Remote patient monitoring is frequently used to monitor patients with chronic disease, but patients are often only monitored for a single disease (CHF, COPD, diabetes) using systems designed to monitor only parameters for that disease. However many patients have multiple diseases that must be managed together; systems need to be designed to monitor a multiplicity of parameters. Moreover most patients are elderly and are averse to technology, and so the system has to be designed to be extremely simple to use. We describe our system, designed for simplicity of use and to support multiple types of device to monitor complex conditions. We describe how IEEE 11073 standards were used to integrate proprietary devices to our gateway to create a platform that is plug-and-play interoperable with our data server. We present preliminary results from our clinical study monitoring 68 CHF patients who were taking daily measurements of blood pressure and weight to investigate effects of behavioral change during Ramazan. There was a small decrease in mean diastolic and systolic blood pressure from pre-Ramazan to Ramazan that was significant (diastolic 131.8, 127.0, P=0.0005; systolic 71.4, 69.1. P=0.008), however there was no significant change from Ramazan to post-Ramazan (P=0.4). There was also a reduction in the number of incidents of systolic and diastolic blood pressure exceeding threshold values from pre-Ramazan to Ramazan.
| Published in | International Journal of Biomedical Science and Engineering (Volume 13, Issue 3) |
| DOI | 10.11648/j.ijbse.20251303.14 |
| Page(s) | 72-79 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Remote Patient Monitoring, Telehealth, CHF, Plug and Play Interoperability, Medical Device Standards, IEEE 11073
Disease | Disease | Device |
|---|---|---|
Anti-coagulation | INR PT | |
Congestive Heart Failure | CHF | Blood Pressure Weigh Scale |
Chronic Obstructive Pulmonary Disease | COPD | Pulse Oximeter |
Diabetes | Blood Glucose Blood Pressure | |
Gestational Diabetes | Blood Glucose | |
Hypertension | Blood Pressure | |
Idiopathic Pulmonary Fibrosis | IPF | Pulse Oximeter |
Infection | Temperature | |
Pre-eclampsia | Urine Protein Blood Pressure |
Type | Model | Protocol | Specialization |
|---|---|---|---|
BG Meter | Bioland G-427B | Proprietary | 11073-10417 |
BG Meter | Lifechek TD-4277 | Proprietary | 11073-10417 |
BG Meter | Taidoc TD-4266 | Proprietary | 11073-10417 |
BG Meter | Roche Accuchek | Bluetooth | 11073-10417 |
BP Meter | Bioland 2006-2B | Proprietary | 11073-10407 |
BP Meter | AND UA-651 BLE | Bluetooth | 11073-10407 |
Urine Analyser | Contec BC401 | Proprietary | 11073-10422 |
Pulse oximeter | Contec CMS 50D-BT | Proprietary | 11073-10404 |
Pulse oximeter | Nonin 3230 | Proprietary | 11073-10404 |
Thermometer | Genial Wearable | Proprietary | 11073-10408 |
Weigh scale | Unique CF398BLE | Proprietary | 11073-10415 |
Smart ring | