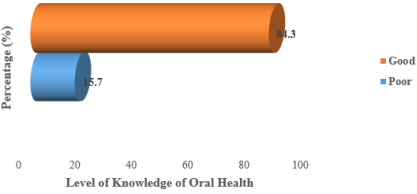
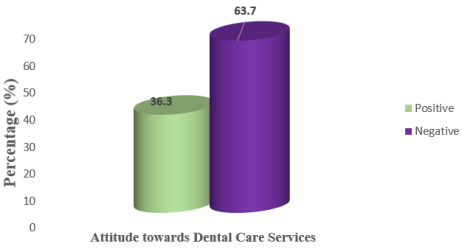
Oral health is an essential component of overall health and quality of life; however, utilisation of professional dental care services remains low in many rural communities in Nigeria. Knowledge and attitudes toward dental care are key determinants of service utilisation, particularly in underserved populations. This study assessed the knowledge, attitudes, and utilisation of professional dental care services among rural residents of Ikwerre Local Government Area, Rivers State, Nigeria. Method: A community-based cross-sectional study was conducted among 300 rural residents selected using multistage sampling. Data were collected using a structured interviewer-administered questionnaire. Descriptive statistics were used to summarize respondents’ knowledge, attitudes, and utilisation of dental care services, while Chi-square tests were used to examine associations between socio-demographic characteristics and knowledge and attitudes. Statistical significance was set at p < 0.05. Result: Most respondents demonstrated good knowledge of oral/dental health (84.3%). Despite this, attitudes toward dental care utilisation were largely negative, with 63.7% of respondents exhibiting unfavourable attitudes. Utilisation of professional dental care services was generally low and largely symptom-driven. Sex and monthly income were significantly associated with knowledge of oral/dental health (p < 0.05). Attitude toward dental care utilisation was significantly associated with level of education, occupation, and monthly income (p < 0.001), while age, marital status, and sex showed no significant association. Conclusion: Although knowledge of oral health was relatively high among rural residents of Ikwerre Local Government Area, negative attitudes toward dental care and low utilisation of professional services persist. Socioeconomic factors play a significant role in shaping attitudes and knowledge, underscoring the need for targeted oral health education, attitude-focused interventions, and improved accessibility and affordability of dental services in rural communities.
| Published in | American Journal of Health Research (Volume 14, Issue 2) |
| DOI | 10.11648/j.ajhr.20261402.11 |
| Page(s) | 65-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Oral Health, Dental Care Utilisation, Attitude, Knowledge, Rural Population, Ikwerre LGA
Variables | Knowledge of Oral/dental health | <i></i>2 | p-value | |
|---|---|---|---|---|
Good n (%) | Poor n (%) | |||
Age (in years) | ||||
18-32 | 63 (24.9) | 15 (31.9) | 4.753 | 0.189 |
33-47 | 94 (37.2) | 11 (23.4) | ||
48-62 | 67 (26.5) | 12 (25.5) | ||
63-77 | 29 (11.5) | 9 (19.1) | ||
Marital Status | ||||
Not currently married | 101 (39.9) | 13 (27.7) | 2.529 | 0.141 |
Married | 152 (60.1) | 34 (72.3) | ||
Sex | ||||
Male | 112 (44.3) | 10 (21.3) | 8.684 | 0.003* |
Female | 141 (55.7) | 37 (78.7) | ||
Level of Education | ||||
No formal education | 49 (19.4) | 10 (21.3) | 4.591 | 0.204 |
Primary | 59 (23.3) | 14 (29.8) | ||
Secondary | 114 (45.1) | 22 (46.8) | ||
Tertiary | 31 (12.3) | 1 (2.1) | ||
Occupation | ||||
Unemployed | 25 (9.9) | 7 (14.9) | 5.166 | 0.272 |
Farmer | 86 (34.0) | 16 (34.0) | ||
Business | 66 (26.1) | 10 (21.3) | ||
Formal Employment | 32 (12.6) | 2 (4.3) | ||
Artisans | 44 (17.4) | 12 (25.5) | ||
Monthly Income | ||||
<₦20,000 | 83 (32.8) | 14 (36.6) | 7.940 | 0.045* |
₦20,000–₦49,999 | 96 (37.9) | 26 (45.5) | ||
₦50,000–₦99,999 | 55 (21.8) | 3 (6.4) | ||
₦100,000 and above | 19 (7.5) | 4 (8.5) | ||
Variables | Attitude towards utilisation of dental care services | 2 | p-value | |
|---|---|---|---|---|
Positive n (%) | Negative n (%) | |||
Age (in years) | ||||
18-32 | 27 (24.8) | 51 (26.7) | 5.268 | 0.154 |
