Anesthesia plays a critical role in modern surgical care by ensuring patient comfort, safety, and physiologic stability. However, the effects of anesthetic agents extend beyond sedation and analgesia and include important, yet often underrecognized, influences on perioperative glucose metabolism. This consideration is particularly relevant in patients with diabetes mellitus, a growing surgical population in whom perioperative hyperglycemia is strongly associated with increased risks of infection, delayed wound healing, cardiovascular complications, and prolonged hospital stay. This narrative review synthesized current clinical and mechanistic evidence regarding how commonly used anesthetic agents and techniques influence perioperative glucose homeostasis. Volatile anesthetics have been shown to impair pancreatic β-cell insulin secretion and promote peripheral insulin resistance through the effect on cellular ion channels, mitochondrial function, and stress hormone pathways, frequently resulting in intraoperative hyperglycemia. In contrast, propofol-based total intravenous anesthesia (TIVA) appears to exert comparatively milder effects on insulin dynamics in many clinical contexts. Adjunctive agents such as dexmedetomidine and clonidine may further stabilize glucose levels through sympatholytic and stress-attenuating mechanisms. Additionally, regional and neuraxial anesthesia consistently demonstrate an ability to blunt the neuroendocrine stress response to surgery, thereby promoting improved glycemic stability. By integrating physiologic mechanisms with clinical findings, this review highlights how anesthetic choice can meaningfully influence perioperative glucose trends. Understanding these interactions is essential for optimizing anesthetic planning, intraoperative monitoring, and glycemic management strategies in diabetic surgical patients.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Anesthetic Effects on Glucose Metabolism, Perioperative Glucose Homeostasis, Surgical Stress and Hyperglycemia,
Glucose Regulation During Anesthesia, Anesthesia and Glycemic Control, Anesthesia Impact on Blood Glucose
1. Background
Diabetes Mellitus is a prevalent comorbidity among surgical patients worldwide and represents a major perioperative management challenge. The national prevalence of diabetes in the United States has risen steadily over the past decades. A 2021 review showed a crude estimate that 11.6% of the United States population had diabetes and a substantial percentage of patients who undergo elective and emergency surgeries present with diagnosed diabetes or impaired glucose tolerance
[1]
Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2024. Atlanta, GA: US Department of Health and Human Services; 2024.
[1]
. Perioperative hyperglycemia in diabetic patients increases mortality and morbidity and has been connected to increased risk of surgical site infection, delayed wound healing, longer length of stay, and cardiovascular complications. These factors make glucose management a cornerstone of perioperative care
[2]
Akhtar S, Barash PG, Inzucchi SE. Scientific principles and clinical implications of perioperative glucose regulation and control. Anesth Analg. 2010 Feb 1; 110(2): 478-97.
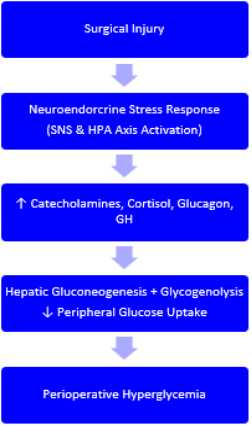
The metabolic disturbances that underlie perioperative hyperglycemia are multifactorial. Surgery injury elicits a complex neuroendocrine response: nociceptive afferent signals and tissue injury activate the sympathetic nervous system and hypothalamic-pituitary-adrenal (HPA) axis, producing elevated circulating catecholamines, cortisol, glucagon, and growth hormone. These hormones increase hepatic gluconeogenesis and glycogenolysis, reduce peripheral glucose uptake, and promote insulin resistance in skeletal muscle and adipose tissue
[3]
Shuford R, Miller-Ocuin JL. Hyperglycemia in the Perioperative Period. Clin Colon Rectal Surg. 2023 Jan 25; 36(3): 198-200.
Physiol Rep Editorial Board. The neuro-endocrine stress response compensates for loss of insulin-mediated glucose homeostasis. Physiol Rep. 2023; 11: e15603.
a physiologic process extensively described in mechanistic analyses of the perioperative neuroendocrine stress response. In patients with diabetes, baseline deficits in insulin secretion and/or action reduce metabolic reverse and widen the amplitude and duration of hyperglycemic excursions during and after surgery.
