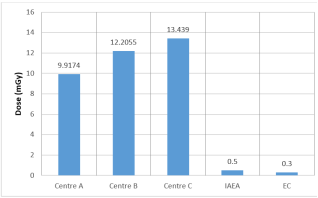
The increasing use of computed tomography (CT) in medical imaging has raised concerns regarding patient exposure to ionizing radiation, necessitating continuous evaluation of dose levels and optimization practices. This study presents a combined assessment of patient radiation dose and protection parameters during general and head CT examinations in selected diagnostic centers in Nigeria, utilizing Optically Stimulated Luminescence Dosimeters (OSLDs) for direct dose measurement. A retrospective analysis of 30 patients was conducted to evaluate skin dose during general CT examinations across three centers (A, B, and C), while a prospective study of 60 adult patients assessed head CT dose indices, including CTDIvol, CTDIw, dose length product (DLP), and effective dose. The mean skin doses for general CT were 9.92 mGy, 12.21 mGy, and 13.44 mGy for Centers A, B, and C respectively, corresponding to estimated effective doses of 0.15 mSv, 0.18 mSv, and 0.20 mSv. For head CT examinations, mean CTDIvol values ranged from 47.83 to 52.52 mGy, while mean DLP values varied from 1080.71 to 1485.48 mGy·cm, with effective doses between 2.49 and 3.17 mSv. Significant inter-center variations were observed, with general CT dose variability largely attributed to operator-dependent factors, whereas differences in head CT doses were primarily influenced by scan length and protocol implementation. Third-quartile values were used to establish local diagnostic reference levels (DRLs), which were higher than some international benchmarks but consistent with findings from similar healthcare settings. The study highlights the need for standardized CT protocols, routine dose monitoring, and strict adherence to the ALARA principle to enhance patient radiation protection while maintaining diagnostic image quality.
| Published in | American Journal of Physics and Applications (Volume 14, Issue 3) |
| DOI | 10.11648/j.ajpa.20261403.11 |
| Page(s) | 32-39 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Computed Tomography, Skin Dose, CTDIvol, Dose Length Product, Effective Dose, Diagnostic Reference Levels (DRLs)
S/n | Center A | Center B | Center C |
|---|---|---|---|
1 | 4.79 | 5.35 | 6.56 |
2 | 11.85 | 4.22 | 6.56 |
3 | 4.68 | 11.56 | 8.35 |
4 | 13.65 | 4.22 | 12.50 |
5 | 20.50 | 11.85 | 6.76 |
6 | 12.50 | 20.34 | 9.56 |
7 | 5.50 | 33.45 | 13.40 |
8 | 4.65 | 8.13 | 9.56 |
9 | 12.60 | 16.39 | 13.45 |
10 | 8.45 | 6.55 | 7.55 |
Parameter | Center A | Center B | Center C |
|---|---|---|---|
Minimum (mGy) | 4.65 | 4.22 | 6.56 |
Maximum (mGy) | 20.50 | 33.45 | 13.45 |
Mean (mGy) | 9.92 | 12.21 | 13.44 |
Range (mGy) | 15.85 | 29.23 | 6.89 |
Standard Deviation (mGy) | 5.5 | 9.2 | 2.6 |
S/n | CTDIv for the Head | ||
|---|---|---|---|
Centre A (mGy) | Centre B (mGy) | Centre C (mGy) | |
1 | 51.3 | 51.3 | 42.56 |
2 | 51.3 | 51.3 | 61.59 |
3 | 51.3 | 52.5 | 62.42 |
4 | 52.3 | 51.3 | 41.82 |
5 | 51.3 | 52.5 | 42.62 |
6 | 52.3 | 52.5 | 46.00 |
7 | 51.3 | 60.5 | 70.86 |
8 | 51.3 | 60.5 | 46.21 |
9 | 52.3 | 51.3 | 44.78 |
10 | 51.3 | 51.3 | 21.21 |
MEAN | 51.60 | 53.50 | 48.01 |
MAX | 52.30 | 60.50 | 70.86 |
MIN | 51.30 | 51.30 | 21.21 |
S/N | Centre A (mGy.cm) | Centre B (mGy.cm) | Centre C (mGy.cm) |
|---|---|---|---|
1 | 1066.9 | 1862.1 | 936.36 |
