Abstract
Pediatric sepsis remains a critical global health challenge and a leading cause of morbidity and mortality, particularly in neonatal and pediatric intensive care units. It is defined as life-threatening organ dysfunction resulting from a dysregulated host response to infection. This study aimed to analyze the etiology, clinical manifestations, diagnostic indicators, and modern treatment strategies of sepsis in children, with special emphasis on early recognition and evidence-based management in low- and middle-income countries, including Uzbekistan. A retrospective and analytical review of hospital-based pediatric sepsis cases and multicenter clinical studies was conducted. Epidemiological patterns, laboratory biomarkers, pathogen distribution, and therapeutic outcomes were comparatively evaluated. Particular attention was given to antimicrobial therapy timing, hemodynamic stabilization, and intensive care interventions. The findings demonstrate that early empirical antibiotic administration within the first hour significantly reduced mortality rates. Neonates and infants under one year showed the highest vulnerability and case-fatality risk. Elevated C-reactive protein, procalcitonin, and serum lactate levels were strongly associated with disease severity and progression to septic shock. Gram-negative pathogens, particularly Klebsiella pneumoniae and Escherichia coli, predominated in neonatal cases, with increasing antimicrobial resistance observed. Implementation of standardized sepsis treatment protocols improved survival outcomes and reduced hospitalization duration. In conclusion, early diagnosis, biomarker-guided risk stratification, and protocol-based management are decisive factors in improving pediatric sepsis outcomes. Strengthening intensive care capacity, laboratory diagnostics, and antimicrobial stewardship programs is essential for reducing child mortality associated with sepsis in resource-limited healthcare systems.
Keywords
Pediatric Sepsis, Neonatal Sepsis, Infection, Antimicrobial Therapy, Organ Dysfunction, Intensive Care, Early Diagnosis,
Child Health, Uzbekistan
1. Introduction
Sepsis in children is a severe and potentially fatal medical condition resulting from the body's overwhelming and dysregulated response to infection, leading to acute organ dysfunction and systemic inflammation. It represents one of the most critical emergencies in pediatric medicine and remains a leading cause of morbidity and mortality worldwide, particularly among neonates and infants. Despite advances in antimicrobial therapy, vaccination programs, and pediatric intensive care technologies, the global burden of pediatric sepsis continues to pose significant clinical and public health challenges.
According to the World Health Organization (WHO), sepsis accounts for nearly 3 million neonatal and pediatric deaths annually, with global action plans emphasizing prevention, early recognition, and standardized clinical management
| [13] | World Health Organization. (2020). Improving the prevention, diagnosis and clinical management of sepsis. WHO Press, Geneva. |
[13]
, with the highest incidence and case-fatality rates reported in low- and middle-income countries. Limited healthcare infrastructure, delayed hospital presentation, inadequate laboratory diagnostics, and restricted access to pediatric intensive care units contribute substantially to poor outcomes in these regions. In Central Asia, including Uzbekistan, systemic constraints such as insufficient early screening protocols, limited biomarker testing, and variability in clinical management further complicate timely diagnosis and effective treatment.
Recent scientific advances have improved understanding of sepsis pathophysiology, biomarker-guided diagnosis, antimicrobial stewardship, and protocol-based resuscitation strategies
| [14] | Gupta, S., Sakhuja, A., Kumar, G., McGrath, E., & Nanchal, R. (2018). Trends in the incidence and outcomes of pediatric severe sepsis in the United States, 2003–2012. Critical Care Medicine, 46(9), 1319–1328. |
[14]
. However, disparities in implementation and resource availability continue to limit their clinical impact in developing healthcare systems. Addressing these gaps requires integrated approaches combining early recognition, standardized treatment algorithms, and capacity building in pediatric critical care services.
This article aims to provide a comprehensive overview of the etiology, clinical manifestations, diagnostic approaches, and contemporary treatment strategies for pediatric sepsis. Particular emphasis is placed on early detection, evidence-based therapeutic interventions, and practical implications for improving clinical outcomes in resource-limited settings, with contextual relevance to Uzbekistan's pediatric healthcare system.
