In the North Batinah Governorate, Sultanate of Oman, a local transmission dengue fever outbreak was examined based on surveillance data from January 1 to December 31, 2023, and containment measures were implemented. This study aimed to determine the sources and factors associated with this outbreak and to recommend countermeasures to prevent future outbreaks. A descriptive analysis was conducted on 194 confirmed cases, followed by an unmatched case-control study involving 194 laboratory-confirmed cases and 194 controls. Data were collected using the standardized dengue fever questionnaire developed by the Oman Ministry of Health, the electronic surveillance system (ALSHIFA+), and phone interviews. Multivariate analysis was performed to examine associations between variables and dengue fever. Among the 194 confirmed cases, males aged 30–59 years (98, 50.5%) were the most affected, with fever (100%), headache (55.2%), and myalgia (49%) being the most common clinical presentations. The case fatality rate was 0.5%. Living in Sohar, particularly in Tareef, Humbar, and Waqaiba, was associated with higher susceptibility to dengue fever (OR = 5.40; 95% CI: 2.17–13.44) due to high vector density, and a history of travel was also identified as a significant risk factor (OR = 3.53; 95% CI: 1.60–7.75). The 2023 dengue fever outbreak was the largest recorded, highlighting the importance of proper removal of breeding sites, community health education, continued implementation of vector control strategies, and maintaining updated vector-borne disease surveillance.
| Published in | American Journal of Medical Science and Technology (Volume 2, Issue 2) |
| DOI | 10.11648/j.ajmst.20260202.14 |
| Page(s) | 57-69 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Dengue Fever Outbreak, Oman, Unmatched Cases Controls Study
Year | No. of cases | Omani | Non- Omani | Travel Associated |
|---|---|---|---|---|
2018 | 2 | 0 | 2 | 2 (100%) |
2019 | 8 | 2 | 6 | 8 (100%) |
2020 | 2 | 2 | 0 | 2 (100%) |
2021 | 6 | 2 | 4 | 4 (66.70%) |
2022 | 29 | 20 | 9 | 12 (41.40%) |
2023 | 194 | 156 | 38 | 28 (14.40%) |
Variable | Cases (n,%) | Controls (n,%) |
|---|---|---|
Gender | ||
Male | 123(63.40%) | 140(72.20%) |
Female | 71(36.60%) | 54(27.80%) |
Age | Age (Median=42 years) (IQR=29 years) | Age (Median=33.5 years) (IQR=21 years) |
1-14 | 8(4.10%) | 11(5.70%) |
15-29 | 38(19.60%) | 61(31.40%) |
30-59 | 98(50.50%) | 87(44.80%) |
>60 years | 50(25.80%) | 35(18.00%) |
Nationality | ||
Omani | 156(80.40%) | 149(76.80%) |
Non Omani | 38(19.60%) | 45(23.20%) |
H/O travel | ||
Yes | 28(14.40%) | 11(5.70%) |
No | 166(85.60%) | 183(94.30%) |
Mean | 44.75 |
Median | 42 |
Standard Deviation | 19.855 |
Minimum | 1 |
Maximum | 91 |
IQR | 29 |
Factor (n 388) | Subgroup | % (n) among cases | % (n) among controls | P-value |
|---|---|---|---|---|
Gender (n 388) | Male | 63.40% (123) | 72.20% (140) | 0.065 |
Female | 36.60% (71) | 27.80% (54) | ||
Age categories (n 388) | 1 - 14 | 4.10% (8) | 5.70% (11) | .028* |
15 - 29 | 19.60% (38) | 31.40% (61) | ||
30 - 59 | 50.50% (98) | 44.80% (87) | ||
≥ 60 | 25.80% (50) | 18.00% (35) | ||
Wilayat (n 385) | Sohar | 76.30% (148) | 52.90% (101) | < 0.001* |
Khaboura | 2.10% (4) | 6.30% (12) | ||
Suwaiq | 6.20% (12) | 11.00% (21) | ||
Liwa | 8.20% (16) | 7.30% (14) | ||
Saham | 3.60% (7) | 10.50% (20) | ||
Shinas | 3.60% (7) | 12.00% (23) | ||
Nationality (n 388) | Omani | 80.40% (156) | 76.80% (149) | 0.386 |
Non-Omani | 19.60% (38) | 23.20% (45) | ||
Travel history (n 388) | Yes | 14.40% (28) | 5.70% (11) | 0.004* |
No | 85.60% (166) | 94.30% (183) |
Factors (n 388) | OR | Lower limit of 95% CI of OR | Upper limit of 95% CI of OR | P value |