2 | 1759.4 | 1349.1 | 1577.88 |
3 | 1708.1 | 1932.5 | 1599.07 |
4 | 1597 | 14.37 | 1087.45 |
5 | 1092 | 1748.6 | 1193.28 |
6 | 1143.6 | 1879.9 | 1196.05 |
7 | 1374.7 | 1490.8 | 20.98 |
8 | 1656.8 | 1430.3 | 1109.12 |
9 | 1512.3 | 1041.3 | 985.25 |
10 | 1066.9 | 1836.4 | 426.85 |
MAEN | 1.397.77 | 1.458.54 | 1013.23 |
MAX | 1.759.40 | 1.932.50 | 1.599.07 |
MIN | 1.066.90 | 14.37 | 20.98 |
Effective Dose to the Head (mSv) | |||
|---|---|---|---|
S/N | Centre A | Centre B | Centre C |
1 | 4.28 | 2.15 | 2.15 |
2 | 3.10 | 3.63 | 3.63 |
3 | 4.44 | 3.68 | 3.68 |
4 | 0.03 | 2.50 | 2.50 |
5 | 4.02 | 2.74 | 2.74 |
6 | 4.32 | 2.75 | 2.75 |
7 | 3.43 | 0.05 | 0.05 |
8 | 3.29 | 2.55 | 2.55 |
9 | 2.39 | 2.27 | 2.27 |
10 | 4.22 | 0.98 | 0.98 |
MEAN | 3.35 | 2.33 | 2.33 |
MAX | 4.44 | 3.68 | 3.68 |
Body region CTDIv (mGy) | DLP (mGy.cm) | |||||||
|---|---|---|---|---|---|---|---|---|
Head | Min. Value | Mean ± SD | Max. Value | 3rdquartile | Min. Value | Mean ± SD | Max Value | 3rdquartile |
A | 41.3 | 51.9±3.7 | 60.5 | 52.3 | 1015.70 | 1485.5±360.8 | 2125.80 | 1782.6 |
B | 51.30 | 52.5±2.8 | 60.5 | 52.5 | 14.4 | 1376.3±547.7 | 1932.5 | 1794.9 |
C | 21.1 | 47.8±10.6 | 70.9 | 52.7 | 20.9 | 1080.71±381.8 | 1762.6 | 1209.1 |
OSLD | Optically Stimulated Dosimeter |
CT | Computed Tomography |
DRLs | Diagnostic Reference Levels |
CTDIv | Represents the Volume Computed Tomography Dose Index |
DLP | Dose Length Product |
ALARA | As Low As Reasonably Achievable |
ICRP | The International Commission on Radio-logical Protection |
UNSCEAR | United Nations Scientific Committee on the Effects of Atomic Radiation |
| [1] | Kalender WA. Computed Tomography: Fundamentals, System Technology, Image Quality, Applications. 3rd ed. Erlangen: Publicis Publishing; 2011. |
| [2] | Abuzaid, M. M., Elzain, M. E., Aljubairy, A. A., Alshamrani, K. M., & Alshamrani, G. M. (2020). Establishment of diagnostic reference levels for computed tomography examinations in the United Arab Emirates. Insights into Imaging, 11(1), 1–10. |
| [3] | Adejoh, T., & Nzotta, C. C. (2016). Head computed tomography: Dose output and optimization in a Nigerian tertiary hospital. West African Journal of Radiology, 23(2), 87–93. |
| [4] | Adejoh, T., Umar, I. M., & Yusuf, M. A. (2022). Assessment of patient radiation dose from computed tomography examinations in selected Nigerian hospitals. Radiation Protection Dosimetry, 198(3), 245–253. |
| [5] | Al Suwaidi, J. S., Al Naemi, H., Al Kuwari, H., & Al Kaabi, M. (2024). Establishment of diagnostic reference levels for computed tomography examinations in Qatar. Biomedicines, 12(11), 2446. |
| [6] | Bernner,,D.J.,& Hall, E.J.(2007).Computed Tomography an increasing source of Radiation Exposure. New England Journal of Medicine, 357(22), 2277–2284. |
| [7] | Tomography (EUR 16262 EN). Office for Official Publications of the European Communities. International Commission on Radiological Protection (ICRP). (2007). The 2007 recommendations of the International Commission on Radiological Protection (ICRP Publication 103). |
| [8] | International Commission on Radiological Protection (ICRP). (2017). Diagnostic reference levels in medical imaging (ICRP Publication 135). |
| [9] | McCollough, C. H., & Schueler, B. A. (2000). Calculation of effective dose. Medical Physics, 27(5), 828–837. |