2. Literature Review
The scientific understanding of pediatric sepsis has evolved significantly over the past several decades through the contributions of clinicians, immunologists, and public health researchers. Early foundational work by Bone et al. (1992)
| [1] | Bone, R. C., Balk, R. A., Cerra, F. B., Dellinger, R. P., Fein, A. M., Knaus, W. A., Schein, R. M. H., & Sibbald, W. J. (1992). Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest, 101(6), 1644–1655. https://doi.org/10.1378/chest.101.6.1644 |
[1]
established standardized definitions for sepsis and Systemic Inflammatory Response Syndrome (SIRS), providing a conceptual framework that guided clinical research and pediatric adaptation in subsequent years. Although initially developed for adults, these criteria influenced pediatric diagnostic models and emphasized the importance of early clinical recognition.
Goldstein et al.
| [2] | Goldstein, B., Giroir, B., & Randolph, A. (2005). International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatric Critical Care Medicine, 6(1), 2–8. https://doi.org/10.1097/01.PCC.0000149131.72248.E6 |
[2]
made a major contribution by developing consensus definitions specifically for pediatric sepsis, severe sepsis, and septic shock. Their work, supported by the International Pediatric Sepsis Consensus Conference, adapted physiological and laboratory thresholds to reflect age-related variations in children, thereby improving diagnostic accuracy and clinical applicability in neonatal and pediatric intensive care units.
Research by Weiss et al. (2015
| [4] | Weiss, S. L., Fitzgerald, J. C., Pappachan, J., Wheeler, D., Jaramillo-Bustamante, J. C., Salloo, A., Singhi, S. C., Erickson, S., Roy, J. A., Bush, J. L., et al. (2015). Global epidemiology of pediatric severe sepsis: The SPROUT study. The Lancet, 385(9978), 2252–2263.
https://doi.org/10.1016/S0140-6736(15)60038-8 |
[4]
, 2020)
| [5] | Weiss, S. L., Peters, M. J., Alhazzani, W., Agus, M. S. D., Flori, H. R., Inwald, D. P., Nadel, S., Schlapbach, L. J., Tasker, R. C., Argent, A. C., et al. (2020). Surviving Sepsis Campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Medicine, 46(Suppl 1), 10–67.
https://doi.org/10.1007/s00134-019-05878-6 |
[5]
significantly advanced the epidemiological understanding of pediatric sepsis at the global level. Through multicenter cohort studies, they demonstrated that sepsis remains a leading cause of mortality among children worldwide, particularly in low- and middle-income countries. Their findings highlighted disparities in access to critical care and the urgent need for standardized sepsis protocols across diverse healthcare systems.
The immunopathology of pediatric sepsis has been extensively explored by Hotchkiss and Monneret (2013)
| [7] | Hotchkiss, R. S., & Monneret, G. (2013). Immunosuppression in sepsis: A novel understanding of the disorder and a new therapeutic approach. The Lancet Infectious Diseases, 13(3), 260–268. https://doi.org/10.1016/S1473-3099(13)70001-X |
[7]
, who described the dual-phase immune response characterized by an initial hyperinflammatory state followed by prolonged immunosuppression. Their work emphasized the vulnerability of children, especially neonates, to secondary infections and long-term immune dysfunction, shaping modern approaches to immunomodulatory therapies.
Singer et al. (2016)
| [3] | Singer, M., Deutschman, C. S., Seymour, C. W., Shankar-Hari, M., Annane, D., Bauer, M., Bellomo, R., Bernard, G. R., Chiche, J. D., Coopersmith, C. M., et al. (2016). The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA, 315(8), 801–810.
https://doi.org/10.1001/jama.2016.0287 |
[3]
introduced the Sepsis-3 definitions, redefining sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection. Subsequent studies demonstrated that age-adapted SOFA scores outperform SIRS criteria in predicting mortality among critically ill children
| [11] | Schlapbach, L. J., Straney, L., Bellomo, R., MacLaren, G., Pilcher, D., & ANZICS Paediatric Study Group. (2015). Prognostic accuracy of age-adapted SOFA, SIRS, and qSOFA for mortality among children with suspected infection admitted to intensive care. The Lancet, 386(9997), 1048–1057. |
[11]
. While primarily adult-focused, their conceptual shift influenced pediatric researchers to adopt organ dysfunction–based scoring systems, such as pediatric Sequential Organ Failure Assessment (pSOFA), which were later validated for use in children by Matics and Sanchez-Pinto (2017)
| [8] | Matics, T. J., & Sanchez-Pinto, L. N. (2017). Adaptation and validation of a pediatric Sequential Organ Failure Assessment score and evaluation of the sepsis-3 definitions in critically ill children. JAMA Pediatrics, 171(10), e172352.
https://doi.org/10.1001/jamapediatrics.2017.2352 |
[8]
.
