Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL)
Introduction: Acute kidney injury (AKI) in pregnancy encompasses all causes of acute renal impairment occurring between conception and delivery. HELLP Syndrome represents a severe form of pre-eclampsia that predisposes pregnant individuals to AKI. Objective: To examine the clinical and aetiological aspects of AKI in HELLP Syndrome among patients admitted to the obstetric intensive care unit of CHU-MEL in Cotonou from May 2018 to June 2023. Method: This was a cross-sectional, descriptive study conducted over five years at CHU-MEL, Cotonou, involving patients diagnosed with HELLP Syndrome. AKI was identified based on ACOG criteria, with staging determined according to the KDIGO classification. Results: A total of 51 patient records with HELLP Syndrome and associated AKI were included in the study. The prevalence of AKI among HELLP Syndrome patients was 64.56%. The majority were primigravidae and nulliparous women, with a mean age of 29 ± 5.92 years (range: 19-40 years). The most frequent gestational age at diagnosis was between 28 and 36 weeks. Diuresis was preserved in 94.12% of patients. Serum creatinine levels ranged from 11 to 74mg/L, and the mean glomerular filtration rate was 46.27 ± 21.55mL/min/1.73m² (range: 7.56-84.13). In this cohort, AKI Stage 1 developed in 65.31% of patients. The primary aetiology was HELLP Syndrome. The majority (82.35%) underwent caesarean section. Maternal mortality was 1.96% (one case), and foetal mortality stood at 31.37%, with complications including neonatal respiratory distress (40%), intrauterine growth restriction (26%), and intrauterine foetal death (19.61%). Conclusion: The prevalence of AKI among patients with HELLP Syndrome is notably high, with significant associated foetal morbidity.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
HELLP Syndrome is a complication of severe preeclampsia during pregnancy that can threaten the safety of both the mother and the foetus
[1]
Liu Q, Ling G, Zhang S, Zhai W, Chen Y. Effect of HELLP syndrome on acute kidney injury in pregnancy and pregnancy outcomes: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020; 20(1): 657.
[2]
Zelmat S, Bouabida D, Boucherit E, Mazour F. Le profil de l’insuffisance rénale dans le HELLP syndrome. Néphrologie Thérapeutique. 2021; 17(5): 377.
[1, 2]
. It is the leading cause of acute kidney injury (AKI) in pregnant women
[3]
Abraham K, Connolly G, Farrell J, Walshe J. The Hellp Syndrome, a Prospective Study. Renal Failure. 2001; 23(5): 705-713.
[3]
. Studies conducted by Erdemoglu and al. in 2010, Gedik and al. in 2017, and Huang and Chen in 2017 have suggested that HELLP Syndrome is a primary cause of pregnancy-related acute kidney injury
[4]
Gedik E, Yücel N, Sahin T, Koca E, Colak, Togal T. Hemolysis, elevated liver enzymes, and low platelet syndrome: Outcomes for patients admitted to intensive care at a tertiary referral hospital. Hypertension in Pregnancy. 2017; 36(1): 21-29.
[5]
Huang C, Chen S. Acute kidney injury during pregnancy and puerperium: a retrospective study in a single center. BMC Nephrology. 2017; 18(1): 146.
[4, 5]
. A study conducted in France in 2004 showed that the prevalence of AKI in cases of severe preeclampsia is estimated to be between 0.8% and 7.4% of HELLP Syndrome cases
[6]
Belenfant X, Pallot J-L, Reziz K, S. Saint Léger. Insuffisance rénale aiguë et grossesse. EMC - Néphrologie. 2004; 1(2): 44-54.
[6]
. Several factors make the diagnosis of AKI more challenging during pregnancy than in its absence. Due to physiological changes and an increased glomerular filtration rate (GFR), serum creatinine decreases during pregnancy, complicating the early and accurate diagnosis of AKI. In Benin, to the best of our knowledge, no studies had yet been conducted in this field. The aim of our study is to describe the clinical and aetiological aspects of AKI in patients with HELLP Syndrome admitted to the obstetric intensive care unit of CHU-MEL in Cotonou.
2. Patients and Methods
This was a retrospective, descriptive study carried out over a five-year period from 1 May 2018 to 30 June 2023. The study population comprised all patients admitted to the obstetric intensive care unit of CHU-MEL who were diagnosed with HELLP Syndrome and who developed acute kidney injury during the study period. Pregnant women or parturients who had been referred to another hospital, discharged against medical advice, absconded, or had not undergone renal blood tests were excluded. AKI was defined as a serum creatinine level >1.1mg/dL or a doubling of the serum creatinine concentration in the absence of renal disease. We classified AKI based on KDIGO criteria. The collected data were entered using the KoboCollect software and analysed using Stata Version 18.
