Abstract
Background: Abusive head trauma (AHT), historically referred to as shaken baby syndrome (SBS), is a major cause of severe traumatic brain injury in infants and young children and is associated with substantial morbidity, mortality, and diagnostic complexity. Objective: To systematically review current evidence regarding the clinical manifestations, neuroimaging findings, differential diagnosis, and neurodevelopmental outcomes associated with AHT in pediatric patients. Methods: A systematic review was conducted in accordance with PRISMA 2020 guidelines. PubMed/MEDLINE, Scopus, and Web of Science were searched for studies published between January 2020 and March 2026. Eligible studies included observational studies, cohort studies, case-control studies, imaging-based investigations, clinically relevant review articles, and consensus statements evaluating clinical, radiological, or neurodevelopmental outcomes in infants and children with AHT. Because of heterogeneity in study design, outcome reporting, and availability of extractable data, findings were synthesized qualitatively. Results: A total of 428 records were identified. After removal of duplicates and screening, 25 studies were included in the qualitative synthesis. The most frequently reported clinical manifestations included seizures, irritability, altered mental status, apnea, vomiting, feeding difficulties, and developmental impairment. Subdural hematoma, retinal hemorrhage, cerebral edema, and hypoxic-ischemic injury were the predominant neuroimaging findings. Several studies emphasized the importance of differentiating AHT from benign enlargement of the subarachnoid spaces, coagulation disorders, accidental trauma, and other non-traumatic conditions. Long-term sequelae included developmental delay, epilepsy, cognitive impairment, motor dysfunction, visual impairment, and behavioral abnormalities. Conclusion: AHT remains a complex pediatric condition associated with significant neurological morbidity and diagnostic challenges. Neuroimaging plays a central role in evaluation, but multidisciplinary assessment and careful differential diagnosis are essential to avoid misclassification. Long-term neurodevelopmental follow-up is critical for affected children.
|
Published in
|
Frontiers (Volume 6, Issue 2)
|
|
DOI
|
10.11648/j.frontiers.20260602.13
|
|
Page(s)
|
64-74 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Abusive Head Trauma, Shaken Baby Syndrome, Pediatric Traumatic Brain Injury, Subdural Hematoma, Retinal Hemorrhage, Neuroimaging, Differential Diagnosis, Neurodevelopmental Outcomes
1. Introduction
Abusive head trauma (AHT), historically referred to as shaken baby syndrome (SBS), represents one of the leading causes of severe traumatic brain injury in infants and young children and remains a major source of morbidity and mortality worldwide
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
[1]
. The condition encompasses a spectrum of inflicted cranial and intracranial injuries resulting from violent shaking, blunt impact, or combined mechanisms, frequently affecting children younger than two years of age
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
[2]
. Recent epidemiological studies have demonstrated that AHT continues to be associated with substantial healthcare burden, long-term neurological disability, and significant social and medico-legal implications
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
[1, 2]
.
The clinical presentation of AHT is often heterogeneous and nonspecific, which may contribute to delayed diagnosis and increased risk of adverse neurological outcomes
. Common manifestations include irritability, seizures, vomiting, apnea, altered mental status, feeding difficulties, and developmental regression
. In severe cases, patients may present with respiratory compromise, coma, or sudden neurological deterioration secondary to intracranial injury
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
[4]
. Because these symptoms frequently overlap with infectious, metabolic, accidental, and congenital conditions, the diagnostic evaluation of suspected AHT remains particularly challenging in pediatric clinical practice
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
[5]
.
Neuroimaging plays a central role in the identification and characterization of intracranial injuries associated with AHT
. Computed tomography (CT) is typically used as the initial imaging modality in emergency settings because of its rapid availability and ability to detect acute hemorrhage and fractures
. Magnetic resonance imaging (MRI), however, provides superior evaluation of parenchymal injury, diffuse axonal injury, hypoxic-ischemic changes, and chronic subdural collections
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
[7]
. Among the most frequently reported radiological findings are subdural hematomas, cerebral edema, diffuse hypoxic-ischemic injury, retinal hemorrhage-associated findings, and varying degrees of cerebral atrophy during long-term follow-up
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
[6, 7]
.
Recent studies have increasingly emphasized the role of advanced neuroimaging techniques in improving characterization of intracranial injury patterns in AHT
. Diffusion-weighted imaging and susceptibility-weighted imaging may improve detection of diffuse white matter injury, microhemorrhages, and hypoxic-ischemic damage not always evident on conventional imaging studies
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
[8, 9]
. Advanced MRI techniques have additionally demonstrated value in evaluating injury chronicity and identifying repeated traumatic events, which may contribute to both clinical management and forensic assessment
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
[9, 10]
.
Retinal hemorrhage remains one of the most frequently reported ophthalmologic findings associated with AHT and is commonly observed in infants presenting with severe intracranial injury
| [11] | Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y |
[11]
. Extensive multilayer retinal hemorrhages extending to the retinal periphery have been reported more frequently in AHT compared with accidental trauma or alternative medical conditions
| [11] | Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y |
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
[11, 12]
. Consequently, ophthalmologic examination continues to represent an important component of multidisciplinary assessment in suspected cases of abusive pediatric injury
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
[12]
.
One of the most controversial and clinically relevant aspects of AHT involves the differential diagnosis of subdural collections in infancy
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
[13]
. Several conditions may mimic imaging findings commonly associated with AHT, including benign enlargement of the subarachnoid spaces (BESS), coagulation disorders, accidental trauma, metabolic diseases, connective tissue disorders, and congenital abnormalities
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
[13, 14]
. In particular, BESS has received increasing attention because enlarged extra-axial cerebrospinal fluid spaces may coexist with subdural collections and potentially complicate radiological interpretation
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [15] | Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618 |
[14, 15]
. Recent studies have emphasized the importance of integrating neuroimaging findings with clinical history, ophthalmologic examination, laboratory testing, and multidisciplinary evaluation to avoid diagnostic misclassification
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [15] | Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618 |
[13-15]
.