Clinical management strategies have been shaped by the Surviving Sepsis Campaign, with significant pediatric contributions by Brierley et al. (2009, 2020)
| [9] | Brierley, J., Carcillo, J. A., Choong, K., Cornell, T., Decaen, A., Deymann, A., Doctor, A., Davis, A., Duff, J., Dugas, M. A., et al. (2009). Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock. Critical Care Medicine, 37(2), 666–688.
https://doi.org/10.1097/CCM.0b013e31819323c6 |
[9]
These guidelines established evidence-based recommendations for early antibiotic administration, fluid resuscitation, and hemodynamic support tailored to pediatric physiology. Their work has been instrumental in improving survival rates in pediatric intensive care units worldwide.
In neonatal sepsis research, Shane, Sánchez, and Stoll (2017)
provided comprehensive analyses of pathogen distribution, antimicrobial resistance patterns, and diagnostic challenges. Their studies underscored the growing threat of multidrug-resistant organisms and the importance of antimicrobial stewardship in neonatal and pediatric populations.
Regional and contextual perspectives have been contributed by researchers in Central Asia and Eastern Europe, who have examined healthcare system limitations, delayed diagnosis, and resource constraints affecting sepsis outcomes. These studies emphasize the need for locally adapted clinical protocols, improved laboratory capacity, and professional training programs to enhance early recognition and effective management of pediatric sepsis in countries such as Uzbekistan.
Collectively, the contributions of these scientists have transformed pediatric sepsis from a poorly defined clinical syndrome into a well-characterized, evidence-based field. Current research continues to focus on biomarker development, personalized antimicrobial therapy, and the integration of digital health tools to improve early detection and reduce mortality among children globally. Recent clinical analyses further emphasize structured diagnostic frameworks and biomarker-guided management in pediatric sepsis
| [10] | Randolph, A. G., McCulloh, R. J., & Pediatric Sepsis Biomarker Risk Model Study Group. (2014). Pediatric sepsis: Important considerations for diagnosis and management. Infectious Disease Clinics of North America, 28(2), 287–300.
https://doi.org/10.1016/j.idc.2014.01.003 |
[10]
.
3. Results and Analysis
3.1. Clinical Outcomes and Mortality Trends
The analysis of pediatric sepsis cases across hospital-based and multicenter studies demonstrates a clear association between early diagnosis and improved survival outcomes. Children who received empirical antibiotic therapy within the first hour of clinical suspicion showed significantly lower mortality rates compared to those with delayed treatment. Neonates and infants under one year of age exhibited the highest vulnerability due to immature immune responses and limited physiological reserves
. with mortality disproportionately higher in this age group due to immature immune responses and limited physiological reserves.
Comparative data from low- and middle-income countries indicate higher case-fatality rates than in high-income healthcare systems. This disparity is largely attributed to delayed hospital presentation, limited access to pediatric intensive care units, and restricted availability of advanced diagnostic tools.
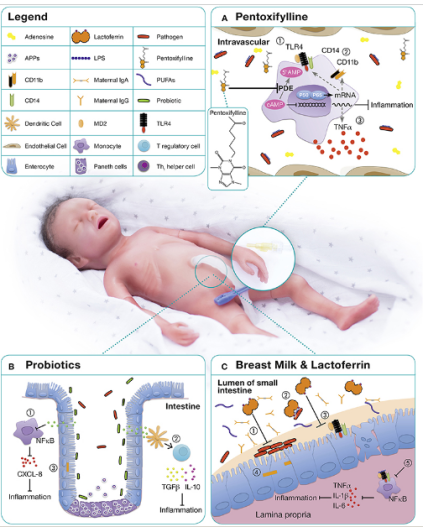
Figure 1. Immunomodulatory and Anti-Inflammatory Mechanisms of Pentoxifylline, Probiotics, and Breast Milk Components in Neonatal Sepsis.