|---|---|---|---|---|
Gender (reference group: Male) | 0.053 | |||
Female | 1.568 | .993 | 2.476 | |
Age (reference group: ≤ 14 year | 0.143 | |||
15 - 29 | .953 | .327 | 2.774 | 0.929 |
30 - 59 | 1.552 | .558 | 4.317 | 0.400 |
≥ 60 | 1.904 | .645 | 5.621 | 0.244 |
Wilayat (reference group: Shinas) | < 0.001* | |||
Sohar | 5.400 | 2.169 | 13.444 | 0.000 |
Khaboura | 1.223 | .289 | 5.166 | 0.784 |
Suwaiq | 1.743 | .559 | 5.433 | 0.338 |
Liwa | 4.032 | 1.290 | 12.602 | 0.017 |
Saham | 1.369 | .398 | 4.703 | 0.618 |
Travel history (reference group: No) | 0.002* | |||
Yes | 3.526 | 1.604 | 7.750 | |
MOH | Ministry of Health |
RNA | Ribonucleic Acid |
WHO | World Health Organization |
IgM | Immunoglobulin M |
IgG | Immunoglobulin G |
RT-PCR | Real-time/Reverse transcription Polymerase Chain Reaction |
NS1 | Nonstructural Protein 1 Antigen |
P | Value |
CI | Confidence Interval |
OR | Odd Ratio |
IQR | Interquartile Range |
AOR | Adjusted Odd Ratio |
CFR | Case Fatality Rate |
SPSS | Statistical Package for the Social Science |
AR | Attack Rate |
NBG | North Batinah Governorate |
DF | Dengue Fever |
| [1] | Chan HBY, How CH, Ng CWM. Definitive tests for dengue fever: when and which should I use? Singapore Med J 2017; 58: 632–635. |
| [2] | Mesfin Z, Ali A, Abagero A, et al. Dengue Fever Outbreak Investigation in Werder Town, Dollo Zone, Somali Region, Ethiopia. Infect Drug Resist 2022; 15: 7207–7217. |
| [3] | Wu D, Zhang X, Deng A, et al. Dengue Fever Outbreaks Caused by Varied Serotype Dengue Virus — Guangdong Province, China, 2019. China CDC Wkly 2020; 2: 740–743. |
| [4] | Wiwanitkit V. Unusual mode of transmission of dengue. J Infect Dev Ctries 2009; 4: 51–54. |
| [5] | Al-Tawfiq JA, Memish ZA. Dengue Hemorrhagic Fever Virus in Saudi Arabia: A Review. Vector Borne Zoonotic Dis 2018; 18: 75–81. |
| [6] | Wiemer D, Frickmann H, Krüger A. Dengue fever: Symptoms, epidemiology, entomology, pathogen diagnosis and prevention. Hautarzt 2017; 68: 1011–1020. |
| [7] | Teoid A, Chia PY, Ramireddi GK, et al. Clinical and prognostic relevance of sST2 in adults with dengue-associated cardiac impairment and severe dengue. PLoS Negl Trop Dis 2022; 16: 1–13. |
| [8] | Wilder-Smith A. Dengue vaccine development: status and future. Bundesgesundheitsblatt - Gesundheitsforsch - Gesundheitsschutz 2020; 63: 40–44. |
| [9] | Norshidah H, Vignesh R, Lai NS. Updates on dengue vaccine and antiviral. Molecules 2021; 26: 1–18. |
| [10] | Shim E. Optimal dengue vaccination strategies of seropositive individuals. Math Biosci Eng 2019; 16: 1171–1189. |
| [11] | Raza FA, Rehman SU, Khalid R, et al. Demographic and clinico-epidemiological features of dengue fever in Faisalabad, Pakistan. PLoS One 2014; 9: 5–11. |
| [12] | Sridhar S, Luedtke A, Langevin E, et al. Effect of Dengue Serostatus on Dengue Vaccine Safety and Efficacy. N Engl J Med 2018; 379: 327–340. |
| [13] | Melebari S, Bakri R, Hafiz A, et al. The epidemiology and incidence of dengue in Makkah, Saudi Arabia, during 2017-2019. Saudi Med J 2021; 42: 1173–1179. |
| [14] | Mehmood A, Khalid Khan F, Chaudhry A, et al. Risk Factors Associated with a Dengue Fever Outbreak in Islamabad, Pakistan: Case-Control Study. JMIR public Heal Surveill 2021; 7: e27266. |
| [15] |
National Center for Statistics and Information (NCSI) O. National Center for Statistics and Information,
https://www.ncsi.gov.om/Pages/NCSI.aspx (accessed 24 February 2026). |
| [16] | Al Balushi L, Al Kalbani M, Al Manji A, et al. A second local dengue fever outbreak: A field experience from Muscat Governorate in Oman, 2022. IJID Reg 2023; 7: 237–241. |