Anesthetic agents influence glucose metabolism through neuroendocrine and cellular mechanisms. Management of these anesthetic agents exert a modulatory effect on this stress response and on glucose homeostasis through several mechanisms. First, the anesthetic agents differ in their effects on neuroendocrine activation: techniques or drugs that blunt nociceptive transmission and sympathetic outflow (e.g. neuraxial blockade, regional anesthesia) typically attenuate the rise in counter-regulatory hormones and thereby mitigate intraoperative hyperglycemia
[4]
van den Brom CE, Bulte CS, Loer SA, Bouwman RA, Boer C. Diabetes, perioperative ischaemia and volatile anaesthetics: consequences of derangements in myocardial substrate metabolism. Cardiovasc Diabetol. 2013 Mar 4; 12: 42.
. Conversely, agents that increase sympathetic tone or catecholamine release (e.g. ketamine and high-dose volatile agents in some contexts) can exacerbate hyperglycemia
[6]
Xiong X, He Y, Zhou C, Zheng Q, Chen C, Liang P. Impact of total intravenous anesthesia and total inhalation anesthesia as the anesthesia maintenance approaches on blood glucose level and postoperative complications in patients with type 2 diabetes mellitus: a double-blind, randomized controlled trial. BMC Anesthesiol. 2024 Jan 22; 24(1): 36.
. Second, anesthetic drugs may have direct actions on pancreatic beta cell function, insulin signaling pathways, or hepatic and peripheral glucose metabolism. Experimental and clinical data indicate that volatile anesthetics (isoflurane, sevoflurane, desflurane) can impair insulin secretion and promote peripheral insulin resistance via effects on ion channels, mitochondrial function, and cellular signaling cascades
[9]
Kitamura T, Saito M, Yoshida K. Effects of volatile anesthetics on insulin secretion and glucose metabolism. Anesth Analg. 2020; 130(4): 1012–1020.
[11]
Yasuda Y, Watanabe M, Kobayashi K, et al. Propofol induces insulin resistance through inhibition of insulin receptor signaling. Biochem Biophys Res Commun. 2013; 439(1): 50–54.
. Propofol, the backbone of total intravenous anesthesia (TIVA), has been variably reported to produce less insulin resistance than volatiles in some clinical contexts, though findings are not uniform and may depend on dose, infusion duration, and the clinical circumstance
[5]
Tanaka K, Nishikawa T, Morimoto Y. Comparison of total intravenous and inhalational anesthesia on perioperative glucose homeostasis in diabetic patients: A randomized controlled trial. Br J Anaesth. 2021; 126(6) 135–1142.
[16]
Gan Y, Li Q, Zhang W, et al. The safety of perioperative dexamethasone with antiemetic dosage in patients with diabetes: a systematic review and meta-analysis. Perioper Med (Lond). 2023; 12: 14.
[5, 16]
.
Adjunct medications commonly employed in modern anesthetic practice, such as dexmedetomidine, clonidine, and multimodal analgesics, have received increasing attention for their potential to stabilize perioperative glucose by reducing catecholamine release and inflammatory mediators
[14]
Zhou W, Wang J, Yang D, et al. Effects of dexmedetomidine on glucose-related hormones and lactate in non-diabetic patients under general anesthesia. Minerva Anestesiol. 2022; 88(1): 8–15.
. Dexmedetomidine has been shown in several clinical studies to attenuate stress hormone surges and to reduce intraoperative and early postoperative hyperglycemia in surgical cohorts, including some diabetic subgroups
[20]
Li M, Zhou X, Huang L, et al. Epidural anesthesia improves perioperative insulin sensitivity and reduces postoperative hyperglycemia in diabetic patients. Anesth Analg. 2020; 131(3): 892–899.
. Conversely, widely used agents such as perioperative corticosteroids and certain vasopressors may induce or worsen hyperglycemia and necessitate anticipatory insulin adjustments.
Beyond individual agents, anesthetic techniques, especially the use of regional or neuraxial anesthesia as an adjunct or alternative to general anesthesia, consistently demonstrates a capacity to blunt the neuroendocrine response to surgical stimulation, reduce perioperative insulin resistance, and improve glycemic stability
[24]
Schricker T, Lattermann R. Perioperative catabolism. Can J Anaesth. 2015 Feb; 62(2): 182-93.