33-47 | 37 (33.9) | 68 (35.6) | ||
48-62 | 25 (22.9) | 54 (28.3) | ||
63-77 | 20 (18.4) | 18 (9.4) | ||
Marital Status | ||||
Not currently married | 43 (39.4) | 71 (37.2) | 0.153 | 0.712 |
Married | 66 (60.6) | 120 (62.8) | ||
Sex | ||||
Male | 46 (42.2) | 76 (39.8) | 0.167 | 0.715 |
Female | 63 (57.8) | 115 (60.2) | ||
Level of Education | ||||
No formal education | 13 (11.9) | 46 (24.0) | 32.941 | <0.001 |
Primary | 19 (17.4) | 54 (28.3) | ||
Secondary | 52 (47.7) | 84 (44.0) | ||
Tertiary | 25 (22.9) | 7 (3.7) | ||
Occupation | ||||
Unemployed | 6 (5.5) | 26 (13.6) | 19.418 | <0.001 |
Farmer | 33 (30.3) | 69 (36.1) | ||
Business | 27 (24.8) | 49 (25.7) | ||
Formal Employment | 23 (21.1) | 11 (5.8) | ||
Artisans | 20 (18.3) | 36 (18.8) | ||
Monthly Income | ||||
<₦20,000 | 27 (24.8) | 70 (36.6) | 24.436 | <0.001 |
₦20,000–₦49,999 | 35 (32.1) | 87 (45.5) | ||
₦50,000–₦99,999 | 31 (28.4) | 27 (14.1) | ||
₦100,000 and above | 16 (14.7) | 7 (3.7) | ||
Variables | Percentage (%) | Cumulative Percentage | |
|---|---|---|---|
Dental visit within the past 1 year | Frequency (n=300) | ||
Yes | 47 | 15.7 | 15.7 |
No | 253 | 84.3 | 100 |
Frequency of Dental Visits | (n=47) | ||
Only if I have a dental problem | 30 | 63.8 | 63.8 |
Once every 6 months | 7 | 14.9 | 78.7 |
Once every year | 10 | 21.3 | 100 |
LGA | Local Government Area |
KL | Knowledge Level |
WHO | World Health Organisation |
| [1] | Abodunrin, O. R., Adebayo, E. T., Adewole, I. E., Olagunju, M. T., Ekeh, C., Samuel, I. O., Zamba, E., Gbaja-Biamila, T., Akinsolu, F. T., Eleje, G. U., Tantawi, M. E., Ezechi, O. C., Foláyan, M. O. Factors associated with the dental service utilisation by enrollees on the Lagos State health insurance scheme, Nigeria. BMC Health Services Research. 2025, 25(1), 14. |
| [2] | Akinboboye, B. O., Malomo, B. I., Gbiri, C. A., Ogunyemi, A. O., Arikawe, A. P., Obashoro-John, O. A. Oral health literacy: effectiveness of a homegrown intervention among community-dwelling older Nigerians. BMC oral health. 2025, 25(1), 1119. |
| [3] | Akwiwu, U. N., & Orbunde, A. K. (2025). Determinants of food consumption patterns in rural households of Ikwerre Local Government Area, Rivers State, Nigeria. Journal of Food Stability, 8(3), 17-31. |
| [4] | Alshammari, R. M., Aljelaly, H. W., Almutair, T. J., Alarfaj, N. A., Alhamami, A. A., Alsomali, E. A., & Alzahrani, J. S. Integrating preventive care strategies in routine dental practice. International Journal of Community Med Public Health. 2024, 11, 4119-4122. |
| [5] | Amedari, M. I., Ogunbodede, E. O., Owotade, F. J., Afolabi, T. O., Amedari, I. K., & Mudasiru, T. O. (2024). A mixed-methods study of the oral health knowledge and practice of community health practitioners. Niger Journal of Health Sciences, 23(2), 7-15. |
| [6] | Asiri, A., Nazir, M. A., Alsharief, M., Shahin, S., Al-Ansari, A., & Al-Khalifa, K. S. (2024). Effect of psychological distress on oral health: a cross-sectional study. BMC oral health, 24(1), 1508. |
| [7] | Balcoș, C., Bamboi, I., Toader, A., Rapis, A., Nicolau, A., Cămăruță, R., & Armencia, A. O. (2025). FACTORS INFLUENCING THE PERCEPTION OF THE NEED FOR DENTAL TREATMENT AMONG THE ADULT POPULATION IN NORTHEASTERN ROMANIA. Romanian Journal of Medical and Dental Education, 14(3). |
| [8] | Chauca-Bajaña, L., Pérez-Jardón, A., Carpio-Cevallos, C., Ordoñez Balladares, A., Proaño-Yela, P., Velásquez Ron, B., Siguencia Suarez, L. J., Romo Olvera, C. V., Orellana Guerrero, D., & Pérez-Sayáns, M. (2025). Factors associated with dental anxiety in patients treated at an integrated dental clinic: a cross-sectional study. Frontiers in oral health, 6, 1689805. |
| [9] | Chen, X., Cheng, L., Chen, Y., & Xie, Y. (2026). Oral Healthcare Knowledge, Attitudes, Confidence, and Learning Experiences among Chinese Nursing Students: A Mixed-Methods Study. International dental journal, 76(1), 103994. |