3. Results
3.1. Frequency
During the study period, 2048 patients were admitted to the obstetric intensive care unit of CHU-MEL for severe preeclampsia, of which 85 cases were HELLP Syndrome, representing a frequency of 4.15%. Six cases were excluded from the study. Of the remaining 79 HELLP Syndrome cases, 51 patients experienced acute kidney injury, equating to an AKI frequency of 64.56% in patients with HELLP Syndrome.
3.2. Sociodemographic Characteristics
The average age was 29 ± 5.92 years, with a range of 19 to 40 years. Women aged 21-25 years were the most represented (27.45%). The patients had at least a primary level of education (60%), followed by secondary (18%), tertiary (18%), and 4% were unschooled. Street vendors (46%) and manual labourers (26%) were the most represented professions.
3.3. Mode and Reason for Admission
Most women were admitted by referral (88.24%). Among HELLP Syndrome patients with AKI, 56.86% had severe preeclampsia, and 21.57% had eclampsia.
3.4. Medical and Obstetric History
Among the 51 patients, only 4 (7.84%) had known hypertension. The mean gravidity was 2.59 ± 1.52. The mean parity was 1.33 ± 1.46. Primigravidae and nulliparous women were the most affected, accounting for 31.37% and 41.18%, respectively.
3.5. Clinical and Biological Aspects
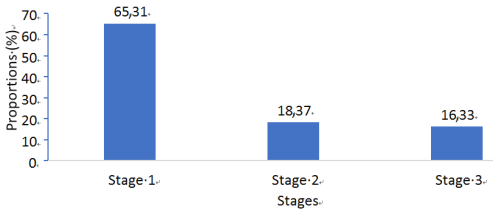
Functional signs included cough in 58.82% of cases (n=30), headaches in 56.86% (n=29), epigastric pain in 35.29% (n=18), seizures in 33.33% (n=17), and visual disturbances in 28% (n=14). General signs included asthenia (62.75%, n=32), conjunctival pallor (17.65%, n=9), and altered consciousness (4 patients). Lower limb oedema was found in 41.18% (n=21). Severe hypertension was present, with a mean systolic blood pressure of 183.25mmHg ± 28.69 (range: 140-290) and a mean diastolic pressure of 117.90 ± 28.69 (range: 82-180). Foetal heart sounds were absent in 23.53% of cases (n=12). Crackles were noted in 3 patients, and active haemorrhage in 2 patients. Diuresis was preserved in 48 patients (94.12%) and oliguric in 3 cases. Regarding proteinuria on dipstick analysis, 22% (n=11) had proteinuria of 2+, 56% (n=28) had proteinuria of 3+, and 20% (n=10) had proteinuria greater than 3+. Among the respondents, 47.06% had a platelet count between 50 and 100. Haemoglobin levels ranged from 4.2 to 13.8, with a mean of 8.46 ± 2.26; 46% of women had mild anaemia. A total of 5 women underwent fasting blood glucose testing, all of which were normal. Aspartate aminotransferase (AST) levels ranged from 10 to 3905, with a median of 127 (IQR: 70-360). Alanine aminotransferase (ALT) levels ranged from 11 to 1714, with a median of 111 (IQR: 37-270). Electrolytes were assessed in 78% of women. Sodium levels were normal in 61.54%, calcium levels normal in 60%, and potassium levels normal in 74.36%. Serum creatinine ranged from 11 to 74mg/L, with a median of 14 (IQR: 12-24). Blood urea levels ranged from 0.45 to 1.88g/L, with a mean of 0.50 ± 0.35. The mean glomerular filtration rate was 46.27 ± 21.55, with extremes of 7.56 and 84.13.
Figure 1. Distribution According to the AKI Classification.
The main aetiological factors were HELLP Syndrome (100%), severe preeclampsia (78%), eclampsia (36%), and immediate postpartum haemorrhage (4%).
4. Discussion
The frequency of acute kidney injury (AKI) among patients with HELLP Syndrome at CHU-MEL was 64.56%. This result is higher than that reported by Ye and al.
[7]
Ye W, Shu H, Yu Y, Li H, Chen L, Liu J. Acute kidney injury in patients with HELLP syndrome. International Urology and Nephrology. 2019; 51(7): 1199-1206.
[7]
in China, which was 48.1%. A lower rate of 15% was reported by Gul and al.