, as described in comprehensive reviews of perioperative catabolic and metabolic stress pathways. These physiologic effects are especially relevant in diabetic patients, where reducing hormonal surges may translate to fewer hyperglycemia-related complications.
Despite the physiologic plausibility and accumulating clinical data, existing literature is heterogenous. Studies vary by patient population (type 1 vs type 2 vs mixed diabetes), type and duration of surgery, anesthetic regimens, perioperative glucose targets, and monitoring frequency, limiting generalizability. Many trials are small, single-center, or focused on non-diabetic cohorts, and direct randomized comparisons of anesthetic regiments specifically in diabetic surgical patients are sparse. Moreover, the clinical significance of modest intraoperative differences in glucose (infection rates, myocardial events, or length of stay) remain incompletely defined
[2]
Akhtar S, Barash PG, Inzucchi SE. Scientific principles and clinical implications of perioperative glucose regulation and control. Anesth Analg. 2010 Feb 1; 110(2): 478-97.
van den Brom CE, Bulte CS, Loer SA, Bouwman RA, Boer C. Diabetes, perioperative ischaemia and volatile anaesthetics: consequences of derangements in myocardial substrate metabolism. Cardiovasc Diabetol. 2013 Mar 4; 12: 42.
Figure 1. Schematic representation of the neuroendocrine stress response to surgery and the sites at which anesthetic agents and techniques modulate perioperative glucose homeostasis.
Given the high prevalence of diabetes in surgical populations and the well-documented association between perioperative hyperglycemia and poor outcomes, clarifying how anesthetic choices influence glucose homeostasis has meaningful implications for perioperative planning and glycemia management protocols. This narrative review synthesizes current evidence on volatile and intravenous anesthetics, adjunctive agents, and regional techniques, with the goal of informing intraoperative monitoring strategies and individualized management plans for patients with diabetes undergoing surgery.
Figure 1. Mechanisms by Which Anesthetic Techniques Influence Perioperative Glucose Homeostasis.
2. Methods
This narrative review was conducted to synthesize current evidence regarding the effects of anesthetics agents and techniques on perioperative glucose regulation in patients with diabetes mellitus. A comprehensive literature search was performed using PubMed, Embased, and Google Scholar for studies published in English through October 2025. The following key terms and their combinations were used: diabetes mellitus, perioperative hyperglycemia, anesthetic agents, volatile anesthesia, total intravenous anesthesia (TIVA), propofol, sevoflurane, isoflurane, desflurane, regional anesthesia, neuraxial block, dexmedetomidine, clonidine, insulin resistance, stress response, and surgical outcomes.
Both clinical studies (randomized controlled trials, cohort studies, case-control studies) and experimental investigations (animal and cellular models) were included to capture mechanistic and translational data relevant to anesthetic-glucose interactions. Systematic reviews and meta-analyses were screened for additional references. Articles were excluded if they (1) focused solely on non-surgical or critical care populations, (2) did not include glucose or insulin-related outcomes, or (3) were editorials or non-peer-reviewed sources.
The selection process involved an initial title and abstract review followed by full text assessment for eligibility. Data were extracted on study by design, population, characteristics (including diabetic type), anesthetic agents or techniques used, glycemic outcomes (intraoperative glucose, insulin levels, stress hormone changes), and postoperative clinical endpoints (infection rates, cardiovascular events, length of stay).
Given the heterogeneity in study designs and outcome measures, findings were summarized descriptively rather than pooled quantitatively. Emphasis was placed on identifying trends in anesthetic-related effects on glucose homeostasis, differences between volatile and intravenous agents, and the potential modulatory roles of adjunctive and regional anesthetic techniques. The synthesis aimed to integrate physiologic mechanisms with clinical outcomes to inform perioperative management strategies for diabetic surgical patients.
3. Results
A total of approximately 120 studies met inclusion criteria, encompassing randomized controlled trials, observational studies, and experimental investigations. Evidence consistently demonstrated that perioperative hyperglycemia remains a frequent and clinically relevant occurrence in diabetic patients, even under established glucose management protocols.
Table 1. Comparative Effects of Common Anesthetic Agents and Techniques on Perioperative Glucose Homeostasis.