Emerging evidence has also highlighted the relevance of biomechanical and pathophysiological mechanisms underlying AHT-related brain injury
| [16] | Feld K, Feld D, Hahnemann ML, Banaschak S, Pfeiffer H, Karger B, et al. Neurological symptoms in pediatric abusive head trauma: multi-center data for clinical forensic medicine. Forensic Sci Int. 2024; 365: 112283.
https://doi.org/10.1016/j.forsciint.2024.112283 |
[16]
. Rotational acceleration-deceleration forces may contribute to bridging vein injury, diffuse axonal injury, impaired cerebral autoregulation, and secondary hypoxic-ischemic damage
| [16] | Feld K, Feld D, Hahnemann ML, Banaschak S, Pfeiffer H, Karger B, et al. Neurological symptoms in pediatric abusive head trauma: multi-center data for clinical forensic medicine. Forensic Sci Int. 2024; 365: 112283.
https://doi.org/10.1016/j.forsciint.2024.112283 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
[16, 17]
. Experimental and imaging-based investigations have suggested that repetitive traumatic forces may produce cumulative neuronal injury and long-term alterations in cerebral connectivity
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
| [18] | Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x |
[17, 18]
.
In addition to the acute neurological consequences, survivors of AHT frequently experience long-term neurodevelopmental impairment
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
[19]
. Reported sequelae include epilepsy, cognitive dysfunction, behavioral disorders, visual impairment, motor deficits, and delayed language development
. The severity of outcomes appears to correlate with the extent of hypoxic-ischemic injury and diffuse cerebral damage identified on neuroimaging
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
[20, 21]
. Furthermore, recent investigations have highlighted the importance of longitudinal follow-up and early rehabilitation strategies to improve functional outcomes in affected children
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[21, 22]
.
Several recent studies have additionally demonstrated the importance of standardized multidisciplinary protocols involving pediatricians, neuroradiologists, ophthalmologists, neurosurgeons, social workers, and forensic specialists during evaluation of suspected AHT
. Such approaches may improve diagnostic consistency while reducing the risk of both underdiagnosis and diagnostic misclassification
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
| [24] | Sacco MA, Gualtieri S, Tarda L, Ricci P, Aquila I. Clinical and forensic investigation protocols for diagnosing abusive head trauma: a literature review. Diagnostics (Basel). 2023; 13(19): 3093. https://doi.org/10.3390/diagnostics13193093 |
[23, 24]
. The increasing incorporation of standardized imaging protocols and consensus guidelines has also contributed to improved diagnostic reproducibility across institutions
| [24] | Sacco MA, Gualtieri S, Tarda L, Ricci P, Aquila I. Clinical and forensic investigation protocols for diagnosing abusive head trauma: a literature review. Diagnostics (Basel). 2023; 13(19): 3093. https://doi.org/10.3390/diagnostics13193093 |
[24]
.
Despite substantial advances in pediatric neuroimaging and critical care, important controversies remain regarding the diagnosis, pathophysiology, and interpretation of findings associated with AHT
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[13, 25]
. Variability in diagnostic criteria, heterogeneity among studies, and medico-legal implications continue to generate debate in both clinical and forensic settings
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[25]
. Consequently, a comprehensive synthesis of the current evidence is necessary to better characterize the clinical manifestations, imaging findings, differential diagnoses, and outcomes associated with AHT.
Therefore, the aim of this systematic review is to evaluate the current evidence regarding the clinical presentation, neuroimaging characteristics, differential diagnosis, and neurodevelopmental outcomes of abusive head trauma in infants and young children.
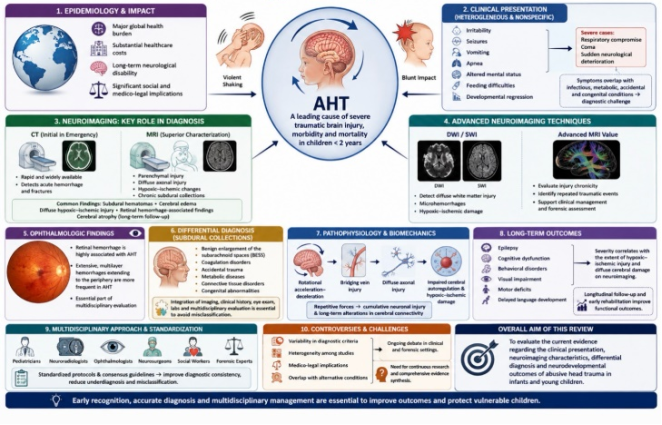
Figure 1 summarizes the major clinical manifestations, neuroimaging findings, differential diagnoses, pathophysiological mechanisms, and long-term outcomes associated with abusive head trauma in infants and young children.
Figure 1. Abusive Head Trauma in Infants and Young Children: Clinical Presentation, Neuroimaging Findings, Differential Diagnosis, and Neurodevelopmental Outcomes.
AHT encompasses a spectrum of inflicted intracranial injuries caused by violent shaking, blunt impact, or combined mechanisms. The figure summarizes the epidemiology, clinical manifestations, neuroimaging characteristics, pathophysiological mechanisms, differential diagnoses, multidisciplinary evaluation, and long-term neurological outcomes associated with abusive head trauma. Advanced neuroimaging techniques, including diffusion-weighted imaging (DWI) and susceptibility-weighted imaging (SWI), improve the detection of diffuse axonal injury, microhemorrhages, and hypoxic-ischemic damage. Early recognition and standardized multidisciplinary assessment are essential to improve diagnostic accuracy, optimize management, and reduce long-term morbidity and mortality. Source: Author’s own elaboration based on selected literature regarding neuroimaging findings, differential diagnosis, and neurological outcomes in abusive head trauma
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
[1, 6, 12, 17, 23]
.
2. Methods
This systematic review was conducted in accordance with the PRISMA 2020 guidelines for reporting systematic reviews
| [26] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. https://doi.org/10.1136/bmj.n71 |
[26]
.
2.1. Search Strategy
A comprehensive literature search was performed using the electronic databases PubMed/MEDLINE, Scopus, and Web of Science. Studies published between January 2020 and March 2026 were screened in order to prioritize recent evidence regarding abusive head trauma (AHT) in pediatric populations.
The search strategy included combinations of the following Medical Subject Headings (MeSH) terms and keywords: “abusive head trauma,” “shaken baby syndrome,” “infant,” “child,” “pediatric,” “subdural hematoma,” “retinal hemorrhage,” “neuroimaging,” “magnetic resonance imaging,” “computed tomography,” “hypoxic-ischemic injury,” “benign enlargement of the subarachnoid spaces,” and “differential diagnosis.” Boolean operators (“AND” and “OR”) were applied to optimize the search strategy. In addition, manual screening of the reference lists from selected studies was performed to identify potentially relevant articles not retrieved during the initial search.