[8]
Gul A, Aslan H, Cebeci A, Polat I, Ulusoy S, Ceylan Y. Maternal and Fetal Outcomes in HELLP Syndrome Complicated with Acute Renal Failure. Renal Failure. 2004; 26(5): 557-562.
[8]
in a study conducted in Turkey. In Algeria, a study by Zelmat and al.
[4]
Gedik E, Yücel N, Sahin T, Koca E, Colak, Togal T. Hemolysis, elevated liver enzymes, and low platelet syndrome: Outcomes for patients admitted to intensive care at a tertiary referral hospital. Hypertension in Pregnancy. 2017; 36(1): 21-29.
[4]
found a prevalence of 33%. Gedik and al. reported a rate of 25%. These variations suggest that the frequency of AKI in patients with HELLP Syndrome differs across study populations.
In our study, the mean age was 29 ± 5.92 years, with a range of 19 to 40 years. Women aged 21-25 years were the most represented (27.45%). This result is similar to findings from Ye and al.
[7]
Ye W, Shu H, Yu Y, Li H, Chen L, Liu J. Acute kidney injury in patients with HELLP syndrome. International Urology and Nephrology. 2019; 51(7): 1199-1206.
[7]
and Gul and al.
[8]
Gul A, Aslan H, Cebeci A, Polat I, Ulusoy S, Ceylan Y. Maternal and Fetal Outcomes in HELLP Syndrome Complicated with Acute Renal Failure. Renal Failure. 2004; 26(5): 557-562.
[8]
, who reported mean ages of 31.10 ± 6.39 and 27.9 ± 4.8 years, respectively, among patients with HELLP Syndrome and AKI. The most represented occupations were street vendors (46%) and manual labourers (26%). Sanogo S
[10]
Sanogo S. Epidémiologie et prise en charge du HELLP syndrome dans le Service de Gynécologie-Obstétrique du CHU Gabriel Touré. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2018. Accessed 21 January 2024.
[10]
, in a study conducted in Mali on women with HELLP Syndrome, found that housewives were three times more represented than other women. The predominance of housewives in certain studies may be attributed to lower literacy rates and socioeconomic conditions.
The mean gravidity was 2.59 ± 1.52, and the mean parity was 1.33 ± 1.46. Gul and al.
[8]
Gul A, Aslan H, Cebeci A, Polat I, Ulusoy S, Ceylan Y. Maternal and Fetal Outcomes in HELLP Syndrome Complicated with Acute Renal Failure. Renal Failure. 2004; 26(5): 557-562.
[8]
, Sullivan and al
[11]
Sullivan CA, Magann EF, Perry KG, Roberts WE, Blake PG, Martin JN. The recurrence risk of the syndrome of hemolysis, elevated liver enzymes, and low platelets (HELLP) in subsequent gestations. American Journal of Obstetrics Gynecology. 1994; 171(4): 940-943.
[11]
, Martin and al.
[12]
Martin JN, Blake PG, Perry KG, McCaul JF, Hess LW, Martin RW. The natural history of HELLP syndrome: Patterns of disease progression and regression. American Journal of Obstetrics and Gynecology. 1991; 164(6): 1500-1513.
[12]
, reported a parity of 1.0 ± 0.83, which may be explained by a higher birth rate in our study population. The most affected groups were primigravidae and nulliparous women, accounting for 31.37% and 41.18% of cases, respectively. This differs in parity distribution from findings by Hafidy and al.
[13]
Hafidy KE, Khair M, Hermas S, Bennani O, Laghzaoui M, Bouhya S. HELLP SYNDROME. A PROPOS DE 28 CAS. Journal Marocain des Sciences Médicales. 2009; 16(3): 23-26.
[13]
, who reported that primigravidae and primiparous women accounted for 39.28% of HELLP Syndrome cases. Similarly, Coulibaly S
[9]
Coulibaly S. Aspect épidémiologique, clinique et pronostique du Hellp syndrome au service de réanimation polyvalente du CHU-GT. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2021. Accessed 21 January 2024.
[9]
, Adnani IE and al.
[14]
Adnani IE, Agzid N, Mahmal S, Hafiane Y, Mtioui N, Elkhayat S et al. Prévalence de l’insuffisance rénale aiguë dans le HELLP syndrome. Néphrologie et Thérapeutique
, found that primigravidae and primiparous women constituted 50.9% and 49.1% of patients with HELLP Syndrome, suggesting that primigravidae are more exposed to HELLP Syndrome.