| [17] | Al-Abri SS, Kurup PJ, Al Manji A, et al. Control of the 2018–2019 dengue fever outbreak in Oman: A country previously without local transmission. Int J Infect Dis 2020; 90: 97–103. |
| [18] | de Almeida PS, Carneiro JPM, Lima-Camara TN, et al. Aedes Aegypti AND Aedes Albopictus (DIPTERA: CULICIDAE) IN ARTIFICIAL BREEDING SITES IN RURAL SETTLEMENTS AND INDIGENOUS VILLAGES. J Trop Pathol 2024; 53: 333–343. |
| [19] |
(NCSI), National Centre for Statistics & Information O. Population of Al Batinah North Governorate, Oman – 2022,
https://data.gov.om/OMPOP2016/population?lang=ar&tsId=1061400 (2023, accessed 24 February 2026). |
| [20] | Manna S, Satapathy P, Bora I, et al. Dengue outbreaks in South Asia amid Covid-19: Epidemiology, transmission, and mitigation strategies. Front Public Heal; 10. Epub ahead of print 2022. |
| [21] |
Oman G of. Al-Shifa Central Initiative,
https://apps.oman.om/en/home-top-level/whole-of-government/central-initiative/al-shifa%0A (2026, accessed 24 February 2026). |
| [22] |
Report of Infectious Diseases – Tarassud System. Gov.om – Sultanate of Oman,
https://gov.om/en/w/report-of-infectious-diseases (accessed 24 February 2026). |
| [23] | Singh N, Singh AK, Kumar A. Dengue outbreak update in India: 2022. Indian J Public Health 2023; 67: 181–183. |
| [24] | Liu W, Hu W, Dong Z, et al. Travel-related infection in Guangzhou, China, 2009-2019. Travel Med Infect Dis 2021; 43: 102106. |
| [25] | Islam MA, Hasan MN, Tiwari A, et al. Correlation of Dengue and Meteorological Factors in Bangladesh: A Public Health Concern. Int J Environ Res Public Health; 20. Epub ahead of print 2023. |
APA Style
Aljabri, M., Abd-Ellatif, E. E., Hashmi, F. A., Saadi, K. A., Moqbali, A. A. (2026). Dengue Fever Outbreak in North AL Batinah Governorate (Oman), January 2023 –December 2023. American Journal of Medical Science and Technology, 2(2), 57-69. https://doi.org/10.11648/j.ajmst.20260202.14
ACS Style
Aljabri, M.; Abd-Ellatif, E. E.; Hashmi, F. A.; Saadi, K. A.; Moqbali, A. A. Dengue Fever Outbreak in North AL Batinah Governorate (Oman), January 2023 –December 2023. Am. J. Med. Sci. Technol. 2026, 2(2), 57-69. doi: 10.11648/j.ajmst.20260202.14
@article{10.11648/j.ajmst.20260202.14,
author = {Malik Aljabri and Eman Elsayed Abd-Ellatif and Fatma Al Hashmi and Khalid Al Saadi and Abir Al Moqbali},
title = {Dengue Fever Outbreak in North AL Batinah Governorate (Oman), January 2023 –December 2023},
journal = {American Journal of Medical Science and Technology},
volume = {2},
number = {2},
pages = {57-69},
doi = {10.11648/j.ajmst.20260202.14},
url = {https://doi.org/10.11648/j.ajmst.20260202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajmst.20260202.14},
abstract = {In the North Batinah Governorate, Sultanate of Oman, a local transmission dengue fever outbreak was examined based on surveillance data from January 1 to December 31, 2023, and containment measures were implemented. This study aimed to determine the sources and factors associated with this outbreak and to recommend countermeasures to prevent future outbreaks. A descriptive analysis was conducted on 194 confirmed cases, followed by an unmatched case-control study involving 194 laboratory-confirmed cases and 194 controls. Data were collected using the standardized dengue fever questionnaire developed by the Oman Ministry of Health, the electronic surveillance system (ALSHIFA+), and phone interviews. Multivariate analysis was performed to examine associations between variables and dengue fever. Among the 194 confirmed cases, males aged 30–59 years (98, 50.5%) were the most affected, with fever (100%), headache (55.2%), and myalgia (49%) being