra MM, Szymonifka JD, Mahajan A, et al. Preliminary results of a phase II trial of proton radiotherapy for pediatric rhabdomyosarcoma. J Clin Oncol. 2014; 32: 3762-3770.
When the patient came to our hospital, she was infected with the COVID-19 and developed symptoms such as difficulty breathing, chest tightness and shortness of breath. She was admitted to the ICU for pericardiocentesis and drainage surgery. Considering that the PBT plan takes a long time, TOMO RT will be given first, and PBT will be carried out after it is completed. In the TOMO treatment plan, the D95 (dose received by 95% of the volume) of PTV was 29.27Gy (reaching 98% of the prescribed dose), while the D95 of PTV in the PBT was 22.02Gy (RBE) (reaching 96% of the prescribed dose). Both datas were consistent with treatment plan requirements. The maximum point dose of TOMO RT in the heart was 30.63Gy, compared with 23.50Gy (RBE) for PBT. The maximum point dose of TOMO RT for the left lung was 30.68Gy, compared with 22.96Gy (RBE) for PBT. The maximum point dose of TOMO RT for the right lung was 30.05Gy, compared with 20.67Gy (RBE) for PBT. In present case, the D99, D98 and D95 (D99: dose received by 99% of the volume; D98: dose received by 98% of the volume; D95: dose received by 95% of the volume) of cardiac in TOMO RT and PBT were 53, 57, 67cGy and 11, 13, 17cGy (RBE), respectively. The D99, D98 and D95 of left lung were 58, 72, 111cGy and 0, 1, 3cGy (RBE), respectively. The D99, D98 and D95 of right lung were 33, 36, 43cGy and 1, 3, 7cGy (RBE), respectively. It can be seen that the dose of PBT for organs at risk were significantly lower than that of photon therapy. The patient had no obvious discomfort symptoms such as nausea, vomiting, and palpitation during the treatment. After the treatment, the patient's chest tightness and shortness of breath disappeared. Follow-up chest CT showed significant shrinkage of the mediastinal RMS. A follow-up examination 1 month after the end of treatment showed that the lesion was continuously shrank on chest CT. A follow up examination 6 months after the completion of radiotherapy showed CR of the lesion.
This was the only report of mediastinal RMS in adults treated with both photons and protons. Although this patient underwent TOMO RT first and PBT later due to the emergency situation, we can be seen from the proton plan that the doses of organs at risk were significantly better than the TOMO plan. During the treatment, there was only mild dermatitis and fatigue, and no other obvious symptoms of discomfort maybe because of the later use of proton therapy. It was a successful case of trying to use proton and photon to collaboratively treat mediastinal RMS. It is worthy of continued follow-up and research in the future to provide treatment reference for similar patients.
5. Conclusions
This report describes a rare case of a mediastinal RMS using photon and proton therapy. It is relatively rare with a poor prognosis. Through radiotherapy combined with subsequent adjuvant chemotherapy, the patient achieved CR six months after radiotherapy. However, recurrence occurred one year after radiotherapy. This indicates the need for further research and optimization of treatment protocols to prolong the remission period and reduce the recurrence rate. Given the rarity of the disease, exploring novel treatment approaches, as part of a comprehensive treatment strategy may improve therapeutic outcomes. Additionally, investigating the mechanisms and causes of recurrence in this patient could aid in developing more effective prevention and treatment strategies to minimize the risk of recurrence.
Abbreviations
RMS
Rhabdomyosarcoma
PBT
Proton Beam Therapy
PET
Positron Emission Tomography
CT
Computerized Tomography
COVID-19
Coronavirus Disease-19
ICU
Intensive Care Unit
GTV
Ross Target Volume
CTV
Clinical Target Volume
PTV
Planned Target Volume
PR
Partial Remission
CR
Complete Remission
RBE
Relative Biological Dose
Acknowledgments
The authors wish to thank Ritsuko Komaki for reviewing the manuscript.
Availability of Data and Materials
The datasets used in the current study are available from the corresponding author on reasonable request.
Declarations
Ethics Approval and Consent to Participate
In accordance with the local guidelines, the Ethics Committee of Sapporo Medical did not require ethical approval for this study. However, this study complied with the guidelines for human studies and was conducted ethically, and in accordance with the guidelines set forth in the Declaration of Helsinki, written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. Moreover, the authors have no ethical conflicts to disclose.