| [10] | Chikuni, W., Amalimeh, B. E., & Agholor, C. N. (2023). Utilisation of oral health services and associated factors in a suburban population in Western Uganda. International Journal of Medical Sciences and Pharma Research, 9(2), 1-12. |
| [11] | Denis, F., & Clement, C. (2025). Oral Health: A Major Global Public Health Concern. Journal of Clinical Medicine, 14(12), 4101. |
| [12] | Do, L. H. M., Dimitropoulos, Y., Biles, J., Christian, B., & Sohn, W. (2025). Employment experiences of the oral health workforce in rural New South Wales: a qualitative study. BMC Health Services Research, 25(1), 922. |
| [13] | Echeverria, M. S., Borges, R. D. C., Karam, S. A., Haubert, G., Cademartori, M. G., Agostini, B. A., & Demarco, F. F. (2025). Oral Health Outcomes and Their Sociodemographic and Service Utilisation Determinants in a Rural Population. Community Dentistry and Oral Epidemiology. |
| [14] | Folayan, M. O., Bernard, O. T., Titus, O. S., Alade, O., Aliyu, T. K., Bhayat, A., Ndembi, N., Fasiku, G., & El Tantawi, M. (2025). Cultural practices, oral health service utilisation and oral health policy and guidelines development in Africa. Frontiers in oral health, 6, 1539827. |
| [15] | Folorunsho, S., Ajayi, V., Sanmori, M., Suleiman, M., Abdullateef, R., & Abdulganiyu, A. (2025). Access to and Utilisation of Dental Care Services by Older Adults in Nigeria: Barriers and Facilitators. Special Care in Dentistry, 45(3), e70040. |
| [16] | Ghoneim, A., Ebnahmady, A., D'Souza, V., Parbhakar, K. K., He, H., Gerbig, M., Singhal, S., & Quiñonez, C. (2022). The impact of dental care programs on healthcare system and societal outcomes: a scoping review. BMC Health Services Research, 22(1), 1574. |
| [17] | Hannan, C. J., Ricks, T. L., Espinoza, L., & Weintraub, J. A. (2021). Addressing Oral Health Inequities, Access to Care, Knowledge, and Behaviors. Preventing chronic disease, 18, E27. |
| [18] | IKPEFAN, D. O., ERHABOR, P., & AZODO, C. C. (2020). Oral Health Awareness and Care Seeking Behaviours among Public and Private Dental Clinics Attendees: Oral Health Awareness and Care Seeking Behaviours among Dental Clinics Attendees. Nigerian Journal of Dental Sciences, 3(1), 9-15. |
| [19] | Inoue, Y., Zaitsu, T., Oshiro, A., Ishimaru, M., Taira, K., Takahashi, H., Aida, J., & Tamiya, N. (2022). Association of marital status and access to dental care among the Japanese population: a cross-sectional study. BMC oral health, 22(1), 278. |
| [20] | Joseph, C. C., & Akaji, E. A. (2022). Utilisation of Dental Services by Rural dwellers: Case of two Communities hosting a tertiary health facility. International Journal of Dentistry Research, 7(1), 19-27. |
| [21] | Kaguru, G., Ayah, R., Mutave, R., & Mugambi, C. (2022). Integrating Oral Health into Primary Health Care: A Systematic Review of Oral Health Training in Sub-Saharan Africa. Journal of multidisciplinary healthcare, 15, 1361–1367. |
| [22] | Mariam, R., Rafique, M. H., Soomro, A. H., Abu Kariem, A., Jarbou, R., Ibrar, A., & Obied, B. (2025). Effect of Dental Fear on Delay in Seeking Dental Treatment among Adults in a South Asian Setting. Cureus, 17(7), e87540-e87540. |
| [23] | Márquez-Arrico, C. F., Almerich-Silla, J. M., & Montiel-Company, J. M. (2019). Oral health knowledge in relation to educational level in an adult population in Spain. Journal of clinical and experimental dentistry, 11(12), e1143–e1150. |
| [24] | Musa, A., Mala, A. K., Adetoye, J., Uchenna, K., Abba, U., & Abdullahi, I. S. (2024). Determinants of Oral Health Knowledge and Practice among Internally Displaced Persons in Maiduguri, Borno State, Nigeria. African Journal of Health and Social Sciences, 1(2), 69-77. |
| [25] | Nigeria Population Commission. (2006). Nigeria demographic and health survey 2006. NPC, ICF. |