In our study, the majority of patients (88.24%) were referred from another healthcare facility, with the most common reasons for admission being severe pre-eclampsia (56.86%) and eclampsia (21.57%). These findings align with those of Guimatsia N
[16]
Guimatsia N, Léolein M. Aspect épidémiologique, clinique, thérapeutique et pronostic du HELLP syndrome au CHU du Point G. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2023. Accessed 21 January 2024.
[16]
, who reported an eclampsia rate of 29% and severe pre-eclampsia rate of 16.7%. Coulibaly S
[9]
Coulibaly S. Aspect épidémiologique, clinique et pronostique du Hellp syndrome au service de réanimation polyvalente du CHU-GT. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2021. Accessed 21 January 2024.
[9]
found an eclampsia rate of 45% in his study. These results confirm that severe pre-eclampsia and eclampsia are the most common admission diagnoses in patients with HELLP Syndrome.
Regarding functional signs, cough was present in 58.82% of cases (n=30), headaches in 56.86% (n=29), epigastric pain in 35.29% (n=18), seizures in 33.33% (n=17), and visual disturbances in 28% (n=14). Headache predominance was also observed in Coulibaly S
[9]
Coulibaly S. Aspect épidémiologique, clinique et pronostique du Hellp syndrome au service de réanimation polyvalente du CHU-GT. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2021. Accessed 21 January 2024.
[9]
, with an incidence of 65.5%, followed by epigastric pain (23.6%).
General symptoms included asthenia in 62.75% (n=32), conjunctival pallor in 17.65% (n=9), altered consciousness in 4 patients, and lower limb oedema in 41.18% (n=21). These findings were similar to those of Coulibaly S
[9]
Coulibaly S. Aspect épidémiologique, clinique et pronostique du Hellp syndrome au service de réanimation polyvalente du CHU-GT. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2021. Accessed 21 January 2024.
[9]
, who reported oedema in 36.4% and conjunctival pallor in 12.7% of cases. Bakayoko M
[15]
Bakayoko MN. Le HELLP syndrome en réanimation Polyvalente et soins intensifs: évaluation de la prise en charge au CHU du Point G. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2019. Accessed 22 January 2024.
[15]
found oedema in 40% and conjunctival pallor in 43.6%.
Regarding dipstick proteinuria, 22% (n=11) had proteinuria of 2+, 56% (n=28) had proteinuria of 3+, and 20% (n=10) had proteinuria exceeding 3+. The mean systolic blood pressure was 183.25 ± 28.69mmHg (range: 140-290), and the mean diastolic blood pressure was 117.90 ± 28.69mmHg (range: 82-180), comparable to results found by Sanogo S
[10]
Sanogo S. Epidémiologie et prise en charge du HELLP syndrome dans le Service de Gynécologie-Obstétrique du CHU Gabriel Touré. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2018. Accessed 21 January 2024.
[10]
.
Diuresis was preserved in 94.12% (n=48) of patients, while 5.88% (n=3) were oliguric. By contrast, Koïta M
[18]
Koita M. Insuffisance rénale aigue obstétricale : profil épidémiologique, étiologique et évolutif dans le service de médecine et d’unité d’hémodialyse de l’hôpital de SIKASSO. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 22 Décembre 2023.
[18]
, in an evaluation of diuresis among patients with obstetric AKI, reported 39.3% oliguria, 28.6% anuria, and 32.1% preserved diuresis. Mahfoud O
[19]
Mahfoudh O. Insuffisance rénale aiguë au cours de la grossesse et du post-partum. Néphrologie
found oliguria in 75% and anuria in 8.33% of cases. These differences may explain the rarity of complications related to AKI in our study and the absence of dialysis requirements.
Haemoglobin levels ranged from 4.2 to 13.8g/dL, with a mean of 8.46 ± 2.26g/dL, and 46% of women had mild anaemia. These results are similar to those of Bèye M and al.
[20]
Bèye MD, Diouf E, Bah MD, Ndoye-Diop M, Kane O, Sall-ka B. Prise en charge du HELLP syndrome en réanimation à Dakar. Annales Françaises d'Anesthésie et de Réanimation. 2006; 25(3): 291-295.
[20]
, who reported haemoglobin levels ranging from 3 to 13g/dL. Elevated ALT levels were observed in 76.47% of patients. Diouf A and al.
[17]
Diouf A A, Mbodji A, Diallo M, Guèye M, Aidara NK, Coulbary AS et al. Le syndrome HELLP : profil clinique et prise en charge à Dakar. Revue Africaine de Medecine Interne. 2017; 4: 13-18.
[17]
found elevated transaminase levels in all patients in their study.