Consent for Publication
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
Wencui Yang wrote the paper, Junetsu Mizoe provided the research data.
Funding
This study was supported by Xi’an International Medical Center Hospital, No. 2023QN011.
Competing interests
The authors have no competing interests to declare.
References
[1]
Suehiro S, Matsuda M, Hirata T, et al. Primary cardiac rhabdomyosarcoma developed after receiving radiotherapy for left breast cancer 18 years prior. J Cardiol Cases. 2017; Mar; 15(6): 181-183.
Chu WP. Anterior mediastinal alveolar rhabdomyosarcoma in an infant: rare site for a common paediatric tumour. Hong Kong Med J. 2013; Oct; 19(5): 458-459.
Donaldson SS, Meza J, Breneman JC, et al. Results from the IRS-IV randomized trial of hyperfractionated radiotherapy in children with rhabdomyosarcoma-a report from the IRSG. Int J Radiat Oncol Biol Phys. 2001; 51: 718-728.
Hsieh CE, Venkatesulu BP, Lee CH, et al. Predictors of Radiation-Induced Liver Disease in Eastern and Western Patients With Hepatocellular Carcinoma Undergoing Proton Beam Therapy. Int J Radiat Oncol Biol Phys. 2019; Sep; 105(1): 73-86.
Ries LAG, Smith MA, Gurney JG, et al. Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975-1995, National Cancer Institute, SEER Program. 1999, NIH Pub. No. 99-4649.
[9]
Takizawa D, Oshiro Y, Mizumoto M, et al. Proton beam therapy for a patient with large rhabdomyosarcoma of the body trunk. Ital J Pediatr. 2015; Nov; 41: 90.
Mizumoto M, Ogino H, Okumura T, et al. Proton Beam Therapy for Hepatocellular Carcinoma: Multicenter Prospective Registry Study in Japan. Int J Radiat Oncol Biol Phys. 2024; Mar; 118(3): 725-733.
Iwata H, Ogino H, Hattori Y, et al. A Phase 2 Study of Image-Guided Proton Therapy for Operable or Ablation-Treatable Primary Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys. 2021; Sep; 111(1): 117-126.
Nishii Y, Sasaki J, Sudou M, et al. Pazopanib for treating rhabdomyosarcoma in adult patients with poor performance status: A case report. Thorac Cancer. 2022; Nov; 13(21): 3080-3083.
Chow SC, Wong RH, Wan IY, et al. Alveolar rhabdomyosarcoma of the anterior mediastinum with vessel invasion in a 4-month-old boy: a case report. J Med Case Rep. 2015; Jul; 9: 157.
Vennarini S, Colombo F, Mirandola A, et al. Clinical Insight on Proton Therapy for Paediatric Rhabdomyosarcoma. Cancer Manag Res. 2023; Oct; 15: 1125-1139.
Martin-Giacalone BA, Li H, Scheurer ME, et al. Germline Genetic Testing and Survival Outcomes Among Children With Rhabdomyosarcoma: A Report From the Children's Oncology Group. JAMA Netw Open. 2024; Mar; 7(3): e244170.
Yock T, Schneider R, Friedmann A, et al. Proton radiotherapy for orbital rhabdomyosarcoma: clinical outcome and a dosimetric comparison with photons. Int J Radiat Oncol Biol Phys. 2005; Nov; 63(4): 1161-1168.
Ladra MM, Szymonifka JD, Mahajan A, et al. Preliminary results of a phase II trial of proton radiotherapy for pediatric rhabdomyosarcoma. J Clin Oncol. 2014; 32: 3762-3770.