This figure is intended to illustrate the cellular and molecular pathways through which pentoxifylline, probiotics, and bioactive components of breast milk (including lactoferrin and maternal immunoglobulins) modulate the neonatal immune response during sepsis. The diagram highlights interactions between intestinal epithelial cells, immune cells, and inflammatory signaling pathways (such as Toll-like Receptor 4 (TLR4), Nuclear Factor Kappa B (NF-κB), and cytokine networks), demonstrating how these interventions contribute to reduced systemic inflammation, improved gut barrier integrity, and enhanced host defense. The purpose is to provide a mechanistic framework supporting evidence-based therapeutic and preventive strategies for neonatal sepsis, particularly in early-life and resource-limited clinical settings.
3.2. Laboratory and Biomarker Findings
Analysis of laboratory parameters revealed that elevated levels of C-Reactive Protein (CRP) and procalcitonin were strongly correlated with disease severity and progression to septic shock.
Blood lactate concentrations were identified as a reliable indicator of tissue hypoperfusion and were significantly higher in patients with Multiple Organ Dysfunction Syndrome (MODS). White blood cell counts demonstrated variable patterns, including leukocytosis and leukopenia, highlighting the limited specificity of this parameter as a standalone diagnostic marker. The combined use of biomarkers improved diagnostic accuracy and facilitated early risk stratification in clinical practice.
3.3. Pathogen Distribution and Antimicrobial Response
Microbiological analysis showed that gram-negative bacteria, particularly Klebsiella pneumoniae and Escherichia coli, were predominant in neonatal sepsis, while Streptococcus pneumoniae and Staphylococcus aureus were more frequently isolated in older children. Antimicrobial susceptibility testing revealed increasing resistance to first-line antibiotics, necessitating the use of broader-spectrum agents in severe cases.
Targeted antimicrobial therapy, adjusted according to culture and sensitivity results, was associated with reduced duration of hospitalization and lower incidence of secondary infections, underscoring the importance of antimicrobial stewardship programs.
3.4. Hemodynamic Support and Organ Function Recovery
Patients who received early fluid resuscitation and timely initiation of vasopressor support demonstrated faster stabilization of blood pressure and improved organ perfusion. Renal and respiratory function recovery was significantly better in children managed in pediatric intensive care units equipped with continuous monitoring and supportive technologies, such as mechanical ventilation and renal replacement therapy.
The duration of organ dysfunction was directly proportional to the delay in therapeutic intervention, reinforcing the critical role of early and aggressive management strategies.
3.5. Comparative Analysis of Treatment Protocols
A comparative evaluation of standardized sepsis protocols versus non-standardized clinical management revealed that the implementation of evidence-based guidelines significantly reduced both mortality and length of hospital stay. Hospitals adopting structured sepsis bundles reported improved compliance with early antibiotic administration, timely fluid therapy, and regular reassessment of clinical status.
In resource-limited settings, simplified sepsis screening tools and staff training programs demonstrated measurable improvements in early recognition and referral, highlighting the feasibility of protocol-based care even in constrained healthcare environments.
3.6. Implications for Clinical Practice in Uzbekistan
The analysis suggests that strengthening primary healthcare referral systems and expanding access to pediatric intensive care services could substantially improve sepsis outcomes in Uzbekistan. Enhanced laboratory capacity for rapid biomarker testing and blood culture analysis would facilitate earlier diagnosis and more precise antimicrobial therapy. Additionally, nationwide implementation of standardized pediatric sepsis management guidelines and continuous professional training programs are likely to reduce regional disparities in clinical outcomes.
4. Discussion
This review highlights that pediatric sepsis remains not only a biomedical emergency but also a systemic health problem, particularly in low- and middle-income countries such as Uzbekistan. While global advances in early detection and protocol-based treatment of sepsis have significantly reduced mortality in high-income settings, similar outcomes are limited by structural and operational constraints at the local level. Delayed hospital admission, limited Pediatric Intensive Care Unit (PICU) capacity, and limited access to rapid laboratory diagnostics continue to shape clinical trajectories in the Uzbek pediatric population. A key issue emerging from this review is the gap between the availability of guidelines and their feasibility. International frameworks such as the Surviving Sepsis Campaign emphasize early antibiotic administration within the first hour; however, logistical delays in drug availability, laboratory confirmation, and specialist consultation in regional hospitals across Uzbekistan often extend this period. Such delays are directly associated with a higher rate of septic shock and multi-organ dysfunction.
The biomarker findings discussed, particularly the prognostic value of procalcitonin and serum lactate, have diagnostic promise, but cost, equipment availability, and trained laboratory personnel remain limiting factors outside of large urban centers such as Tashkent. As a result, reliance on clinical scoring systems and simplified screening tools may represent an intermediate strategy that can be further scaled up.