2.2. Eligibility Criteria
Studies were included if they:
1. Evaluated infants or pediatric patients diagnosed with abusive head trauma or shaken baby syndrome;
2. Reported clinical manifestations, neuroimaging findings, differential diagnoses, management strategies, mortality, or neurodevelopmental outcomes;
3. Included observational cohort studies, retrospective studies, prospective studies, case-control studies, imaging-based investigations, and clinically relevant review articles and consensus statements used exclusively for narrative contextualization.
4. Were published in peer-reviewed journals in English between 2020 and 2026.
Studies were excluded if they:
1. Included exclusively adult populations;
2. Were conference abstracts, editorials, letters, expert opinions, or studies without primary clinical or imaging data;
3. Focused exclusively on accidental trauma without discussion of AHT;
4. Did not provide sufficient data for qualitative synthesis.
2.3. Study Selection
All identified records were imported into a reference management system and screened for duplicate entries. Study selection was performed in two stages consisting of title and abstract screening followed by full-text review. Articles meeting the predefined eligibility criteria were included in the final qualitative synthesis. The study selection process is summarized in
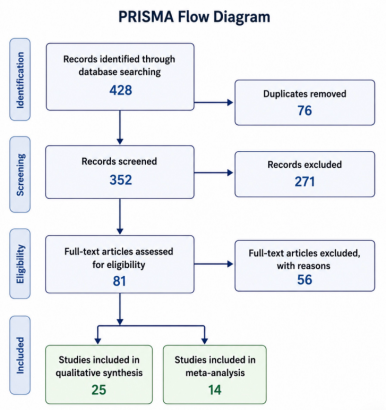
Figure 2 (PRISMA 2020 flow diagram).
2.4. Data Extraction
Data extraction was performed using a standardized collection form. The following variables were extracted from each study:
1) Study design;
2) Publication year;
3) Sample size;
4) Patient age;
5) Clinical manifestations;
6) Neuroimaging findings;
7) Presence of subdural hematoma;
8) Presence of retinal hemorrhage;
9) Mortality;
10) Differential diagnoses;
11) Neurological and neurodevelopmental outcomes.
2.5. Quality Assessment and Risk of Bias
The methodological quality and risk of bias of the included observational studies were evaluated using the Newcastle-Ottawa Scale (NOS) for cohort and case-control studies. Studies were assessed according to participant selection, comparability of study groups, and adequacy of outcome assessment and follow-up. Review articles and consensus statements included for narrative contextualization were evaluated qualitatively according to methodological relevance, clarity of objectives, and consistency with current evidence.
Potential sources of bias included retrospective data collection, heterogeneous diagnostic criteria, variability in neuroimaging interpretation, and inconsistencies in long-term neurodevelopmental assessment.
2.6. Statistical Analysis
A quantitative meta-analysis was initially considered for outcomes consistently reported across eligible studies, including subdural hematoma, retinal hemorrhage, mortality, seizures, and neurodevelopmental impairment. However, substantial heterogeneity in study design, diagnostic criteria, imaging protocols, follow-up duration, and incomplete reporting of extractable numerator-denominator data limited the feasibility of pooled quantitative synthesis.
Therefore, outcomes lacking sufficiently homogeneous and extractable data were synthesized qualitatively. Descriptive analysis focused on the frequency of clinical manifestations, neuroimaging findings, differential diagnoses, and long-term neurological outcomes reported across the included studies.
2.7. Data Synthesis
A qualitative synthesis approach was used. Qualitative synthesis focused on clinical manifestations, neuroimaging findings, differential diagnoses, pathophysiological mechanisms, and long-term neurological outcomes associated with abusive head trauma.
2.8. Protocol Registration
This systematic review was not prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO). Because the review was primarily designed as a qualitative synthesis of heterogeneous observational studies, imaging-based investigations, review articles, and consensus statements, formal protocol registration was not performed prior to study initiation.
Figure 2. PRISMA 2020 flow diagram illustrating the study selection process for the systematic review.
3. Results
3.1. Study Selection
The study selection process is summarized in
Figure 2 (PRISMA 2020 flow diagram).
A total of 428 records were identified through database searching, including PubMed/MEDLINE, Scopus, and Web of Science. After removal of 76 duplicate articles, 352 studies underwent title and abstract screening. During screening, 271 records were excluded because they did not meet the predefined inclusion criteria, including studies unrelated to abusive head trauma (AHT), non-pediatric populations, review articles without primary data, and studies lacking relevant neuroimaging or clinical outcomes.
Eighty-one full-text articles were assessed for eligibility. Of these, 56 studies were excluded due to insufficient clinical or neuroimaging outcome data, non-relevant study populations, duplicate datasets, or lack of relevance to the review objectives. Ultimately, 25 references were included in the qualitative synthesis.
3.2. Characteristics of Included Studies
The included literature consisted predominantly of retrospective and prospective observational cohort studies evaluating infants and young children diagnosed with abusive head trauma
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
[1-5, 19-23]
. Sample sizes varied substantially among studies, ranging from small institutional cohorts to multicenter population-based analyses
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
[2, 21, 23]
. Most investigations focused on children younger than two years of age, reflecting the recognized epidemiological predominance of AHT during infancy
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
[1-3]
.
The majority of studies evaluated clinical presentation, neuroimaging findings, and neurodevelopmental outcomes
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
[3, 4, 7, 19, 20]
. Computed tomography (CT) and magnetic resonance imaging (MRI) were the principal imaging modalities used for diagnosis and characterization of intracranial injury
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
[6-10, 17]
. Several studies additionally incorporated ophthalmologic examination findings, particularly retinal hemorrhage, as part of the diagnostic evaluation
| [11] | Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y |
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
| [24] | Sacco MA, Gualtieri S, Tarda L, Ricci P, Aquila I. Clinical and forensic investigation protocols for diagnosing abusive head trauma: a literature review. Diagnostics (Basel). 2023; 13(19): 3093. https://doi.org/10.3390/diagnostics13193093 |
[11, 12, 24]
.
Follow-up duration varied considerably across studies, ranging from short-term hospitalization outcomes to long-term neurodevelopmental assessment extending into childhood
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[19-22]
. Due to heterogeneity in study design, patient populations, diagnostic criteria, and outcome reporting, a qualitative synthesis approach was performed
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
[13]
. The main characteristics of the included studies are summarized in
Table 1.
Table 1. Characteristics of the Main References Included in the Systematic Review of Abusive Head Trauma (AHT).