the most common clinical presentations. The case fatality rate was 0.5%. Living in Sohar, particularly in Tareef, Humbar, and Waqaiba, was associated with higher susceptibility to dengue fever (OR = 5.40; 95% CI: 2.17–13.44) due to high vector density, and a history of travel was also identified as a significant risk factor (OR = 3.53; 95% CI: 1.60–7.75). The 2023 dengue fever outbreak was the largest recorded, highlighting the importance of proper removal of breeding sites, community health education, continued implementation of vector control strategies, and maintaining updated vector-borne disease surveillance.},
year = {2026}
}
TY - JOUR T1 - Dengue Fever Outbreak in North AL Batinah Governorate (Oman), January 2023 –December 2023 AU - Malik Aljabri AU - Eman Elsayed Abd-Ellatif AU - Fatma Al Hashmi AU - Khalid Al Saadi AU - Abir Al Moqbali Y1 - 2026/03/23 PY - 2026 N1 - https://doi.org/10.11648/j.ajmst.20260202.14 DO - 10.11648/j.ajmst.20260202.14 T2 - American Journal of Medical Science and Technology JF - American Journal of Medical Science and Technology JO - American Journal of Medical Science and Technology SP - 57 EP - 69 PB - Science Publishing Group UR - https://doi.org/10.11648/j.ajmst.20260202.14 AB - In the North Batinah Governorate, Sultanate of Oman, a local transmission dengue fever outbreak was examined based on surveillance data from January 1 to December 31, 2023, and containment measures were implemented. This study aimed to determine the sources and factors associated with this outbreak and to recommend countermeasures to prevent future outbreaks. A descriptive analysis was conducted on 194 confirmed cases, followed by an unmatched case-control study involving 194 laboratory-confirmed cases and 194 controls. Data were collected using the standardized dengue fever questionnaire developed by the Oman Ministry of Health, the electronic surveillance system (ALSHIFA+), and phone interviews. Multivariate analysis was performed to examine associations between variables and dengue fever. Among the 194 confirmed cases, males aged 30–59 years (98, 50.5%) were the most affected, with fever (100%), headache (55.2%), and myalgia (49%) being the most common clinical presentations. The case fatality rate was 0.5%. Living in Sohar, particularly in Tareef, Humbar, and Waqaiba, was associated with higher susceptibility to dengue fever (OR = 5.40; 95% CI: 2.17–13.44) due to high vector density, and a history of travel was also identified as a significant risk factor (OR = 3.53; 95% CI: 1.60–7.75). The 2023 dengue fever outbreak was the largest recorded, highlighting the importance of proper removal of breeding sites, community health education, continued implementation of vector control strategies, and maintaining updated vector-borne disease surveillance. VL - 2 IS - 2 ER -
Department of Disease Surveillance and Prevention, Ministry of Health, Sohar, Oman
Department of Public Health and Community Medicine, Mansoura University, Mansoura, Egypt
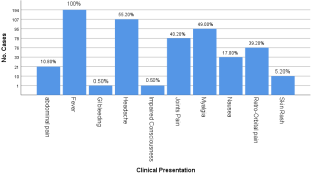
Figure 1. Distribution of dengue fever (DF) cases by clinical features during the 2023 outbreak in North Al Batinah Governorate (Oman).
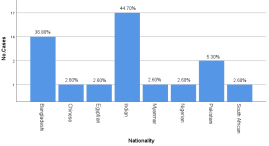
Figure 2. Nationalities among non-Omani dengue fever (DF) cases during the 2023 outbreak in North Al Batinah Governorate (Oman).
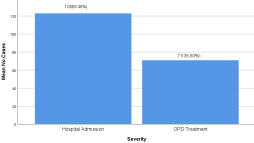
Figure 3. Distribution of DF cases during the 2023 outbreak in North Al Batinah Governorate (Oman) by severity.
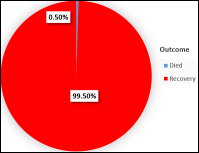
Figure 4. Distribution of DF cases by clinical outcome during the 2023 outbreak in North Al Batinah Governorate (Oman).