| [26] | Northridge, M. E., Kumar, A., Kaur, R. Disparities in Access to Oral Health Care. Annual review of public health. 2020, 41, 513–535. |
| [27] | Nota, A., Caruso, S., Cantile, T., Gatto, R., Ingenito, A., Tecco, S., Ferrazzano, G. F. Socioeconomic Factors and Oral Health-Related Behaviours Associated with Dental Caries in Preschool Children from Central Italy (Province of Ascoli Piceno). Biomedical research international. 2019, 7981687. |
| [28] | Nzabonimana, E., Malele-Kolisa, Y., Hlongwa, P. Oral health knowledge, attitude and oral hygiene practices among adults in Rwanda. PAMJ Clinical Medicine. 2024, 14(4). |
| [29] | Okoroafor, C. C., Okobi, O. E., Owodeha-Ashaka, M., Okobi, E., Oluseye, B., Ekpang, O. B., Aya, L. E., Owolabi, O. J., Oru-Betem, T. E., Nwafor, J. N. Dental Health Knowledge, Attitude, and Practice among University of Calabar Students. Cureus. 2023, 15(6), e40055. |
| [30] | Olatosi, O. O., Oyapero, A., Ashaolu, J. F., Abe, A., & Boyede, G. O. (2022). Dental caries and oral health: an ignored health barrier to learning in Nigerian slums: a cross-sectional survey. PAMJ-One Health, 7(13). |
| [31] | Opoku, P., Salu, S., Azornu, C. K., & Komesuor, J. (2024). Oral health knowledge, practice, and associated factors among Junior High School students of Koforidua, Ghana: a cross-sectional study. BMC Oral Health, 24(1), 449. |
| [32] | Osadolor, O. O., Akaji, E. A., Otakhoigbogie, U., Amuta, H. C., Obi, D. I., & Osadolor, A. J. Dental service utilisation of a rural population in Nigeria. International Journal Dentistry Research. 2019, 4(2), 62-5. |
| [33] | Osuh, M. E., Oke, G. A., Lilford, R. J., Osuh, J. I., Lawal, F. B., Gbadebo, S. O., Harris, B. Oral health in an urban slum, Nigeria: residents’ perceptions, practices and care-seeking experiences. BMC oral health. 2023, 23(1), 657. |
| [34] | Panditi, M., K A., Palle, E., & Kodali, P. B. (2025). Availability and utilisation of oral healthcare services at rural community health centers in South India: a mixed methods study. BMC oral health, 25(1), 977. |
| [35] | Parmar, D., Sailo, J. L., Sakhamuri, S., Dalapati, C., Dutta, S. D., Arya, S., & Dixit, H. (2025). Assessment of Oral Health Disparities and Barriers to Care among Underserved Populations in Urban and Rural Settings. Journal of pharmacy & bioallied sciences, 17(Suppl 1), S445–S447. |
| [36] | Peres, M. A., Macpherson, L. M. D., Weyant, R. J., Daly, B., Venturelli, R., Mathur, M. R., Listl, S., Celeste, R. K., Guarnizo-Herreño, C. C., Kearns, C., Benzian, H., Allison, P., & Watt, R. G. (2019). Oral diseases: a global public health challenge. Lancet (London, England), 394(10194), 249–260. |
| [37] | Samuel, D., Eyenghe, T., & Brown, I. (2025). Socioeconomic Effects on Household Access to Primary Healthcare Facilities in Selected Riverine Communities, Rivers State, Nigeria. International Journal of Social Science and Human Research, 4(5) 967-979. |
| [38] | Sharmin, F., Matsuyama, Y., Kino, S., Kiuchi, S., Kondo, K., & Aida, J. (2025). Gender differences in roles of health behavior between marital status and oral health. Geriatrics & gerontology international, 25(10), 1397–1403. |
| [39] | Shomuyiwa, D. O., & Bridge, G. (2023). Oral health of adolescents in West Africa: prioritizing its social determinants. Global health research and policy, 8(1), 28. |
| [40] | Shrestha, A., Bhagat, T., Agrawal, S. K., Gautam, U., & Joshi, N. P. (2025). Practice of self-medication to manage oral health issues in a community setting in Nepal. BMC oral health, 25(1), 32. |
| [41] | Stephen, O. O., Kelvin, O. O., Udogadi, N. S. (2022). Oral health knowledge, attitude, practices, and utilisation of dental services amongst automobile technicians in Benin City. Biomedical Journal of Scientific & Technical Research. 2022, 44(3), 35524-35530. |