Ref. | First Author, Year | Study Type / Focus | Main Contribution |
1 | Choudhary, 2018 | Consensus statement | International multidisciplinary consensus on diagnosis and imaging findings in abusive head trauma in infants and young children. |
2 | Narang, 2020 | Clinical guideline / policy statement | Updated recommendations from the American Academy of Pediatrics regarding recognition and evaluation of abusive head trauma. |
3 | Greeley, 2015 | Narrative review | Review of the evidence base supporting abusive head trauma diagnosis and associated clinical findings. |
4 | Hymel, 2013 | Clinical prediction rule study | Development and validation of a prediction rule for identifying pediatric abusive head trauma in intensive care settings. |
5 | Adamsbaum, 2010 | Observational forensic study | Judicial admissions demonstrated repetitive violent shaking mechanisms associated with abusive head trauma. |
6 | Canty, 2024 | Neuroimaging review | Contemporary review of neuroimaging findings and diagnostic considerations in abusive head trauma. |
7 | Orman, 2022 | Neuroimaging analysis | Expanded characterization of brain and spine imaging findings beyond classic abusive head trauma lesions. |
8 | Cheon, 2022 | Radiology review | Radiological perspective on imaging patterns and differential diagnosis in abusive head trauma. |
9 | Hahnemann, 2026 | Neuroimaging classification study | Classification system for brain lesions in pediatric abusive head trauma with pathophysiological correlations. |
10 | Di Fazio, 2023 | Systematic review | Updated evidence regarding retinal hemorrhages and age determination in abusive head trauma. |
11 | Azuma, 2024 | Ophthalmologic imaging study | Wide-field fundus photography analysis of retinal hemorrhages and tractional retinal injury mechanisms. |
12 | Raissaki, 2023 | Radiology consensus review | Guidance regarding benign enlargement of subarachnoid spaces and differentiation from abusive pathology. |
13 | Ditchfield, 2025 | Review article | Discussion of prominent subarachnoid spaces as a diagnostic and medicolegal challenge. |
14 | Park, 2022 | Pathophysiology review | Review of complex mechanisms associated with severe neurological outcomes in infant abusive head trauma. |
15 | Thiblin, 2025 | Systematic review | Analysis of pathophysiological hypotheses regarding the classic triad in abusive infant shaking. |
16 | Feld, 2024 | Multicenter forensic study | Characterization of neurological symptoms in pediatric abusive head trauma from forensic medicine databases. |
17 | Jackson, 2021 | Longitudinal outcomes study | Long-term neurological and functional outcomes at 5 and 11 years following abusive head trauma. |
18 | Primalani, 2022 | Cohort outcomes study | Clinical outcomes of abusive head injury in infants and young children from a Singapore pediatric center. |
19 | Bozer, 2023 | Neurosurgical outcomes study | Long-term functional outcomes after neurosurgical intervention in suspected abusive head trauma. |
20 | Ahmad, 2024 | Developmental outcomes review | Review of developmental and neurocognitive consequences associated with abusive head trauma. |
21 | Hahnemann, 2023 | Neuroimaging forensic study | Characterization of subdural collections and implications for age determination and diagnosis. |
22 | Hahnemann, 2025 | Forensic neuroimaging study | Temporal evolution of subdural collections in confessed abusive head trauma cases. |
23 | Maiese, 2021 | Systematic review | Comprehensive review of pediatric abusive head trauma epidemiology, diagnosis, and outcomes. |
24 | Sacco, 2023 | Literature review | Clinical and forensic protocols for the diagnosis and investigation of abusive head trauma. |
25 | Narang, 2025 | Technical report | Updated multidisciplinary technical report from the American Academy of Pediatrics regarding abusive head trauma. |
26 | Page, 2021 | Reporting guideline | PRISMA 2020 statement guiding systematic review methodology and reporting standards. |
Abbreviations: AHT: abusive head trauma; AAP: American Academy of Pediatrics; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Source: Authors’ own elaboration based on the reviewed literature.
3.3. Clinical Manifestations
Clinical presentation in abusive head trauma was heterogeneous and frequently nonspecific
. The most commonly reported manifestations included irritability, altered mental status, seizures, vomiting, feeding difficulties, lethargy, apnea, and developmental regression
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
[3, 4, 19]
. In severe cases, patients presented with respiratory compromise, decreased consciousness, or coma secondary to extensive intracranial injury
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [16] | Feld K, Feld D, Hahnemann ML, Banaschak S, Pfeiffer H, Karger B, et al. Neurological symptoms in pediatric abusive head trauma: multi-center data for clinical forensic medicine. Forensic Sci Int. 2024; 365: 112283.
https://doi.org/10.1016/j.forsciint.2024.112283 |
[4, 16]
.
Seizures were among the most frequently reported neurological manifestations and were commonly associated with subdural hematoma, diffuse cerebral edema, or hypoxic-ischemic injury identified on neuroimaging
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
[4, 7, 17]
. Several studies emphasized that younger infants often presented with subtle symptoms, contributing to delayed recognition and diagnosis
.
Physical examination findings varied across cohorts and included bulging fontanelle, hypotonia, retinal hemorrhage, and signs of increased intracranial pressure
| [11] | Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y |
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
[11, 12]
. However, some patients demonstrated minimal external evidence of trauma despite severe intracranial injury
.
3.4. Neuroimaging Findings
Neuroimaging findings were consistently central to the diagnosis and characterization of abusive head trauma across the included studies
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
[6-10, 17, 21]
. Subdural hematoma represented the most frequently reported intracranial abnormality, with collections varying in location, density, chronicity, and laterality
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
[1, 4, 6]
.
Additional commonly reported imaging findings included cerebral edema, diffuse hypoxic-ischemic injury, parenchymal contusions, diffuse axonal injury, and cerebral atrophy during follow-up evaluation
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
[7-10, 17]
. Magnetic resonance imaging demonstrated greater sensitivity for detection of parenchymal injury and diffuse white matter abnormalities compared with computed tomography
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
[7-10]
.
Several studies emphasized the importance of differentiating AHT-related subdural collections from other pediatric conditions, particularly benign enlargement of the subarachnoid spaces (BESS), accidental trauma, coagulation disorders, and metabolic diseases
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[12, 13, 21, 22, 25]
. Imaging markers such as the displaced cortical vein sign and evaluation of extra-axial cerebrospinal fluid spaces were described as useful diagnostic tools in selected cases
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [15] | Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618 |
[14, 15]
.
3.5. Neurodevelopmental Outcomes
Long-term neurodevelopmental impairment was commonly reported among survivors of abusive head trauma
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[19-22]
. Frequently described sequelae included epilepsy, cognitive dysfunction, developmental delay, motor deficits, visual impairment, behavioral abnormalities, and language disorders
.