Wencui, Y., Junetsu, M. (2025). Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report. American Journal of Clinical and Experimental Medicine, 13(4), 84-90. https://doi.org/10.11648/j.ajcem.20251304.13
Wencui, Y.; Junetsu, M. Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report. Am. J. Clin. Exp. Med.2025, 13(4), 84-90. doi: 10.11648/j.ajcem.20251304.13
Wencui Y, Junetsu M. Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report. Am J Clin Exp Med. 2025;13(4):84-90. doi: 10.11648/j.ajcem.20251304.13
@article{10.11648/j.ajcem.20251304.13,
author = {Yang Wencui and Mizoe Junetsu},
title = {Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report
},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {4},
pages = {84-90},
doi = {10.11648/j.ajcem.20251304.13},
url = {https://doi.org/10.11648/j.ajcem.20251304.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251304.13},
abstract = {Rhabdomyosarcoma (RMS) is a common malignant soft tissue tumor in children and adolescents. Usually, the incidence of mediastinal RMS is extremely low. Traditional radiotherapy causes great damage to normal tissues around the tumor. Proton beams have a unique Bragg peak that can significantly reduce damage to the surrounding normal tissues while ensuring sufficient dose of the tumor. We report a case of a 33-year-old Chinese female with primary mediastinal RMS, and introduce a treatment plan involving photon radiotherapy and proton beam therapy (PBT) for this rare and interesting case. The patient started to have chest tightness and shortness of breath two months prior to presentation at the local hospital. The cardiac color ultrasound showed pericardial effusion and pericardiocentesis was performed. She was discharged after the procedure. She had a Positron Emission Tomography (PET)/ Computerized Tomography (CT) examination and the results suggested mediastinal tumor and enlarged mediastinal lymph nodes and her puncture pathology through bronchoscopy showed RMS. The following month, the patient developed chest tightness and shortness of breath again. In our hospital a multidisciplinary treatment was conducted to formulate a plan for radiotherapy of the mediastinal RMS. She received the photon and proton beam therapy. After PBT, the tumor had significantly decreased in size. PBT may improve the tumor control and the patient’s quality of life with symptomatic mediastinal RMS. The present case illustrates that PBT may be also useful for cases that are difficult to treat with photon radiotherapy and surgery.},
year = {2025}
}
TY - JOUR
T1 - Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report
AU - Yang Wencui
AU - Mizoe Junetsu
Y1 - 2025/07/23
PY - 2025
N1 - https://doi.org/10.11648/j.ajcem.20251304.13
DO - 10.11648/j.ajcem.20251304.13
T2 - American Journal of Clinical and Experimental Medicine
JF - American Journal of Clinical and Experimental Medicine
JO - American Journal of Clinical and Experimental Medicine
SP - 84
EP - 90
PB - Science Publishing Group
SN - 2330-8133
UR - https://doi.org/10.11648/j.ajcem.20251304.13
AB - Rhabdomyosarcoma (RMS) is a common malignant soft tissue tumor in children and adolescents. Usually, the incidence of mediastinal RMS is extremely low. Traditional radiotherapy causes great damage to normal tissues around the tumor. Proton beams have a unique Bragg peak that can significantly reduce damage to the surrounding normal tissues while ensuring sufficient dose of the tumor. We report a case of a 33-year-old Chinese female with primary mediastinal RMS, and introduce a treatment plan involving photon radiotherapy and proton beam therapy (PBT) for this rare and interesting case. The patient started to have chest tightness and shortness of breath two months prior to presentation at the local hospital. The cardiac color ultrasound showed pericardial effusion and pericardiocentesis was performed. She was discharged after the procedure. She had a Positron Emission Tomography (PET)/ Computerized Tomography (CT) examination and the results suggested mediastinal tumor and enlarged mediastinal lymph nodes and her puncture pathology through bronchoscopy showed RMS. The following month, the patient developed chest tightness and shortness of breath again. In our hospital a multidisciplinary treatment was conducted to formulate a plan for radiotherapy of the mediastinal RMS. She received the photon and proton beam therapy. After PBT, the tumor had significantly decreased in size. PBT may improve the tumor control and the patient’s quality of life with symptomatic mediastinal RMS. The present case illustrates that PBT may be also useful for cases that are difficult to treat with photon radiotherapy and surgery.