Anesthetic Agent/Technique
Effect on Insulin Secretion
Effect on Insulin Resistance
Effect on Stress Hormones
Net Effect on Glucose
Key Mechanism
Overall Glycemic Impact
Sevoflurane/Isoflurane/Desflurane
↑ Impaired β-cell function
↑ Increased
Minimal suppression
↑ Hypergly-cemia
Ion channel & mitochondrial effects
Least favorable
Propofol (TIVA)
Mild ↓ or neutral
Mild ↑ (dose de-pendent)
Blunts SNS modestly
↔ / ↓ com-pared to vola-tiles
Less β-cell suppression
More favorable
Dexmedetomidine
Neutral
↓↓ Cortisol & catecholamines
Sympatholysis
Highly favorable adjunct
Clonidine
Neutral
Sympatholysis
Favorable adjunct
Ketamine
SNS stimulation
Unfavorable in diabetics
Perioperative Steroids
Neutral
Gluconeogenesis
Requires insulin planning
Vasopressors (epi-containing)
Neutral
Adrenergic stimulation
Transient hyperglycemia
Regional/Neuraxial
Preserved
Blocks afferent stress response
Most favorable technique
Table 1. Summary comparison of how commonly used anesthetic agents and techniques influence insulin physiology, stress hormone, release, and perioperative glucose trends in diabetic patients.
3.1. Volatile vs. Intravenous Anesthetics
Across multiple studies, volatile agents, including sevoflurane, isoflurane, and desflurane, were associated with dose-dependent impairments in insulin secretion and peripheral glucose utilization
[8]
Li Y, Zhang J, Liu Y, et al. Isoflurane induces hepatic insulin resistance through oxidative stress and inflammation in mice. J Diabetes Res. 2021; 2021: 5583142.
Kitamura T, Saito M, Yoshida K. Effects of volatile anesthetics on insulin secretion and glucose metabolism. Anesth Analg. 2020; 130(4): 1012–1020.
[10]
Kawano T, Oshita S, Takahashi A, et al. Isoflurane impairs glucose tolerance via inhibition of insulin secretion in humans. Anesthesiology. 2019; 131(1): 113–122.
[8-10]
. Mechanistic investigations attributed these effects to altered pancreatic beta cell ion channel function, mitochondrial oxidative activity, and interference with insulin signaling pathways
[8]
Li Y, Zhang J, Liu Y, et al. Isoflurane induces hepatic insulin resistance through oxidative stress and inflammation in mice. J Diabetes Res. 2021; 2021: 5583142.
. Conversely, propofol-based total intravenous anesthesia (TIVA) was generally associated with lower intraoperative glucose levels and reduced postoperative insulin resistance compared with volatile agents,
[5]
Tanaka K, Nishikawa T, Morimoto Y. Comparison of total intravenous and inhalational anesthesia on perioperative glucose homeostasis in diabetic patients: A randomized controlled trial. Br J Anaesth. 2021; 126(6) 135–1142.
[7]
Chen J, Wang Y, Xu X, et al. Propofol-based anesthesia improves intraoperative glucose stability compared to sevoflurane in patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2020; 13: 481–489.
[5, 7]
although results varied. Some studies noted that prolonged infusions or higher doses of propofol could attenuate these benefits
[12]
Marik PE, Varon J. Perioperative glycemic control: An evidence-based review. J Clin Anesth. 2022; 77: 110627.
Table 2. Volatile Anesthesia vs. Propofol-Based TIVA in Diabetic Surgical Patients.
Feature
Volatile Anesthesia
Propofol TIVA
β-cell insulin secretion
Significantly impaired
Mild or variable effect
Peripheral insulin resistance
Increased
Less pronounced
Intraoperative glucose levels
Higher
Lower
Postoperative insulin requirements
Increased
Reduced in several studies
Mechanistic basis
Mitochondrial dysfunction, ion channel effects
Less β-cell interference
Clinical trend
Greater glucose variability
Improved glucose stability
Table 2. Direct comparison of physiologic and clinical glycemic effects between volatile anesthetics and propofol-based total intravenous anesthesia.
3.2. Adjunctive and Sympathetic Agents
The alpha-2 adrenergic agonists: dexmedetomidine and clonidine demonstrated reproducible reductions in intraoperative glucose excursions and serum cortisol levels in both diabetic and non-diabetic cohorts
[13]
Kim H, Lee S, Park S, et al. Dexmedetomidine attenuates stress-induced hyperglycemia and improves glycemic control in surgical patients. J Anesth. 2022; 36(4): 556–564.