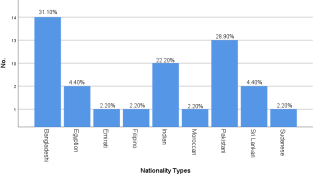
Figure 5. Nationalities among non-Omani individuals in the control group.
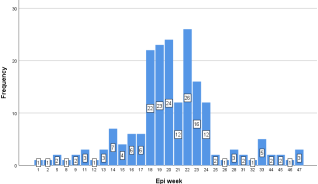
Figure 6. Epidemic curve of DF cases by week during the 2023 outbreak in North Al Batinah Governorate (Oman).
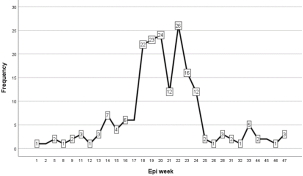
Figure 7. Line graph showing the epidemic curve of DF cases by week during the 2023 outbreak in North Al Batinah Governorate (Oman).
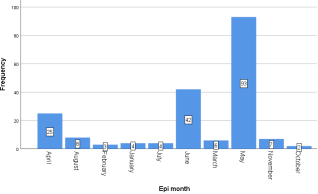
Figure 8. Epidemic curve of DF cases by month during the 2023 outbreak in North Al Batinah Governorate (Oman).
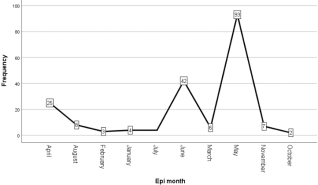
Figure 9. Line graph showing the epidemic curve of DF cases by month during the 2023 outbreak in North Al Batinah Governorate (Oman).
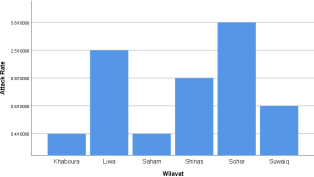
Figure 10. Distribution of DF attack rate by wilayat during the 2023 outbreak in North AL Batinah Governorate (Oman).
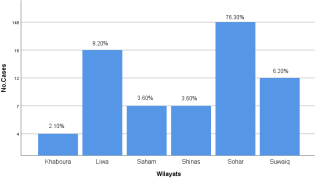
Figure 11. Distribution of DF cases by wilayat during the 2023 outbreak in North AL Batinah Governorate outbreak (Oman).
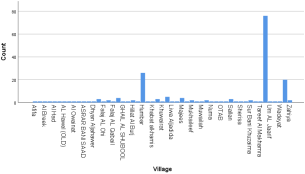
Figure 12. Distribution of DF cases by village during the 2023 outbreak in North AL Batinah Governorate (Oman).
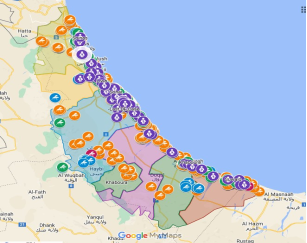
Figure 13. Map showing the distribution of DF Cases and Vectors during the 2023 outbreak in North AL Batinah Governorate (Oman).
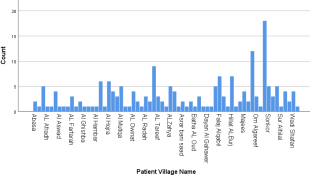
Figure 14. Distribution of DF controls by village during the 2023 outbreak in North AL Batinah Governorate (Oman).
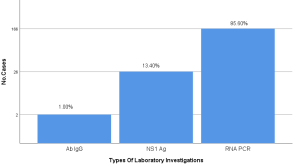
Figure 15. Distribution of cases of DF by type of laboratory investigation during the 2023 outbreak in North AL Batinah Governorate (Oman).
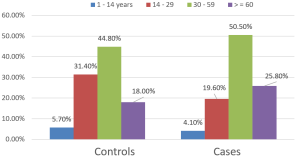
Figure 16. Distribution of age categories among DF cases and controls.
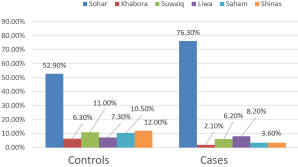
Figure 17. Distribution of Wilayates among DF cases and controls.
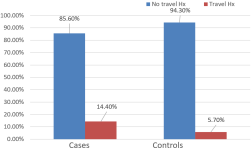
Figure 18. Distribution of DF cases and controls based on history of travel.
Information