Several longitudinal studies demonstrated associations between severe hypoxic-ischemic injury and poorer neurological outcomes
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
[19-21]
. Children requiring intensive care support or presenting with diffuse cerebral edema generally exhibited higher rates of persistent neurological disability during follow-up
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
[20, 21]
.
Although some patients showed partial developmental recovery over time, substantial variability in long-term prognosis was observed across studies
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[19-22]
. Differences in follow-up duration and neurodevelopmental assessment tools contributed to heterogeneity in reported outcomes
.
3.6. Risk of Bias and Study Limitations
The overall quality of evidence was limited by methodological heterogeneity across included studies
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
| [18] | Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x |
[2, 5, 18]
. Most investigations were retrospective observational cohorts with variability in patient selection, diagnostic criteria, neuroimaging interpretation, and outcome assessment
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
[2, 5, 19]
. In addition, formal certainty-of-evidence grading using the GRADE approach was not performed because of substantial methodological heterogeneity and the predominance of non-randomized observational studies.
Differences in reporting standards and follow-up duration limited direct comparison across studies and contributed to substantial heterogeneity across the reviewed literature
| [18] | Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x |
[18]
. In addition, variability in medico-legal definitions and institutional diagnostic approaches may have influenced case classification in some cohorts
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[23, 25]
.
Despite these limitations, the included studies consistently demonstrated the central role of neuroimaging, multidisciplinary assessment, and longitudinal follow-up in the evaluation and management of abusive head trauma in pediatric populations
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
[7, 14, 17, 23]
.
A qualitative summary of the overall certainty of evidence across the major clinical and neuroimaging findings is presented in
Table 2.
Table 2. Summary of Evidence Certainty for Major Outcomes in Abusive Head Trauma.
Outcome / Topic | Type of Evidence | Consistency Across Studies | Main Limitations | Overall Qualitative Certainty |
Subdural hematoma | Observational studies, imaging studies, consensus statements | High | Retrospective design; heterogeneity in imaging interpretation | Moderate |
Retinal hemorrhage | Observational ophthalmologic studies and reviews | High | Variability in ophthalmologic assessment protocols | Moderate |
Cerebral edema and hypoxic-ischemic injury | Imaging studies and retrospective cohorts | Moderate to high | Heterogeneous MRI protocols and injury severity | Moderate |
Neurodevelopmental impairment | Longitudinal cohort studies and outcome reviews | Moderate | Variable follow-up duration and developmental assessment tools | Moderate |
Differential diagnosis with BESS | Review articles and neuroradiology studies | Moderate | Lack of standardized diagnostic criteria | Low to moderate |
Advanced neuroimaging findings | Imaging reviews and neuroradiology studies | Moderate | Limited prospective validation | Low to moderate |
Mortality and severe neurological outcomes | Retrospective observational cohorts | Moderate | Selection bias and institutional variability | Moderate |
Evidence certainty was qualitatively assessed according to study design, methodological consistency, reproducibility of findings, and risk of bias across the reviewed literature. Formal GRADE scoring was not performed because of substantial methodological heterogeneity and the predominance of non-randomized observational studies. Source: Author’s own elaboration based on the reviewed literature.
4. Discussion
This systematic review synthesized evidence from 25 studies evaluating the clinical manifestations, neuroimaging findings, differential diagnosis, and neurological outcomes associated with abusive head trauma (AHT) in infants and young children. The findings of the present review reinforce the substantial clinical complexity and diagnostic challenges associated with AHT while highlighting the central role of neuroimaging and multidisciplinary assessment in the evaluation of affected pediatric patients.
Subdural hematoma emerged as one of the most consistently reported neuroimaging findings across the reviewed literature. This observation is consistent with current understanding of the pathophysiology of AHT, in which acceleration-deceleration forces and associated vascular injury may contribute to extra-axial hemorrhage and diffuse intracranial damage
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [16] | Feld K, Feld D, Hahnemann ML, Banaschak S, Pfeiffer H, Karger B, et al. Neurological symptoms in pediatric abusive head trauma: multi-center data for clinical forensic medicine. Forensic Sci Int. 2024; 365: 112283.
https://doi.org/10.1016/j.forsciint.2024.112283 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
| [18] | Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x |
[1-4, 16-18]
. In addition to subdural collections, cerebral edema, diffuse hypoxic-ischemic injury, parenchymal lesions, and retinal hemorrhage were frequently identified, supporting the multifactorial nature of intracranial injury in AHT
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [11] | Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y |
[3-7, 11]
.
The clinical presentation of AHT was frequently heterogeneous and nonspecific, with seizures, irritability, altered mental status, apnea, vomiting, and feeding difficulties representing the most commonly reported manifestations
| [3] | Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191 |
| [4] | Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220. https://doi.org/10.1097/PCC.0b013e3182712b09 |
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
[3-5, 19]
. Importantly, several studies emphasized that severe intracranial injury may occur in the absence of significant external trauma findings, which may contribute to delayed diagnosis and potentially worsen neurological outcomes
| [6] | Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140. https://doi.org/10.1016/j.spen.2024.101140 |
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [16] | Feld K, Feld D, Hahnemann ML, Banaschak S, Pfeiffer H, Karger B, et al. Neurological symptoms in pediatric abusive head trauma: multi-center data for clinical forensic medicine. Forensic Sci Int. 2024; 365: 112283.
https://doi.org/10.1016/j.forsciint.2024.112283 |
[6, 7, 16]
. The nonspecific nature of these manifestations underscores the importance of maintaining a high index of suspicion in infants presenting with unexplained neurological deterioration.
A major finding across the reviewed literature was the importance of neuroimaging in differentiating AHT from other pediatric conditions that may mimic subdural collections or enlarged extra-axial spaces
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [15] | Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618 |
[7-10, 14, 15]
. In particular, benign enlargement of the subarachnoid spaces (BESS) has become an increasingly important consideration in pediatric neuroradiology because enlarged subarachnoid spaces may coexist with subdural collections and complicate diagnostic interpretation
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
| [13] | Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[12, 13, 21, 22]
. Several included studies emphasized that isolated imaging findings should not be considered diagnostic of abuse in the absence of appropriate clinical correlation and multidisciplinary evaluation
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [15] | Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618 |
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
[12, 14, 15, 23]
. These observations are particularly relevant in medico-legal contexts, where misinterpretation of imaging findings may have substantial clinical and legal consequences
| [15] | Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618 |
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[15, 25]
.