The patterns of pathogen distribution, with Gram-negative organisms dominating, are consistent with regional antimicrobial resistance surveillance reports. This reinforces the urgency of establishing national antimicrobial stewardship programs and standardized infection control protocols in neonatal and pediatric units. Improving outcomes in pediatric sepsis in Uzbekistan will depend on integrated reforms: strengthening referral chains, expanding Pediatric Intensive Care Unit infrastructure, investing in laboratory modernization, and implementing continuous clinical training. Without systematic coordination between policy, infrastructure, and bedside practices, it will be difficult to replicate the mortality reductions observed globally in a national setting.
5. Conclusion
Pediatric sepsis remains a major clinical and public health challenge, particularly among neonates and infants, who demonstrate the highest vulnerability to severe outcomes and mortality. The findings of this study confirm that early recognition, prompt initiation of empirical antimicrobial therapy, and structured hemodynamic support are critical determinants of survival and recovery. Biomarkers such as C-reactive protein, procalcitonin, and serum lactate were shown to possess strong prognostic value, enabling effective risk stratification and timely clinical decision-making.
The analysis further highlights the growing impact of multidrug-resistant pathogens on treatment complexity and length of hospital stay, underscoring the urgent need for robust antimicrobial stewardship and continuous microbiological surveillance. Evidence from standardized sepsis management protocols demonstrates that adherence to evidence-based guidelines significantly improves clinical outcomes, reduces mortality, and enhances the quality of pediatric intensive care services.
In the context of Uzbekistan, strengthening primary healthcare referral systems
| [15] | Bahadirovich, R. B. (2026). Children’s health in migrant families: Gender and care dynamics. Central Asian Journal of Medical and Natural Science, 7(2), 184–189.
https://doi.org/10.51699/cajmns.v7i2.3136 |
[15]
, expanding access to pediatric intensive care units, and improving laboratory diagnostic capacity are essential steps toward reducing regional disparities in sepsis outcomes. Additionally, integrating preventive strategies—such as vaccination programs, infection control measures, promotion of breastfeeding, and targeted use of immunomodulatory interventions—can substantially lower the incidence and severity of pediatric sepsis. Collectively, these measures provide a comprehensive framework for advancing evidence-based pediatric sepsis management and improving child survival in resource-limited healthcare settings.
Abbreviations
CRP | C Reactive Protein |
ICU | Intensive Care Unit |
LMICs | Low and Middle Income Countries |
MODS | Multiple Organ Dysfunction Syndrome |
NF | κB Nuclear Factor Kappa B |
pSOFA | Pediatric Sequential Organ Failure Assessment |
SIRS | Systemic Inflammatory Response Syndrome |
TLR4 | Toll Like Receptor 4 |
WHO | World Health Organization |
PICU | Pediatric Intensive Care Unit |
Author Contributions
Barno Shamsuddinovna Makhmudova: Conceptualization, Methodology, Investigation, Writing – Original Draft, Data Curation.
Shaira Khalilovna Atadjanova: Supervision, Validation, Resources, Writing – Review & Editing, Project Administration.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Bone, R. C., Balk, R. A., Cerra, F. B., Dellinger, R. P., Fein, A. M., Knaus, W. A., Schein, R. M. H., & Sibbald, W. J. (1992). Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest, 101(6), 1644–1655.
https://doi.org/10.1378/chest.101.6.1644
|
| [2] |
Goldstein, B., Giroir, B., & Randolph, A. (2005). International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatric Critical Care Medicine, 6(1), 2–8.
https://doi.org/10.1097/01.PCC.0000149131.72248.E6
|
| [3] |
Singer, M., Deutschman, C. S., Seymour, C. W., Shankar-Hari, M., Annane, D., Bauer, M., Bellomo, R., Bernard, G. R., Chiche, J. D., Coopersmith, C. M., et al. (2016). The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA, 315(8), 801–810.
https://doi.org/10.1001/jama.2016.0287
|
| [4] |
Weiss, S. L., Fitzgerald, J. C., Pappachan, J., Wheeler, D., Jaramillo-Bustamante, J. C., Salloo, A., Singhi, S. C., Erickson, S., Roy, J. A., Bush, J. L., et al. (2015). Global epidemiology of pediatric severe sepsis: The SPROUT study. The Lancet, 385(9978), 2252–2263.