Yildiz M, Tavlan A, Tuncer S, et al. Effect of dexmedetomidine on hemodynamic responses and stress hormones during surgery. Eur J Anaesthesiol. 2020; 37(11): 1045–1051.
. Dexmedetomidine’s attenuation of catecholamine release and inflammatory mediators correlated with improved glycemic stability and, in several studies, reduced postoperative insulin requirements
[19]
Khan ZP, Ferguson CN, Jones RM. Alpha-2 and imidazoline receptor agonists: Their pharmacology and therapeutic role. Anaesthesia. 2019; 74(6): 698–707.
. In contrast, perioperative corticosteroids, epinephrine-containing local anesthetics, and vasopressor infusions were consistently associated with transient hyperglycemia, often necessitating insulin titration or glucose monitoring adjustments
[17]
Glowniak JV, Loriaux DL. A double-blind study on the effects of perioperative dexamethasone on blood glucose in diabetic patients. Anesth Analg. 2018; 126(3): 1110–1116.
Kadoi Y, Saito S. Effect of ketamine and catecholamine activation on glucose metabolism in diabetic and non-diabetic rats. Can J Anaesth. 2018; 65(9): 1053–1060.
Table 3. Impact of Regional and Neuraxial Anesthesia on the Surgical Stress Response and Glycemic Stability.
Mechanism
Effect
Glycemic Result
Blockade of nociceptive afferents
Reduced HPA axis stimulation
Improved peripheral insulin sensitivity
Stable glucose levels
Reduced inflammatory mediators
Reduced postoperative hyperglycemia
Observed clinical outcomes
Improved recovery metrics
Studies evaluating epidural and spinal anesthesia, either as primary techniques or adjuncts to general anesthesia, demonstrated attenuated stress hormone surges and reduced perioperative insulin resistance
[20]
Li M, Zhou X, Huang L, et al. Epidural anesthesia improves perioperative insulin sensitivity and reduces postoperative hyperglycemia in diabetic patients. Anesth Analg. 2020; 131(3): 892–899.
.These findings were most pronounced in abdominal, orthopedic, and lower extremity procedures. Reduced sympathetic activation and lower circulating cortisol and catecholamine levels under regional anesthesia were associated with smaller glucose fluctuations and, in some cohorts, reduced postoperative infection rates and length of stay
[22]
Koh I, Han K, Lee H, et al. Regional anesthesia and postoperative glucose stability: A meta-analysis. Acta Anaesthesiol Scand. 2021; 65(7): 944–952.
Table 3. Physiologic mechanisms by which regional and neuraxial anesthesia blunt the surgical stress response and improve perioperative glucose control.
3.4. Heterogeneity and Limitations
Despite consistent physiologic patterns, substantial heterogeneity was noted across studies regarding diabetes subtype, surgical type and duration, anesthetic regiments, and glycemia targets. Few randomized controlled trials directly compared anesthetic techniques specifically in diabetic surgical populations
[12]
Marik PE, Varon J. Perioperative glycemic control: An evidence-based review. J Clin Anesth. 2022; 77: 110627.
.Moreover, many studies lacked standardized glucose monitoring protocols or robust reporting of clinical outcomes such as wound infection or myocardial events
[5]
Tanaka K, Nishikawa T, Morimoto Y. Comparison of total intravenous and inhalational anesthesia on perioperative glucose homeostasis in diabetic patients: A randomized controlled trial. Br J Anaesth. 2021; 126(6) 135–1142.
[5]
.
4. Conclusions
Current evidence supports a meaningful influence of anesthetic choice and technique on perioperative glucose homeostasis in patients with diabetes mellitus. Volatile anesthetics tend to impair insulin secretion and increase insulin resistance, while propofol-based TIVA and sympatholytic adjuncts such as dexmedetomidine may offer modest glycemic advantages. Regional and neuraxial anesthesia consistently attenuate the neuroendocrine stress response and promote more stable perioperative glucose profiles.
However, existing data are limited by small sample sizes, heterogenous methodologies, and a paucity of trials specifically designed for diabetic surgical cohorts. The clinical significance of modest intraoperative glucose difference, particularly in relation to infection, cardiovascular outcomes, and recovery metrics, remains incompletely defined.