In our study, creatinine levels ranged from 11 to 74mg/L, with 72.55% of patients having creatinine levels between 11 and 20mg/L. However, Ibrahim F
[21]
Fomba I. Insuffisance rénale aigue d’origine obstétricale : aspects épidémiologique, étiologique et évolutif dans le service de néphrologie et hémodialyse du CHU DU POINT G. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2023. Accessed 24 December 2023).
[21]
found a mean creatinine level of 114mg/L (range: 23-226), with 53.1% of patients having creatinine levels between 57 and 113mg/L. Koïta M
[18]
Koita M. Insuffisance rénale aigue obstétricale : profil épidémiologique, étiologique et évolutif dans le service de médecine et d’unité d’hémodialyse de l’hôpital de SIKASSO. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 22 Décembre 2023.
[18]
reported a mean creatinine level of 106mg/L (range: 30-245), with 60.7% of patients exceeding 90mg/L. These differences may explain the lower severity of AKI in our study.
The main etiology of ARA found was HELLP Syndrome (100.00%), retro-placental hematoma (9.80%). Miguil and al.
[22]
Miguil M, Salmi S, Moussaid I, Benyounes M. Insuffisance rénale aiguë hémodialysée en obstétrique. Néphrologie et Thérapeutique. 2011; 7: 179-181.
[22]
in his study found as main etiologies preeclampsia-eclampsia or 67.2%, followed by hemorrhage or 25.9%. Selçuk and al
[23]
Selcuk NY, Tonbul HZ, San A, Odabas AR. Changes in frequency and etiology of acute renal failure in pregnancy (1980 - 1997). Renal Failure. 1998; 20(3): 513-517.
[23]
found as main etiologies HELLP Syndrome or 35.9%, postpartum hemorrhage or 17.9%, preeclampsia-eclampsia or 15.4%. This difference in the distribution in the results could be explained by the fact that we had carried out our study on a population of patients with HELLP Syndrome.
5. Conclusion
The prevalence of AKI among patients with HELLP syndrome is remarkably high. Associated complications, including neonatal respiratory distress, intrauterine growth restriction, foetal death, and maternal mortality, highlight the urgent need for improved management and preventive strategies for hypertensive disorders in pregnancy (severe pre-eclampsia, eclampsia, and HELLP Syndrome). Early intervention is essential to reduce maternal and neonatal morbidity and mortality.
Abbreviations
AKI
Acute Kidney Injury
KDIGO
Kidney Disease Improving Global Outcomes
ACOG
American College of Obstetricians and Gynecologists
HKM
Hubert Koutoukou Maga
HELLP
Hemolysis Elevated Liver Enzymes and Low Platelets
Acknowledgments
The authors wish to thank NJITAM GASSAM Stéphane Brice for his contributions to the translation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Liu Q, Ling G, Zhang S, Zhai W, Chen Y. Effect of HELLP syndrome on acute kidney injury in pregnancy and pregnancy outcomes: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020; 20(1): 657.
[2]
Zelmat S, Bouabida D, Boucherit E, Mazour F. Le profil de l’insuffisance rénale dans le HELLP syndrome. Néphrologie Thérapeutique. 2021; 17(5): 377.
[3]
Abraham K, Connolly G, Farrell J, Walshe J. The Hellp Syndrome, a Prospective Study. Renal Failure. 2001; 23(5): 705-713.
[4]
Gedik E, Yücel N, Sahin T, Koca E, Colak, Togal T. Hemolysis, elevated liver enzymes, and low platelet syndrome: Outcomes for patients admitted to intensive care at a tertiary referral hospital. Hypertension in Pregnancy. 2017; 36(1): 21-29.
[5]
Huang C, Chen S. Acute kidney injury during pregnancy and puerperium: a retrospective study in a single center. BMC Nephrology. 2017; 18(1): 146.
[6]
Belenfant X, Pallot J-L, Reziz K, S. Saint Léger. Insuffisance rénale aiguë et grossesse. EMC - Néphrologie. 2004; 1(2): 44-54.
[7]
Ye W, Shu H, Yu Y, Li H, Chen L, Liu J. Acute kidney injury in patients with HELLP syndrome. International Urology and Nephrology. 2019; 51(7): 1199-1206.
[8]
Gul A, Aslan H, Cebeci A, Polat I, Ulusoy S, Ceylan Y. Maternal and Fetal Outcomes in HELLP Syndrome Complicated with Acute Renal Failure. Renal Failure. 2004; 26(5): 557-562.