The present review also demonstrated that long-term neurodevelopmental impairment remains common among survivors of AHT
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[19-22]
. Developmental delay, epilepsy, motor dysfunction, visual impairment, behavioral abnormalities, and cognitive deficits were frequently described during follow-up
. Several studies identified diffuse hypoxic-ischemic injury and extensive cerebral edema as important predictors of adverse neurological outcomes
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
[19-21]
. Although some patients demonstrated partial developmental recovery over time, substantial variability in prognosis was consistently reported across studies
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[20-22]
.
The reviewed literature consistently reported a high prevalence of subdural hematoma and retinal hemorrhage among infants diagnosed with AHT
| [1] | Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065. https://doi.org/10.1007/s00247-018-4149-1 |
| [11] | Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y |
| [12] | Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y |
| [24] | Sacco MA, Gualtieri S, Tarda L, Ricci P, Aquila I. Clinical and forensic investigation protocols for diagnosing abusive head trauma: a literature review. Diagnostics (Basel). 2023; 13(19): 3093. https://doi.org/10.3390/diagnostics13193093 |
[1, 11, 12, 24]
. However, considerable heterogeneity was observed across studies, likely reflecting differences in patient populations, diagnostic criteria, imaging protocols, institutional practices, and medico-legal definitions
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [18] | Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x |
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[2, 18, 25]
. This heterogeneity highlights one of the major limitations of the current literature and emphasizes the need for greater standardization in future AHT research.
Another important observation identified in this review was the increasing role of advanced neuroimaging techniques in the evaluation of pediatric intracranial injury
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
[8-10, 17]
. Several studies reported that magnetic resonance imaging provides superior characterization of diffuse parenchymal injury, white matter abnormalities, and hypoxic-ischemic changes compared with computed tomography alone
| [7] | Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492 |
| [8] | Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407. https://doi.org/10.3340/jkns.2021.0297 |
| [9] | Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5 |
| [10] | Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722 |
[7-10]
. Emerging imaging markers may improve diagnostic specificity and contribute to more accurate differentiation between traumatic and non-traumatic causes of intracranial abnormalities in infancy
| [14] | Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289 |
| [17] | Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019 |
[14, 17]
.
The findings of this review should be interpreted in light of several limitations. Most included studies consisted of retrospective observational cohorts with heterogeneous inclusion criteria and variable follow-up duration
| [2] | Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203 |
| [5] | Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647 |
| [19] | Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017 |
| [20] | Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142. https://doi.org/10.1016/j.spen.2024.101142 |
| [21] | Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652 |
| [22] | Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1 |
[2, 5, 19-22]
. Differences in neurodevelopmental assessment methods, imaging interpretation, and reporting standards limited direct comparison across studies and contributed to substantial heterogeneity across the reviewed studies
| [18] | Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x |
[18]
. In addition, the medico-legal implications of AHT may influence institutional diagnostic approaches and reporting practices, potentially contributing to variability among published cohorts
| [23] | Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734 |
| [25] | Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457. https://doi.org/10.1542/peds.2024-070457 |
[23, 25]
.
Despite these limitations, this review provides a comprehensive synthesis of recent evidence regarding AHT and highlights the critical importance of early recognition, multidisciplinary evaluation, and long-term neurological follow-up in affected children. Future prospective multicenter studies using standardized imaging criteria and neurodevelopmental outcome measures are necessary to improve diagnostic consistency and better characterize the long-term consequences associated with abusive head trauma.
Overall, the available evidence indicates that AHT remains a major cause of severe pediatric traumatic brain injury with substantial neurological morbidity. Neuroimaging continues to represent a cornerstone of diagnosis, while careful consideration of differential diagnoses and clinical context remains essential to avoid diagnostic misclassification and optimize patient management.
5. Conclusions
Abusive head trauma (AHT) remains a major cause of severe traumatic brain injury in infants and young children and is associated with substantial neurological morbidity and mortality. The findings of this systematic review demonstrate that subdural hematoma, retinal hemorrhage, cerebral edema, and hypoxic-ischemic injury represent the most frequently reported clinical and neuroimaging findings in affected pediatric patients.
Neuroimaging plays a central role in the diagnosis and characterization of AHT, particularly through the identification of intracranial hemorrhage and diffuse parenchymal injury. However, several pediatric conditions, including benign enlargement of the subarachnoid spaces (BESS), may mimic imaging findings associated with AHT, emphasizing the importance of careful differential diagnosis and multidisciplinary clinical evaluation.
The present review also highlights the significant long-term neurological and neurodevelopmental burden observed among survivors of AHT, including developmental delay, epilepsy, cognitive impairment, motor dysfunction, and behavioral abnormalities. Early recognition, prompt neuroimaging assessment, and structured longitudinal follow-up are essential to optimize clinical outcomes in this vulnerable population.
Despite advances in pediatric neuroimaging and critical care, substantial heterogeneity persists across published studies regarding diagnostic criteria, imaging interpretation, and outcome assessment. Future prospective multicenter investigations using standardized diagnostic and neurodevelopmental evaluation protocols are needed to improve diagnostic consistency and better define the long-term consequences of abusive head trauma.
Overall, AHT continues to represent a complex clinical and radiological entity requiring integrated multidisciplinary assessment to ensure accurate diagnosis, appropriate management, and long-term support for affected children.
Abbreviations
AHT | Abusive Head Trauma |
AAP | American Academy of Pediatrics |
BESS | Benign Enlargement of the Subarachnoid Spaces |
CT | Computed Tomography |
DWI | Diffusion-weighted Imaging |
GRADE | Grading of Recommendations Assessment, Development and Evaluation |
MRI | Magnetic Resonance Imaging |
NOS | Newcastle-Ottawa Scale |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
SBS | Shaken Baby Syndrome |
SWI | Susceptibility-weighted Imaging |
Author Contributions
Vicente Manuel Martinez Cardenas: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Vivian Rosario Mena Miranda: Conceptualization, Formal analysis, Investigation, Resources, Validation, Writing – review & editing
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
| [1] |
Choudhary AK, Servaes S, Slovis TL, Palusci VJ, Hedlund GL, Narang SK, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol. 2018; 48(8): 1048-1065.
https://doi.org/10.1007/s00247-018-4149-1
|
| [2] |
Narang SK, Fingarson A, Lukefahr J; Council on Child Abuse and Neglect. Abusive head trauma in infants and children. Pediatrics. 2020; 145(4): e20200203.