Future research should prioritize prospective, adequately powered trials comparing anesthetics regimens in diabetic patients, incorporating standardized glucose targets, insulin management algorithms, and long-term outcome measures. Understanding the interplay between anesthetic technique, metabolic physiology, and glycemic control will be critical for optimizing perioperative care and improving outcomes in this growing surgical population.
Abbreviations
TIVA
Total Intravenous Anesthesia
Author Contributions
Mariah Ganga: Data Curation, Formal Analysis, Investigation, Resources, Writing – Original Draft
Dan Erdman: Conceptualization, Writing – Review & Editing, Methodology
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2024. Atlanta, GA: US Department of Health and Human Services; 2024.
[2]
Akhtar S, Barash PG, Inzucchi SE. Scientific principles and clinical implications of perioperative glucose regulation and control. Anesth Analg. 2010 Feb 1; 110(2): 478-97.
van den Brom CE, Bulte CS, Loer SA, Bouwman RA, Boer C. Diabetes, perioperative ischaemia and volatile anaesthetics: consequences of derangements in myocardial substrate metabolism. Cardiovasc Diabetol. 2013 Mar 4; 12: 42.
Tanaka K, Nishikawa T, Morimoto Y. Comparison of total intravenous and inhalational anesthesia on perioperative glucose homeostasis in diabetic patients: A randomized controlled trial. Br J Anaesth. 2021; 126(6) 135–1142.
[6]
Xiong X, He Y, Zhou C, Zheng Q, Chen C, Liang P. Impact of total intravenous anesthesia and total inhalation anesthesia as the anesthesia maintenance approaches on blood glucose level and postoperative complications in patients with type 2 diabetes mellitus: a double-blind, randomized controlled trial. BMC Anesthesiol. 2024 Jan 22; 24(1): 36.
Chen J, Wang Y, Xu X, et al. Propofol-based anesthesia improves intraoperative glucose stability compared to sevoflurane in patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2020; 13: 481–489.
[8]
Li Y, Zhang J, Liu Y, et al. Isoflurane induces hepatic insulin resistance through oxidative stress and inflammation in mice. J Diabetes Res. 2021; 2021: 5583142.
Kitamura T, Saito M, Yoshida K. Effects of volatile anesthetics on insulin secretion and glucose metabolism. Anesth Analg. 2020; 130(4): 1012–1020.
[10]
Kawano T, Oshita S, Takahashi A, et al. Isoflurane impairs glucose tolerance via inhibition of insulin secretion in humans. Anesthesiology. 2019; 131(1): 113–122.
[11]
Yasuda Y, Watanabe M, Kobayashi K, et al. Propofol induces insulin resistance through inhibition of insulin receptor signaling. Biochem Biophys Res Commun. 2013; 439(1): 50–54.
Kim H, Lee S, Park S, et al. Dexmedetomidine attenuates stress-induced hyperglycemia and improves glycemic control in surgical patients. J Anesth. 2022; 36(4): 556–564.
Zhou W, Wang J, Yang D, et al. Effects of dexmedetomidine on glucose-related hormones and lactate in non-diabetic patients under general anesthesia. Minerva Anestesiol. 2022; 88(1): 8–15.
Yildiz M, Tavlan A, Tuncer S, et al. Effect of dexmedetomidine on hemodynamic responses and stress hormones during surgery. Eur J Anaesthesiol. 2020; 37(11): 1045–1051.
Gan Y, Li Q, Zhang W, et al. The safety of perioperative dexamethasone with antiemetic dosage in patients with diabetes: a systematic review and meta-analysis. Perioper Med (Lond). 2023; 12: 14.
[17]
Glowniak JV, Loriaux DL. A double-blind study on the effects of perioperative dexamethasone on blood glucose in diabetic patients. Anesth Analg. 2018; 126(3): 1110–1116.
Kadoi Y, Saito S. Effect of ketamine and catecholamine activation on glucose metabolism in diabetic and non-diabetic rats. Can J Anaesth. 2018; 65(9): 1053–1060.
Physiol Rep Editorial Board. The neuro-endocrine stress response compensates for loss of insulin-mediated glucose homeostasis. Physiol Rep. 2023; 11: e15603.