[9]
Coulibaly S. Aspect épidémiologique, clinique et pronostique du Hellp syndrome au service de réanimation polyvalente du CHU-GT. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2021. Accessed 21 January 2024.
[10]
Sanogo S. Epidémiologie et prise en charge du HELLP syndrome dans le Service de Gynécologie-Obstétrique du CHU Gabriel Touré. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2018. Accessed 21 January 2024.
[11]
Sullivan CA, Magann EF, Perry KG, Roberts WE, Blake PG, Martin JN. The recurrence risk of the syndrome of hemolysis, elevated liver enzymes, and low platelets (HELLP) in subsequent gestations. American Journal of Obstetrics Gynecology. 1994; 171(4): 940-943.
[12]
Martin JN, Blake PG, Perry KG, McCaul JF, Hess LW, Martin RW. The natural history of HELLP syndrome: Patterns of disease progression and regression. American Journal of Obstetrics and Gynecology. 1991; 164(6): 1500-1513.
[13]
Hafidy KE, Khair M, Hermas S, Bennani O, Laghzaoui M, Bouhya S. HELLP SYNDROME. A PROPOS DE 28 CAS. Journal Marocain des Sciences Médicales. 2009; 16(3): 23-26.
[14]
Adnani IE, Agzid N, Mahmal S, Hafiane Y, Mtioui N, Elkhayat S et al. Prévalence de l’insuffisance rénale aiguë dans le HELLP syndrome. Néphrologie et Thérapeutique
Bakayoko MN. Le HELLP syndrome en réanimation Polyvalente et soins intensifs: évaluation de la prise en charge au CHU du Point G. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2019. Accessed 22 January 2024.
[16]
Guimatsia N, Léolein M. Aspect épidémiologique, clinique, thérapeutique et pronostic du HELLP syndrome au CHU du Point G. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2023. Accessed 21 January 2024.
[17]
Diouf A A, Mbodji A, Diallo M, Guèye M, Aidara NK, Coulbary AS et al. Le syndrome HELLP : profil clinique et prise en charge à Dakar. Revue Africaine de Medecine Interne. 2017; 4: 13-18.
[18]
Koita M. Insuffisance rénale aigue obstétricale : profil épidémiologique, étiologique et évolutif dans le service de médecine et d’unité d’hémodialyse de l’hôpital de SIKASSO. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 22 Décembre 2023.
[19]
Mahfoudh O. Insuffisance rénale aiguë au cours de la grossesse et du post-partum. Néphrologie
Bèye MD, Diouf E, Bah MD, Ndoye-Diop M, Kane O, Sall-ka B. Prise en charge du HELLP syndrome en réanimation à Dakar. Annales Françaises d'Anesthésie et de Réanimation. 2006; 25(3): 291-295.
[21]
Fomba I. Insuffisance rénale aigue d’origine obstétricale : aspects épidémiologique, étiologique et évolutif dans le service de néphrologie et hémodialyse du CHU DU POINT G. BAMAKO: Faculté de Médecine et d’Odontostomatologie; 2023. Accessed 24 December 2023).
[22]
Miguil M, Salmi S, Moussaid I, Benyounes M. Insuffisance rénale aiguë hémodialysée en obstétrique. Néphrologie et Thérapeutique. 2011; 7: 179-181.
[23]
Selcuk NY, Tonbul HZ, San A, Odabas AR. Changes in frequency and etiology of acute renal failure in pregnancy (1980 - 1997). Renal Failure. 1998; 20(3): 513-517.