| [10] | Ngaram, N., & Mohammed, I. M. (2019). Assessment of radiation dose from computed tomography examinations in northern Nigeria. International Journal of Medical Physics, Clinical Engineering and Radiation Oncology, 8(4), 375–385. |
| [11] | Sadiq, A. A., Musa, B. G., & Garba, I. (2020). Evaluation of radiation doses from CT examinations in northern Nigeria. Journal of Radiological Protection, 40(4), 1023–1035. |
| [12] | United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). (2021). Sources, effects and risks of ionizing radiation. United Nations. |
| [13] | European Commission. European Guidelines on Quality Criteria for Computed Tomography. EUR 16262 EN. Luxembourg; 1999. |
APA Style
Yemisi, I., Okafor, T. H., Pada, I., Samson, O. O., Abdul-Jamiu, A., et al. (2026). Optimization of Patient Radiation Protection and Dose Levels in Some Nigerian CT Facilities Using OSL Dosimetry. American Journal of Physics and Applications, 14(3), 32-39. https://doi.org/10.11648/j.ajpa.20261403.11
ACS Style
Yemisi, I.; Okafor, T. H.; Pada, I.; Samson, O. O.; Abdul-Jamiu, A., et al. Optimization of Patient Radiation Protection and Dose Levels in Some Nigerian CT Facilities Using OSL Dosimetry. Am. J. Phys. Appl. 2026, 14(3), 32-39. doi: 10.11648/j.ajpa.20261403.11
@article{10.11648/j.ajpa.20261403.11,
author = {Ilupeju Yemisi and Tobenna Henry Okafor and Isaac Pada and Odeleye Olagoke Samson and Aribisala Abdul-Jamiu and Sunday Habila Sarki},
title = {Optimization of Patient Radiation Protection and Dose Levels in Some Nigerian CT Facilities Using OSL Dosimetry},
journal = {American Journal of Physics and Applications},
volume = {14},
number = {3},
pages = {32-39},
doi = {10.11648/j.ajpa.20261403.11},
url = {https://doi.org/10.11648/j.ajpa.20261403.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpa.20261403.11},
abstract = {The increasing use of computed tomography (CT) in medical imaging has raised concerns regarding patient exposure to ionizing radiation, necessitating continuous evaluation of dose levels and optimization practices. This study presents a combined assessment of patient radiation dose and protection parameters during general and head CT examinations in selected diagnostic centers in Nigeria, utilizing Optically Stimulated Luminescence Dosimeters (OSLDs) for direct dose measurement. A retrospective analysis of 30 patients was conducted to evaluate skin dose during general CT examinations across three centers (A, B, and C), while a prospective study of 60 adult patients assessed head CT dose indices, including CTDIvol, CTDIw, dose length product (DLP), and effective dose. The mean skin doses for general CT were 9.92 mGy, 12.21 mGy, and 13.44 mGy for Centers A, B, and C respectively, corresponding to estimated effective doses of 0.15 mSv, 0.18 mSv, and 0.20 mSv. For head CT examinations, mean CTDIvol values ranged from 47.83 to 52.52 mGy, while mean DLP values varied from 1080.71 to 1485.48 mGy·cm, with effective doses between 2.49 and 3.17 mSv. Significant inter-center variations were observed, with general CT dose variability largely attributed to operator-dependent factors, whereas differences in head CT doses were primarily influenced by scan length and protocol implementation. Third-quartile values were used to establish local diagnostic reference levels (DRLs), which were higher than some international benchmarks but consistent with findings from similar healthcare settings. The study highlights the need for standardized CT protocols, routine dose monitoring, and strict adherence to the ALARA principle to enhance patient radiation protection while maintaining diagnostic image quality.},