Ganga, M., Erdman, D. (2026). The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review. International Journal of Anesthesia and Clinical Medicine, 14(1), 41-46. https://doi.org/10.11648/j.ijacm.20261401.17
Ganga, M.; Erdman, D. The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review. Int. J. Anesth. Clin. Med.2026, 14(1), 41-46. doi: 10.11648/j.ijacm.20261401.17
Ganga M, Erdman D. The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review. Int J Anesth Clin Med. 2026;14(1):41-46. doi: 10.11648/j.ijacm.20261401.17
@article{10.11648/j.ijacm.20261401.17,
author = {Mariah Ganga and Dan Erdman},
title = {The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {41-46},
doi = {10.11648/j.ijacm.20261401.17},
url = {https://doi.org/10.11648/j.ijacm.20261401.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.17},
abstract = {Anesthesia plays a critical role in modern surgical care by ensuring patient comfort, safety, and physiologic stability. However, the effects of anesthetic agents extend beyond sedation and analgesia and include important, yet often underrecognized, influences on perioperative glucose metabolism. This consideration is particularly relevant in patients with diabetes mellitus, a growing surgical population in whom perioperative hyperglycemia is strongly associated with increased risks of infection, delayed wound healing, cardiovascular complications, and prolonged hospital stay. This narrative review synthesized current clinical and mechanistic evidence regarding how commonly used anesthetic agents and techniques influence perioperative glucose homeostasis. Volatile anesthetics have been shown to impair pancreatic β-cell insulin secretion and promote peripheral insulin resistance through the effect on cellular ion channels, mitochondrial function, and stress hormone pathways, frequently resulting in intraoperative hyperglycemia. In contrast, propofol-based total intravenous anesthesia (TIVA) appears to exert comparatively milder effects on insulin dynamics in many clinical contexts. Adjunctive agents such as dexmedetomidine and clonidine may further stabilize glucose levels through sympatholytic and stress-attenuating mechanisms. Additionally, regional and neuraxial anesthesia consistently demonstrate an ability to blunt the neuroendocrine stress response to surgery, thereby promoting improved glycemic stability. By integrating physiologic mechanisms with clinical findings, this review highlights how anesthetic choice can meaningfully influence perioperative glucose trends. Understanding these interactions is essential for optimizing anesthetic planning, intraoperative monitoring, and glycemic management strategies in diabetic surgical patients.},
year = {2026}
}
TY - JOUR
T1 - The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review
AU - Mariah Ganga
AU - Dan Erdman
Y1 - 2026/03/05
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.17
DO - 10.11648/j.ijacm.20261401.17
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 41
EP - 46
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.17
AB - Anesthesia plays a critical role in modern surgical care by ensuring patient comfort, safety, and physiologic stability. However, the effects of anesthetic agents extend beyond sedation and analgesia and include important, yet often underrecognized, influences on perioperative glucose metabolism. This consideration is particularly relevant in patients with diabetes mellitus, a growing surgical population in whom perioperative hyperglycemia is strongly associated with increased risks of infection, delayed wound healing, cardiovascular complications, and prolonged hospital stay. This narrative review synthesized current clinical and mechanistic evidence regarding how commonly used anesthetic agents and techniques influence perioperative glucose homeostasis. Volatile anesthetics have been shown to impair pancreatic β-cell insulin secretion and promote peripheral insulin resistance through the effect on cellular ion channels, mitochondrial function, and stress hormone pathways, frequently resulting in intraoperative hyperglycemia. In contrast, propofol-based total intravenous anesthesia (TIVA) appears to exert comparatively milder effects on insulin dynamics in many clinical contexts. Adjunctive agents such as dexmedetomidine and clonidine may further stabilize glucose levels through sympatholytic and stress-attenuating mechanisms. Additionally, regional and neuraxial anesthesia consistently demonstrate an ability to blunt the neuroendocrine stress response to surgery, thereby promoting improved glycemic stability. By integrating physiologic mechanisms with clinical findings, this review highlights how anesthetic choice can meaningfully influence perioperative glucose trends. Understanding these interactions is essential for optimizing anesthetic planning, intraoperative monitoring, and glycemic management strategies in diabetic surgical patients.