Giovanna, Z., Joseph, A., Armel, A., Jacques, V., Eugene, Z. (2025). Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL). International Journal of Anesthesia and Clinical Medicine, 13(1), 58-62. https://doi.org/10.11648/j.ijacm.20251301.18
Giovanna, Z.; Joseph, A.; Armel, A.; Jacques, V.; Eugene, Z. Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL). Int. J. Anesth. Clin. Med.2025, 13(1), 58-62. doi: 10.11648/j.ijacm.20251301.18
Giovanna Z, Joseph A, Armel A, Jacques V, Eugene Z. Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL). Int J Anesth Clin Med. 2025;13(1):58-62. doi: 10.11648/j.ijacm.20251301.18
@article{10.11648/j.ijacm.20251301.18,
author = {Zossoungbo Giovanna and Akodjenou Joseph and Adjofoguè Armel and Vigan Jacques and Zoumènou Eugene},
title = {Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL)},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {1},
pages = {58-62},
doi = {10.11648/j.ijacm.20251301.18},
url = {https://doi.org/10.11648/j.ijacm.20251301.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251301.18},
abstract = {Introduction: Acute kidney injury (AKI) in pregnancy encompasses all causes of acute renal impairment occurring between conception and delivery. HELLP Syndrome represents a severe form of pre-eclampsia that predisposes pregnant individuals to AKI. Objective: To examine the clinical and aetiological aspects of AKI in HELLP Syndrome among patients admitted to the obstetric intensive care unit of CHU-MEL in Cotonou from May 2018 to June 2023. Method: This was a cross-sectional, descriptive study conducted over five years at CHU-MEL, Cotonou, involving patients diagnosed with HELLP Syndrome. AKI was identified based on ACOG criteria, with staging determined according to the KDIGO classification. Results: A total of 51 patient records with HELLP Syndrome and associated AKI were included in the study. The prevalence of AKI among HELLP Syndrome patients was 64.56%. The majority were primigravidae and nulliparous women, with a mean age of 29 ± 5.92 years (range: 19-40 years). The most frequent gestational age at diagnosis was between 28 and 36 weeks. Diuresis was preserved in 94.12% of patients. Serum creatinine levels ranged from 11 to 74mg/L, and the mean glomerular filtration rate was 46.27 ± 21.55mL/min/1.73m² (range: 7.56-84.13). In this cohort, AKI Stage 1 developed in 65.31% of patients. The primary aetiology was HELLP Syndrome. The majority (82.35%) underwent caesarean section. Maternal mortality was 1.96% (one case), and foetal mortality stood at 31.37%, with complications including neonatal respiratory distress (40%), intrauterine growth restriction (26%), and intrauterine foetal death (19.61%). Conclusion: The prevalence of AKI among patients with HELLP Syndrome is notably high, with significant associated foetal morbidity.},
year = {2025}
}
TY - JOUR
T1 - Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL)
AU - Zossoungbo Giovanna
AU - Akodjenou Joseph
AU - Adjofoguè Armel
AU - Vigan Jacques
AU - Zoumènou Eugene
Y1 - 2025/06/25
PY - 2025
N1 - https://doi.org/10.11648/j.ijacm.20251301.18
DO - 10.11648/j.ijacm.20251301.18
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 58
EP - 62
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20251301.18
AB - Introduction: Acute kidney injury (AKI) in pregnancy encompasses all causes of acute renal impairment occurring between conception and delivery. HELLP Syndrome represents a severe form of pre-eclampsia that predisposes pregnant individuals to AKI. Objective: To examine the clinical and aetiological aspects of AKI in HELLP Syndrome among patients admitted to the obstetric intensive care unit of CHU-MEL in Cotonou from May 2018 to June 2023. Method: This was a cross-sectional, descriptive study conducted over five years at CHU-MEL, Cotonou, involving patients diagnosed with HELLP Syndrome. AKI was identified based on ACOG criteria, with staging determined according to the KDIGO classification. Results: A total of 51 patient records with HELLP Syndrome and associated AKI were included in the study. The prevalence of AKI among HELLP Syndrome patients was 64.56%. The majority were primigravidae and nulliparous women, with a mean age of 29 ± 5.92 years (range: 19-40 years). The most frequent gestational age at diagnosis was between 28 and 36 weeks. Diuresis was preserved in 94.12% of patients. Serum creatinine levels ranged from 11 to 74mg/L, and the mean glomerular filtration rate was 46.27 ± 21.55mL/min/1.73m² (range: 7.56-84.13). In this cohort, AKI Stage 1 developed in 65.31% of patients. The primary aetiology was HELLP Syndrome. The majority (82.35%) underwent caesarean section. Maternal mortality was 1.96% (one case), and foetal mortality stood at 31.37%, with complications including neonatal respiratory distress (40%), intrauterine growth restriction (26%), and intrauterine foetal death (19.61%). Conclusion: The prevalence of AKI among patients with HELLP Syndrome is notably high, with significant associated foetal morbidity.