VL - 13
IS - 4
ER -
Oncology Department, Xi'an International Medical Center Hospital, Xi'an, China. Sapporo High Functioning Radiotherapy Center, Sapporo Kojinkai Memorial Hospital, Sapporo, Japan
Wencui, Y., Junetsu, M. (2025). Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report. American Journal of Clinical and Experimental Medicine, 13(4), 84-90. https://doi.org/10.11648/j.ajcem.20251304.13
Wencui, Y.; Junetsu, M. Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report. Am. J. Clin. Exp. Med.2025, 13(4), 84-90. doi: 10.11648/j.ajcem.20251304.13
Wencui Y, Junetsu M. Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report. Am J Clin Exp Med. 2025;13(4):84-90. doi: 10.11648/j.ajcem.20251304.13
@article{10.11648/j.ajcem.20251304.13,
author = {Yang Wencui and Mizoe Junetsu},
title = {Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report
},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {4},
pages = {84-90},
doi = {10.11648/j.ajcem.20251304.13},
url = {https://doi.org/10.11648/j.ajcem.20251304.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251304.13},
abstract = {Rhabdomyosarcoma (RMS) is a common malignant soft tissue tumor in children and adolescents. Usually, the incidence of mediastinal RMS is extremely low. Traditional radiotherapy causes great damage to normal tissues around the tumor. Proton beams have a unique Bragg peak that can significantly reduce damage to the surrounding normal tissues while ensuring sufficient dose of the tumor. We report a case of a 33-year-old Chinese female with primary mediastinal RMS, and introduce a treatment plan involving photon radiotherapy and proton beam therapy (PBT) for this rare and interesting case. The patient started to have chest tightness and shortness of breath two months prior to presentation at the local hospital. The cardiac color ultrasound showed pericardial effusion and pericardiocentesis was performed. She was discharged after the procedure. She had a Positron Emission Tomography (PET)/ Computerized Tomography (CT) examination and the results suggested mediastinal tumor and enlarged mediastinal lymph nodes and her puncture pathology through bronchoscopy showed RMS. The following month, the patient developed chest tightness and shortness of breath again. In our hospital a multidisciplinary treatment was conducted to formulate a plan for radiotherapy of the mediastinal RMS. She received the photon and proton beam therapy. After PBT, the tumor had significantly decreased in size. PBT may improve the tumor control and the patient’s quality of life with symptomatic mediastinal RMS. The present case illustrates that PBT may be also useful for cases that are difficult to treat with photon radiotherapy and surgery.},
year = {2025}
}
TY - JOUR
T1 - Proton Beam Therapy for a Patient with Mediastinal Rhabdomyosarcoma: A Case Report
AU - Yang Wencui
AU - Mizoe Junetsu
Y1 - 2025/07/23
PY - 2025
N1 - https://doi.org/10.11648/j.ajcem.20251304.13
DO - 10.11648/j.ajcem.20251304.13
T2 - American Journal of Clinical and Experimental Medicine
JF - American Journal of Clinical and Experimental Medicine
JO - American Journal of Clinical and Experimental Medicine
SP - 84
EP - 90
PB - Science Publishing Group
SN - 2330-8133
UR - https://doi.org/10.11648/j.ajcem.20251304.13
AB - Rhabdomyosarcoma (RMS) is a common malignant soft tissue tumor in children and adolescents. Usually, the incidence of mediastinal RMS is extremely low. Traditional radiotherapy causes great damage to normal tissues around the tumor. Proton beams have a unique Bragg peak that can significantly reduce damage to the surrounding normal tissues while ensuring sufficient dose of the tumor. We report a case of a 33-year-old Chinese female with primary mediastinal RMS, and introduce a treatment plan involving photon radiotherapy and proton beam therapy (PBT) for this rare and interesting case. The patient started to have chest tightness and shortness of breath two months prior to presentation at the local hospital. The cardiac color ultrasound showed pericardial effusion and pericardiocentesis was performed. She was discharged after the procedure. She had a Positron Emission Tomography (PET)/ Computerized Tomography (CT) examination and the results suggested mediastinal tumor and enlarged mediastinal lymph nodes and her puncture pathology through bronchoscopy showed RMS. The following month, the patient developed chest tightness and shortness of breath again. In our hospital a multidisciplinary treatment was conducted to formulate a plan for radiotherapy of the mediastinal RMS. She received the photon and proton beam therapy. After PBT, the tumor had significantly decreased in size. PBT may improve the tumor control and the patient’s quality of life with symptomatic mediastinal RMS. The present case illustrates that PBT may be also useful for cases that are difficult to treat with photon radiotherapy and surgery.
VL - 13
IS - 4
ER -