VL - 14
IS - 1
ER -
Ganga, M., Erdman, D. (2026). The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review. International Journal of Anesthesia and Clinical Medicine, 14(1), 41-46. https://doi.org/10.11648/j.ijacm.20261401.17
Ganga, M.; Erdman, D. The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review. Int. J. Anesth. Clin. Med.2026, 14(1), 41-46. doi: 10.11648/j.ijacm.20261401.17
Ganga M, Erdman D. The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review. Int J Anesth Clin Med. 2026;14(1):41-46. doi: 10.11648/j.ijacm.20261401.17
@article{10.11648/j.ijacm.20261401.17,
author = {Mariah Ganga and Dan Erdman},
title = {The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {41-46},
doi = {10.11648/j.ijacm.20261401.17},
url = {https://doi.org/10.11648/j.ijacm.20261401.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.17},
abstract = {Anesthesia plays a critical role in modern surgical care by ensuring patient comfort, safety, and physiologic stability. However, the effects of anesthetic agents extend beyond sedation and analgesia and include important, yet often underrecognized, influences on perioperative glucose metabolism. This consideration is particularly relevant in patients with diabetes mellitus, a growing surgical population in whom perioperative hyperglycemia is strongly associated with increased risks of infection, delayed wound healing, cardiovascular complications, and prolonged hospital stay. This narrative review synthesized current clinical and mechanistic evidence regarding how commonly used anesthetic agents and techniques influence perioperative glucose homeostasis. Volatile anesthetics have been shown to impair pancreatic β-cell insulin secretion and promote peripheral insulin resistance through the effect on cellular ion channels, mitochondrial function, and stress hormone pathways, frequently resulting in intraoperative hyperglycemia. In contrast, propofol-based total intravenous anesthesia (TIVA) appears to exert comparatively milder effects on insulin dynamics in many clinical contexts. Adjunctive agents such as dexmedetomidine and clonidine may further stabilize glucose levels through sympatholytic and stress-attenuating mechanisms. Additionally, regional and neuraxial anesthesia consistently demonstrate an ability to blunt the neuroendocrine stress response to surgery, thereby promoting improved glycemic stability. By integrating physiologic mechanisms with clinical findings, this review highlights how anesthetic choice can meaningfully influence perioperative glucose trends. Understanding these interactions is essential for optimizing anesthetic planning, intraoperative monitoring, and glycemic management strategies in diabetic surgical patients.},
year = {2026}
}
TY - JOUR
T1 - The Effects of Anesthetic Agents on Perioperative Glucose Homeostasis in Patients with Diabetes: A Narrative Review
AU - Mariah Ganga
AU - Dan Erdman
Y1 - 2026/03/05
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.17
DO - 10.11648/j.ijacm.20261401.17
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 41
EP - 46
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.17
AB - Anesthesia plays a critical role in modern surgical care by ensuring patient comfort, safety, and physiologic stability. However, the effects of anesthetic agents extend beyond sedation and analgesia and include important, yet often underrecognized, influences on perioperative glucose metabolism. This consideration is particularly relevant in patients with diabetes mellitus, a growing surgical population in whom perioperative hyperglycemia is strongly associated with increased risks of infection, delayed wound healing, cardiovascular complications, and prolonged hospital stay. This narrative review synthesized current clinical and mechanistic evidence regarding how commonly used anesthetic agents and techniques influence perioperative glucose homeostasis. Volatile anesthetics have been shown to impair pancreatic β-cell insulin secretion and promote peripheral insulin resistance through the effect on cellular ion channels, mitochondrial function, and stress hormone pathways, frequently resulting in intraoperative hyperglycemia. In contrast, propofol-based total intravenous anesthesia (TIVA) appears to exert comparatively milder effects on insulin dynamics in many clinical contexts. Adjunctive agents such as dexmedetomidine and clonidine may further stabilize glucose levels through sympatholytic and stress-attenuating mechanisms. Additionally, regional and neuraxial anesthesia consistently demonstrate an ability to blunt the neuroendocrine stress response to surgery, thereby promoting improved glycemic stability. By integrating physiologic mechanisms with clinical findings, this review highlights how anesthetic choice can meaningfully influence perioperative glucose trends. Understanding these interactions is essential for optimizing anesthetic planning, intraoperative monitoring, and glycemic management strategies in diabetic surgical patients.
VL - 14
IS - 1
ER -