VL - 13
IS - 1
ER -
Giovanna, Z., Joseph, A., Armel, A., Jacques, V., Eugene, Z. (2025). Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL). International Journal of Anesthesia and Clinical Medicine, 13(1), 58-62. https://doi.org/10.11648/j.ijacm.20251301.18
Giovanna, Z.; Joseph, A.; Armel, A.; Jacques, V.; Eugene, Z. Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL). Int. J. Anesth. Clin. Med.2025, 13(1), 58-62. doi: 10.11648/j.ijacm.20251301.18
Giovanna Z, Joseph A, Armel A, Jacques V, Eugene Z. Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL). Int J Anesth Clin Med. 2025;13(1):58-62. doi: 10.11648/j.ijacm.20251301.18
@article{10.11648/j.ijacm.20251301.18,
author = {Zossoungbo Giovanna and Akodjenou Joseph and Adjofoguè Armel and Vigan Jacques and Zoumènou Eugene},
title = {Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL)},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {1},
pages = {58-62},
doi = {10.11648/j.ijacm.20251301.18},
url = {https://doi.org/10.11648/j.ijacm.20251301.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251301.18},
abstract = {Introduction: Acute kidney injury (AKI) in pregnancy encompasses all causes of acute renal impairment occurring between conception and delivery. HELLP Syndrome represents a severe form of pre-eclampsia that predisposes pregnant individuals to AKI. Objective: To examine the clinical and aetiological aspects of AKI in HELLP Syndrome among patients admitted to the obstetric intensive care unit of CHU-MEL in Cotonou from May 2018 to June 2023. Method: This was a cross-sectional, descriptive study conducted over five years at CHU-MEL, Cotonou, involving patients diagnosed with HELLP Syndrome. AKI was identified based on ACOG criteria, with staging determined according to the KDIGO classification. Results: A total of 51 patient records with HELLP Syndrome and associated AKI were included in the study. The prevalence of AKI among HELLP Syndrome patients was 64.56%. The majority were primigravidae and nulliparous women, with a mean age of 29 ± 5.92 years (range: 19-40 years). The most frequent gestational age at diagnosis was between 28 and 36 weeks. Diuresis was preserved in 94.12% of patients. Serum creatinine levels ranged from 11 to 74mg/L, and the mean glomerular filtration rate was 46.27 ± 21.55mL/min/1.73m² (range: 7.56-84.13). In this cohort, AKI Stage 1 developed in 65.31% of patients. The primary aetiology was HELLP Syndrome. The majority (82.35%) underwent caesarean section. Maternal mortality was 1.96% (one case), and foetal mortality stood at 31.37%, with complications including neonatal respiratory distress (40%), intrauterine growth restriction (26%), and intrauterine foetal death (19.61%). Conclusion: The prevalence of AKI among patients with HELLP Syndrome is notably high, with significant associated foetal morbidity.},
year = {2025}
}
TY - JOUR
T1 - Clinical and Aetiological Aspects of Acute Kidney Injury in Patients with Hellp Syndrome in the Obstetric Intensive Care Unit of the University Hospital Centre for Mother and Child (CHU-MEL)
AU - Zossoungbo Giovanna
AU - Akodjenou Joseph
AU - Adjofoguè Armel
AU - Vigan Jacques
AU - Zoumènou Eugene
Y1 - 2025/06/25
PY - 2025
N1 - https://doi.org/10.11648/j.ijacm.20251301.18
DO - 10.11648/j.ijacm.20251301.18
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 58
EP - 62
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20251301.18
AB - Introduction: Acute kidney injury (AKI) in pregnancy encompasses all causes of acute renal impairment occurring between conception and delivery. HELLP Syndrome represents a severe form of pre-eclampsia that predisposes pregnant individuals to AKI. Objective: To examine the clinical and aetiological aspects of AKI in HELLP Syndrome among patients admitted to the obstetric intensive care unit of CHU-MEL in Cotonou from May 2018 to June 2023. Method: This was a cross-sectional, descriptive study conducted over five years at CHU-MEL, Cotonou, involving patients diagnosed with HELLP Syndrome. AKI was identified based on ACOG criteria, with staging determined according to the KDIGO classification. Results: A total of 51 patient records with HELLP Syndrome and associated AKI were included in the study. The prevalence of AKI among HELLP Syndrome patients was 64.56%. The majority were primigravidae and nulliparous women, with a mean age of 29 ± 5.92 years (range: 19-40 years). The most frequent gestational age at diagnosis was between 28 and 36 weeks. Diuresis was preserved in 94.12% of patients. Serum creatinine levels ranged from 11 to 74mg/L, and the mean glomerular filtration rate was 46.27 ± 21.55mL/min/1.73m² (range: 7.56-84.13). In this cohort, AKI Stage 1 developed in 65.31% of patients. The primary aetiology was HELLP Syndrome. The majority (82.35%) underwent caesarean section. Maternal mortality was 1.96% (one case), and foetal mortality stood at 31.37%, with complications including neonatal respiratory distress (40%), intrauterine growth restriction (26%), and intrauterine foetal death (19.61%). Conclusion: The prevalence of AKI among patients with HELLP Syndrome is notably high, with significant associated foetal morbidity.
VL - 13
IS - 1
ER -