| [42] | Wali, E., Phil-Eze, P. O., Wizor, C. H., Abdullahi, M., Afolabi, O. O., Eze, I. C., & Bosco-Abiahu, L. C. (2021). Flood vulnerability assessment on selected communities in local Government Area of Rivers State, Nigeria, using remote sensing and GIS techniques. J. Geogr. Environ. Earth Sci. Int, 25, 46-57. |
| [43] | Wang, L., Gao, H., Chen, J., Shi, Y., Ma, D., Fan, J., & Xia, X. (2025). Knowledge, attitude, and practice towards oral health in parents and teachers of kindergarten students: a cross-sectional survey. BMJ open, 15(6), e089404. |
| [44] | Wert, M. (2020). Remembering Restoration Losers: Oguri Tadamasa, Ii Naosuke, and Tokugawa Supporters. BRILL. |
| [45] | World Health Organisation (WHO). (2022). Global oral health status report: Towards universal health coverage for oral health by 2030. Geneva: WHO. |
| [46] | Yadav, P., Arya, A., & Yadav, P. (2022). Prevalence of tobacco use and awareness about its ill-effects amongst adult rural population of district Rewari. International Journal of Community. Medicine. Public Health, 11(9), 4190. |
APA Style
Ndudim, O. M., Atuzie, Q. D., Ogba, A. A., Emordi, N. A., Wegbom, A. I. (2026). Assessment of Knowledge, Attitudes and Utilisation of Professional Dental Care Services Among Rural Residents of Ikwerre Local Government Area, Rivers State, Nigeria. American Journal of Health Research, 14(2), 65-76. https://doi.org/10.11648/j.ajhr.20261402.11
ACS Style
Ndudim, O. M.; Atuzie, Q. D.; Ogba, A. A.; Emordi, N. A.; Wegbom, A. I. Assessment of Knowledge, Attitudes and Utilisation of Professional Dental Care Services Among Rural Residents of Ikwerre Local Government Area, Rivers State, Nigeria. Am. J. Health Res. 2026, 14(2), 65-76. doi: 10.11648/j.ajhr.20261402.11
AMA Style
Ndudim OM, Atuzie QD, Ogba AA, Emordi NA, Wegbom AI. Assessment of Knowledge, Attitudes and Utilisation of Professional Dental Care Services Among Rural Residents of Ikwerre Local Government Area, Rivers State, Nigeria. Am J Health Res. 2026;14(2):65-76. doi: 10.11648/j.ajhr.20261402.11
@article{10.11648/j.ajhr.20261402.11,
author = {Oluchi Mildred Ndudim and Queen Desmond Atuzie and Amaka Azubuike Ogba and Nnenna Ali Emordi and Anthony Ike Wegbom},
title = {Assessment of Knowledge, Attitudes and Utilisation of Professional Dental Care Services Among Rural Residents of Ikwerre Local Government Area, Rivers State, Nigeria},
journal = {American Journal of Health Research},
volume = {14},
number = {2},
pages = {65-76},
doi = {10.11648/j.ajhr.20261402.11},
url = {https://doi.org/10.11648/j.ajhr.20261402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20261402.11},
abstract = {Oral health is an essential component of overall health and quality of life; however, utilisation of professional dental care services remains low in many rural communities in Nigeria. Knowledge and attitudes toward dental care are key determinants of service utilisation, particularly in underserved populations. This study assessed the knowledge, attitudes, and utilisation of professional dental care services among rural residents of Ikwerre Local Government Area, Rivers State, Nigeria. Method: A community-based cross-sectional study was conducted among 300 rural residents selected using multistage sampling. Data were collected using a structured interviewer-administered questionnaire. Descriptive statistics were used to summarize respondents’ knowledge, attitudes, and utilisation of dental care services, while Chi-square tests were used to examine associations between socio-demographic characteristics and knowledge and attitudes. Statistical significance was set at p < 0.05. Result: Most respondents demonstrated good knowledge of oral/dental health (84.3%). Despite this, attitudes toward dental care