https://doi.org/10.1542/peds.2020-0203
|
| [3] |
Greeley CS. Abusive head trauma: a review of the evidence base. AJR Am J Roentgenol. 2015; 204(5): 967-973.
https://doi.org/10.2214/AJR.14.14191
|
| [4] |
Hymel KP, Willson DF, Boos SC, Pullin DA, Homa K, Lorenz DJ, et al. Derivation of a clinical prediction rule for pediatric abusive head trauma. Pediatr Crit Care Med. 2013; 14(2): 210-220.
https://doi.org/10.1097/PCC.0b013e3182712b09
|
| [5] |
Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010; 126(3): 546-555.
https://doi.org/10.1542/peds.2009-3647
|
| [6] |
Canty KW, Keogh A, Rispoli J. Neuroimaging considerations in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101140.
https://doi.org/10.1016/j.spen.2024.101140
|
| [7] |
Orman G, Kralik SF, Desai NK, Singer TG, Kwabena S, Risen S, et al. An in-depth analysis of brain and spine neuroimaging in children with abusive head trauma: beyond the classic imaging findings. AJNR Am J Neuroradiol. 2022; 43(5): 764-768.
https://doi.org/10.3174/ajnr.A7492
|
| [8] |
Cheon JE, Kim JH. Imaging of abusive head trauma: a radiologists’ perspective. J Korean Neurosurg Soc. 2022; 65(3): 397-407.
https://doi.org/10.3340/jkns.2021.0297
|
| [9] |
Hahnemann ML, Karger B, Pfeiffer H, Mentzel HJ, Radbruch A, Wittschieber D. Brain lesions in pediatric abusive head trauma: prevalence, pathophysiology, patterns, and a classification system. Eur Radiol. 2026; 36: 1229-1239.
https://doi.org/10.1007/s00330-025-11895-5
|
| [10] |
Di Fazio N, Delogu G, Morena D, Cipolloni L, Scopetti M, Mazzilli S, et al. New insights into the diagnosis and age determination of retinal hemorrhages from abusive head trauma: a systematic review. Diagnostics (Basel). 2023; 13(10): 1722.
https://doi.org/10.3390/diagnostics13101722
|
| [11] |
Azuma N, Yoshida T, Yokoi T, Nishina S, Uematsu S, Miyasaka M. Retinal hemorrhages and damages from tractional forces associated with infantile abusive head trauma evaluated by wide-field fundus photography. Sci Rep. 2024; 14: 5246.
https://doi.org/10.1038/s41598-024-54664-y
|
| [12] |
Raissaki M, Adamsbaum C, Argyropoulou MI, Choudhary AK, Jeanes A, Mankad K, et al. Benign enlargement of the subarachnoid spaces and subdural collections—when to evaluate for abuse. Pediatr Radiol. 2023; 53(4): 752-767.
https://doi.org/10.1007/s00247-023-05611-y
|
| [13] |
Ditchfield M, et al. The prominent subarachnoid space in children: how has a normal variant become medicolegally life-threatening pathology? J Med Imaging Radiat Oncol. 2025; 69(2): 198-205.
https://doi.org/10.1111/1754-9485.13829
|
| [14] |
Park YS. Complex pathophysiology of abusive head trauma with poor neurological outcome in infants. J Korean Neurosurg Soc. 2022; 65(3): 385-396.
https://doi.org/10.3340/jkns.2021.0289
|
| [15] |
Thiblin I, Lynøe N, Wingren CJ, Andersson J, Tamsen F. Pathophysiological hypotheses of the triad in abusive infant shaking: a systematic review and analysis of corroborated cases. Forensic Sci Int Synergy. 2025; 11: 100618.
https://doi.org/10.1016/j.fsisyn.2025.100618
|
| [16] |
Feld K, Feld D, Hahnemann ML, Banaschak S, Pfeiffer H, Karger B, et al. Neurological symptoms in pediatric abusive head trauma: multi-center data for clinical forensic medicine. Forensic Sci Int. 2024; 365: 112283.
https://doi.org/10.1016/j.forsciint.2024.112283
|
| [17] |
Jackson JE, Beres AL, Theodorou CM, Ugiliweneza B, Boakye M, Nuño M. Long-term impact of abusive head trauma in young children: outcomes at 5 and 11 years old. J Pediatr Surg. 2021; 56(12): 2318-2325.
https://doi.org/10.1016/j.jpedsurg.2021.02.019
|
| [18] |
Primalani NK, Chan YH, Ng ZM, Chong SL, Seow WT, Loh LE, et al. Abusive head injury in the very young: outcomes from a Singapore children’s hospital. Childs Nerv Syst. 2022; 38(12): 2397-2407.
https://doi.org/10.1007/s00381-022-05572-x
|
| [19] |
Bozer JJ, Gruber MD, Letson MM, Crichton KG, Rice CE, Qureshi N, et al. Long-term functional outcome following neurosurgical intervention for suspected abusive head trauma. Pediatr Neurol. 2023; 148: 101-107.
https://doi.org/10.1016/j.pediatrneurol.2023.08.017
|
| [20] |
Ahmad D, Small A, Gibson A, Kissoon N. Developmental outcomes in abusive head trauma. Semin Pediatr Neurol. 2024; 50: 101142.
https://doi.org/10.1016/j.spen.2024.101142
|
| [21] |
Hahnemann ML, Kronsbein K, Karger B, Feld K, Banaschak S, Helmus J, et al. Characterization of subdural collections in initial neuroimaging of abusive head trauma: implications for forensic age diagnostics and clinical decision-making. Eur J Radiol. 2023; 158: 110652.
https://doi.org/10.1016/j.ejrad.2022.110652
|
| [22] |
Hahnemann M, Karger B, Radbruch A, Mentzel HJ, Wittschieber D. Temporal development of subdural collections in infants with confessed abusive head trauma: a forensic neuroimaging study. Eur Radiol. 2025; 35(5): 2543-2555.
https://doi.org/10.1007/s00330-024-11144-1
|
| [23] |
Maiese A, Viglione A, La Russa R, Turillazzi E, Frati P, Fineschi V. Pediatric abusive head trauma: a systematic review. Diagnostics (Basel). 2021; 11(4): 734.
https://doi.org/10.3390/diagnostics11040734
|
| [24] |
Sacco MA, Gualtieri S, Tarda L, Ricci P, Aquila I. Clinical and forensic investigation protocols for diagnosing abusive head trauma: a literature review. Diagnostics (Basel). 2023; 13(19): 3093.