year = {2026}
}
TY - JOUR T1 - Optimization of Patient Radiation Protection and Dose Levels in Some Nigerian CT Facilities Using OSL Dosimetry AU - Ilupeju Yemisi AU - Tobenna Henry Okafor AU - Isaac Pada AU - Odeleye Olagoke Samson AU - Aribisala Abdul-Jamiu AU - Sunday Habila Sarki Y1 - 2026/05/26 PY - 2026 N1 - https://doi.org/10.11648/j.ajpa.20261403.11 DO - 10.11648/j.ajpa.20261403.11 T2 - American Journal of Physics and Applications JF - American Journal of Physics and Applications JO - American Journal of Physics and Applications SP - 32 EP - 39 PB - Science Publishing Group SN - 2330-4308 UR - https://doi.org/10.11648/j.ajpa.20261403.11 AB - The increasing use of computed tomography (CT) in medical imaging has raised concerns regarding patient exposure to ionizing radiation, necessitating continuous evaluation of dose levels and optimization practices. This study presents a combined assessment of patient radiation dose and protection parameters during general and head CT examinations in selected diagnostic centers in Nigeria, utilizing Optically Stimulated Luminescence Dosimeters (OSLDs) for direct dose measurement. A retrospective analysis of 30 patients was conducted to evaluate skin dose during general CT examinations across three centers (A, B, and C), while a prospective study of 60 adult patients assessed head CT dose indices, including CTDIvol, CTDIw, dose length product (DLP), and effective dose. The mean skin doses for general CT were 9.92 mGy, 12.21 mGy, and 13.44 mGy for Centers A, B, and C respectively, corresponding to estimated effective doses of 0.15 mSv, 0.18 mSv, and 0.20 mSv. For head CT examinations, mean CTDIvol values ranged from 47.83 to 52.52 mGy, while mean DLP values varied from 1080.71 to 1485.48 mGy·cm, with effective doses between 2.49 and 3.17 mSv. Significant inter-center variations were observed, with general CT dose variability largely attributed to operator-dependent factors, whereas differences in head CT doses were primarily influenced by scan length and protocol implementation. Third-quartile values were used to establish local diagnostic reference levels (DRLs), which were higher than some international benchmarks but consistent with findings from similar healthcare settings. The study highlights the need for standardized CT protocols, routine dose monitoring, and strict adherence to the ALARA principle to enhance patient radiation protection while maintaining diagnostic image quality. VL - 14 IS - 3 ER -
Department of Medical Physics, National Hospital, Abuja, Nigeria
Department of Radiology, NHS Hospital, Gloucestershire, United Kingdom
Department of Medical Physics, National Hospital, Abuja, Nigeria
Department of Radiology, University of Maiduguri Teaching Hospital, Maiduguri, Nigeria
Department of Physics, Nasarawa State University, Keffi, Nigeria
Department of Physics, Nasarawa State University, Keffi, Nigeria
Information