utilisation were largely negative, with 63.7% of respondents exhibiting unfavourable attitudes. Utilisation of professional dental care services was generally low and largely symptom-driven. Sex and monthly income were significantly associated with knowledge of oral/dental health (p < 0.05). Attitude toward dental care utilisation was significantly associated with level of education, occupation, and monthly income (p < 0.001), while age, marital status, and sex showed no significant association. Conclusion: Although knowledge of oral health was relatively high among rural residents of Ikwerre Local Government Area, negative attitudes toward dental care and low utilisation of professional services persist. Socioeconomic factors play a significant role in shaping attitudes and knowledge, underscoring the need for targeted oral health education, attitude-focused interventions, and improved accessibility and affordability of dental services in rural communities.},
year = {2026}
}
TY - JOUR T1 - Assessment of Knowledge, Attitudes and Utilisation of Professional Dental Care Services Among Rural Residents of Ikwerre Local Government Area, Rivers State, Nigeria AU - Oluchi Mildred Ndudim AU - Queen Desmond Atuzie AU - Amaka Azubuike Ogba AU - Nnenna Ali Emordi AU - Anthony Ike Wegbom Y1 - 2026/03/04 PY - 2026 N1 - https://doi.org/10.11648/j.ajhr.20261402.11 DO - 10.11648/j.ajhr.20261402.11 T2 - American Journal of Health Research JF - American Journal of Health Research JO - American Journal of Health Research SP - 65 EP - 76 PB - Science Publishing Group SN - 2330-8796 UR - https://doi.org/10.11648/j.ajhr.20261402.11 AB - Oral health is an essential component of overall health and quality of life; however, utilisation of professional dental care services remains low in many rural communities in Nigeria. Knowledge and attitudes toward dental care are key determinants of service utilisation, particularly in underserved populations. This study assessed the knowledge, attitudes, and utilisation of professional dental care services among rural residents of Ikwerre Local Government Area, Rivers State, Nigeria. Method: A community-based cross-sectional study was conducted among 300 rural residents selected using multistage sampling. Data were collected using a structured interviewer-administered questionnaire. Descriptive statistics were used to summarize respondents’ knowledge, attitudes, and utilisation of dental care services, while Chi-square tests were used to examine associations between socio-demographic characteristics and knowledge and attitudes. Statistical significance was set at p < 0.05. Result: Most respondents demonstrated good knowledge of oral/dental health (84.3%). Despite this, attitudes toward dental care utilisation were largely negative, with 63.7% of respondents exhibiting unfavourable attitudes. Utilisation of professional dental care services was generally low and largely symptom-driven. Sex and monthly income were significantly associated with knowledge of oral/dental health (p < 0.05). Attitude toward dental care utilisation was significantly associated with level of education, occupation, and monthly income (p < 0.001), while age, marital status, and sex showed no significant association. Conclusion: Although knowledge of oral health was relatively high among rural residents of Ikwerre Local Government Area, negative attitudes toward dental care and low utilisation of professional services persist. Socioeconomic factors play a significant role in shaping attitudes and knowledge, underscoring the need for targeted oral health education, attitude-focused interventions, and improved accessibility and affordability of dental services in rural communities. VL - 14 IS - 2 ER -
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Information