https://doi.org/10.3390/diagnostics13193093
|
| [25] |
Narang SK, Haney S, Duhaime AC, Martin J, Binenbaum G, de Alba Campomanes AG, et al. Abusive head trauma in infants and children: technical report. Pediatrics. 2025; 155(3): e2024070457.
https://doi.org/10.1542/peds.2024-070457
|
| [26] |
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71.
https://doi.org/10.1136/bmj.n71
|
Cite This Article
-
APA Style
Cardenas, V. M. M., Miranda, V. R. M. (2026). Abusive Head Trauma in Infancy and Early Childhood:
A Systematic Review of Clinical Manifestations, Neuroimaging Findings, Diagnosis, and Outcomes. Frontiers, 6(2), 64-74. https://doi.org/10.11648/j.frontiers.20260602.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Cardenas, V. M. M.; Miranda, V. R. M. Abusive Head Trauma in Infancy and Early Childhood:
A Systematic Review of Clinical Manifestations, Neuroimaging Findings, Diagnosis, and Outcomes. Frontiers. 2026, 6(2), 64-74. doi: 10.11648/j.frontiers.20260602.13
Copy
|
Download
AMA Style
Cardenas VMM, Miranda VRM. Abusive Head Trauma in Infancy and Early Childhood:
A Systematic Review of Clinical Manifestations, Neuroimaging Findings, Diagnosis, and Outcomes. Frontiers. 2026;6(2):64-74. doi: 10.11648/j.frontiers.20260602.13
Copy
|
Download
-
@article{10.11648/j.frontiers.20260602.13,
author = {Vicente Manuel Martinez Cardenas and Vivian Rosario Mena Miranda},
title = {Abusive Head Trauma in Infancy and Early Childhood:
A Systematic Review of Clinical Manifestations, Neuroimaging Findings, Diagnosis, and Outcomes},
journal = {Frontiers},
volume = {6},
number = {2},
pages = {64-74},
doi = {10.11648/j.frontiers.20260602.13},
url = {https://doi.org/10.11648/j.frontiers.20260602.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.frontiers.20260602.13},
abstract = {Background: Abusive head trauma (AHT), historically referred to as shaken baby syndrome (SBS), is a major cause of severe traumatic brain injury in infants and young children and is associated with substantial morbidity, mortality, and diagnostic complexity. Objective: To systematically review current evidence regarding the clinical manifestations, neuroimaging findings, differential diagnosis, and neurodevelopmental outcomes associated with AHT in pediatric patients. Methods: A systematic review was conducted in accordance with PRISMA 2020 guidelines. PubMed/MEDLINE, Scopus, and Web of Science were searched for studies published between January 2020 and March 2026. Eligible studies included observational studies, cohort studies, case-control studies, imaging-based investigations, clinically relevant review articles, and consensus statements evaluating clinical, radiological, or neurodevelopmental outcomes in infants and children with AHT. Because of heterogeneity in study design, outcome reporting, and availability of extractable data, findings were synthesized qualitatively. Results: A total of 428 records were identified. After removal of duplicates and screening, 25 studies were included in the qualitative synthesis. The most frequently reported clinical manifestations included seizures, irritability, altered mental status, apnea, vomiting, feeding difficulties, and developmental impairment. Subdural hematoma, retinal hemorrhage, cerebral edema, and hypoxic-ischemic injury were the predominant neuroimaging findings. Several studies emphasized the importance of differentiating AHT from benign enlargement of the subarachnoid spaces, coagulation disorders, accidental trauma, and other non-traumatic conditions. Long-term sequelae included developmental delay, epilepsy, cognitive impairment, motor dysfunction, visual impairment, and behavioral abnormalities. Conclusion: AHT remains a complex pediatric condition associated with significant neurological morbidity and diagnostic challenges. Neuroimaging plays a central role in evaluation, but multidisciplinary assessment and careful differential diagnosis are essential to avoid misclassification. Long-term neurodevelopmental follow-up is critical for affected children.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Abusive Head Trauma in Infancy and Early Childhood:
A Systematic Review of Clinical Manifestations, Neuroimaging Findings, Diagnosis, and Outcomes
AU - Vicente Manuel Martinez Cardenas
AU - Vivian Rosario Mena Miranda
Y1 - 2026/06/10
PY - 2026
N1 - https://doi.org/10.11648/j.frontiers.20260602.13
DO - 10.11648/j.frontiers.20260602.13
T2 - Frontiers
JF - Frontiers
JO - Frontiers
SP - 64
EP - 74
PB - Science Publishing Group
SN - 2994-7197
UR - https://doi.org/10.11648/j.frontiers.20260602.13
AB - Background: Abusive head trauma (AHT), historically referred to as shaken baby syndrome (SBS), is a major cause of severe traumatic brain injury in infants and young children and is associated with substantial morbidity, mortality, and diagnostic complexity. Objective: To systematically review current evidence regarding the clinical manifestations, neuroimaging findings, differential diagnosis, and neurodevelopmental outcomes associated with AHT in pediatric patients. Methods: A systematic review was conducted in accordance with PRISMA 2020 guidelines. PubMed/MEDLINE, Scopus, and Web of Science were searched for studies published between January 2020 and March 2026. Eligible studies included observational studies, cohort studies, case-control studies, imaging-based investigations, clinically relevant review articles, and consensus statements evaluating clinical, radiological, or neurodevelopmental outcomes in infants and children with AHT. Because of heterogeneity in study design, outcome reporting, and availability of extractable data, findings were synthesized qualitatively. Results: A total of 428 records were identified. After removal of duplicates and screening, 25 studies were included in the qualitative synthesis. The most frequently reported clinical manifestations included seizures, irritability, altered mental status, apnea, vomiting, feeding difficulties, and developmental impairment. Subdural hematoma, retinal hemorrhage, cerebral edema, and hypoxic-ischemic injury were the predominant neuroimaging findings. Several studies emphasized the importance of differentiating AHT from benign enlargement of the subarachnoid spaces, coagulation disorders, accidental trauma, and other non-traumatic conditions. Long-term sequelae included developmental delay, epilepsy, cognitive impairment, motor dysfunction, visual impairment, and behavioral abnormalities. Conclusion: AHT remains a complex pediatric condition associated with significant neurological morbidity and diagnostic challenges. Neuroimaging plays a central role in evaluation, but multidisciplinary assessment and careful differential diagnosis are essential to avoid misclassification. Long-term neurodevelopmental follow-up is critical for affected children.
VL - 6
IS - 2
ER -
Copy
|
Download