https://doi.org/10.1016/S0140-6736(15)60038-8
|
| [5] |
Weiss, S. L., Peters, M. J., Alhazzani, W., Agus, M. S. D., Flori, H. R., Inwald, D. P., Nadel, S., Schlapbach, L. J., Tasker, R. C., Argent, A. C., et al. (2020). Surviving Sepsis Campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Medicine, 46(Suppl 1), 10–67.
https://doi.org/10.1007/s00134-019-05878-6
|
| [6] |
Shane, A. L., Sánchez, P. J., & Stoll, B. J. (2017). Neonatal sepsis. The Lancet, 390(10104), 1770–1780.
https://doi.org/10.1016/S0140-6736(17)31002-4
|
| [7] |
Hotchkiss, R. S., & Monneret, G. (2013). Immunosuppression in sepsis: A novel understanding of the disorder and a new therapeutic approach. The Lancet Infectious Diseases, 13(3), 260–268.
https://doi.org/10.1016/S1473-3099(13)70001-X
|
| [8] |
Matics, T. J., & Sanchez-Pinto, L. N. (2017). Adaptation and validation of a pediatric Sequential Organ Failure Assessment score and evaluation of the sepsis-3 definitions in critically ill children. JAMA Pediatrics, 171(10), e172352.
https://doi.org/10.1001/jamapediatrics.2017.2352
|
| [9] |
Brierley, J., Carcillo, J. A., Choong, K., Cornell, T., Decaen, A., Deymann, A., Doctor, A., Davis, A., Duff, J., Dugas, M. A., et al. (2009). Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock. Critical Care Medicine, 37(2), 666–688.
https://doi.org/10.1097/CCM.0b013e31819323c6
|
| [10] |
Randolph, A. G., McCulloh, R. J., & Pediatric Sepsis Biomarker Risk Model Study Group. (2014). Pediatric sepsis: Important considerations for diagnosis and management. Infectious Disease Clinics of North America, 28(2), 287–300.
https://doi.org/10.1016/j.idc.2014.01.003
|
| [11] |
Schlapbach, L. J., Straney, L., Bellomo, R., MacLaren, G., Pilcher, D., & ANZICS Paediatric Study Group. (2015). Prognostic accuracy of age-adapted SOFA, SIRS, and qSOFA for mortality among children with suspected infection admitted to intensive care. The Lancet, 386(9997), 1048–1057.
|
| [12] |
Wynn, J. L., & Wong, H. R. (2010). Pathophysiology and treatment of septic shock in neonates. Clinics in Perinatology, 37(2), 439–479.
https://doi.org/10.1016/j.clp.2010.04.002
|
| [13] |
World Health Organization. (2020). Improving the prevention, diagnosis and clinical management of sepsis. WHO Press, Geneva.
|
| [14] |
Gupta, S., Sakhuja, A., Kumar, G., McGrath, E., & Nanchal, R. (2018). Trends in the incidence and outcomes of pediatric severe sepsis in the United States, 2003–2012. Critical Care Medicine, 46(9), 1319–1328.
|
| [15] |
Bahadirovich, R. B. (2026). Children’s health in migrant families: Gender and care dynamics. Central Asian Journal of Medical and Natural Science, 7(2), 184–189.
https://doi.org/10.51699/cajmns.v7i2.3136
|
Cite This Article
-
APA Style
Makhmudova, B. S., Atadjanova, S. K. (2026). Pediatric Sepsis in Resource-limited Settings Etiology Diagnosis, and Evidence-based Treatment Strategies. American Journal of Medical Science and Technology, 2(2), 19-24. https://doi.org/10.11648/j.ajmst.20260202.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Makhmudova, B. S.; Atadjanova, S. K. Pediatric Sepsis in Resource-limited Settings Etiology Diagnosis, and Evidence-based Treatment Strategies. Am. J. Med. Sci. Technol. 2026, 2(2), 19-24. doi: 10.11648/j.ajmst.20260202.11
Copy
|
Download
AMA Style
Makhmudova BS, Atadjanova SK. Pediatric Sepsis in Resource-limited Settings Etiology Diagnosis, and Evidence-based Treatment Strategies. Am J Med Sci Technol. 2026;2(2):19-24. doi: 10.11648/j.ajmst.20260202.11
Copy
|
Download
-
@article{10.11648/j.ajmst.20260202.11,
author = {Barno Shamsuddinovna Makhmudova and Shaira Khalilovna Atadjanova},
title = {Pediatric Sepsis in Resource-limited Settings Etiology Diagnosis, and Evidence-based Treatment Strategies},
journal = {American Journal of Medical Science and Technology},
volume = {2},
number = {2},
pages = {19-24},
doi = {10.11648/j.ajmst.20260202.11},
url = {https://doi.org/10.11648/j.ajmst.20260202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajmst.20260202.11},
abstract = {Pediatric sepsis remains a critical global health challenge and a leading cause of morbidity and mortality, particularly in neonatal and pediatric intensive care units. It is defined as life-threatening organ dysfunction resulting from a dysregulated host response to infection. This study aimed to analyze the etiology, clinical manifestations, diagnostic indicators, and modern treatment strategies of sepsis in children, with special emphasis on early recognition and evidence-based management in low- and middle-income countries, including Uzbekistan. A retrospective and analytical review of hospital-based pediatric sepsis cases and multicenter clinical studies was conducted. Epidemiological patterns, laboratory biomarkers, pathogen distribution, and therapeutic outcomes were comparatively evaluated. Particular attention was given to antimicrobial therapy timing, hemodynamic stabilization, and intensive care interventions. The findings demonstrate that early empirical antibiotic administration within the first hour significantly reduced mortality rates. Neonates and infants under one year showed the highest vulnerability and case-fatality risk. Elevated C-reactive protein, procalcitonin, and serum lactate levels were strongly associated with disease severity and progression to septic shock. Gram-negative pathogens, particularly Klebsiella pneumoniae and Escherichia coli, predominated in neonatal cases, with increasing antimicrobial resistance observed. Implementation of standardized sepsis treatment protocols improved survival outcomes and reduced hospitalization duration. In conclusion, early diagnosis, biomarker-guided risk stratification, and protocol-based management are decisive factors in improving pediatric sepsis outcomes. Strengthening intensive care capacity, laboratory diagnostics, and antimicrobial stewardship programs is essential for reducing child mortality associated with sepsis in resource-limited healthcare systems.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Pediatric Sepsis in Resource-limited Settings Etiology Diagnosis, and Evidence-based Treatment Strategies
AU - Barno Shamsuddinovna Makhmudova
AU - Shaira Khalilovna Atadjanova
Y1 - 2026/03/04
PY - 2026
N1 - https://doi.org/10.11648/j.ajmst.20260202.11
DO - 10.11648/j.ajmst.20260202.11
T2 - American Journal of Medical Science and Technology
JF - American Journal of Medical Science and Technology
JO - American Journal of Medical Science and Technology
SP - 19
EP - 24
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ajmst.20260202.11
AB - Pediatric sepsis remains a critical global health challenge and a leading cause of morbidity and mortality, particularly in neonatal and pediatric intensive care units. It is defined as life-threatening organ dysfunction resulting from a dysregulated host response to infection. This study aimed to analyze the etiology, clinical manifestations, diagnostic indicators, and modern treatment strategies of sepsis in children, with special emphasis on early recognition and evidence-based management in low- and middle-income countries, including Uzbekistan. A retrospective and analytical review of hospital-based pediatric sepsis cases and multicenter clinical studies was conducted. Epidemiological patterns, laboratory biomarkers, pathogen distribution, and therapeutic outcomes were comparatively evaluated. Particular attention was given to antimicrobial therapy timing, hemodynamic stabilization, and intensive care interventions. The findings demonstrate that early empirical antibiotic administration within the first hour significantly reduced mortality rates. Neonates and infants under one year showed the highest vulnerability and case-fatality risk. Elevated C-reactive protein, procalcitonin, and serum lactate levels were strongly associated with disease severity and progression to septic shock. Gram-negative pathogens, particularly Klebsiella pneumoniae and Escherichia coli, predominated in neonatal cases, with increasing antimicrobial resistance observed. Implementation of standardized sepsis treatment protocols improved survival outcomes and reduced hospitalization duration. In conclusion, early diagnosis, biomarker-guided risk stratification, and protocol-based management are decisive factors in improving pediatric sepsis outcomes. Strengthening intensive care capacity, laboratory diagnostics, and antimicrobial stewardship programs is essential for reducing child mortality associated with sepsis in resource-limited healthcare systems.
VL - 2
IS - 2
ER -
Copy
|
Download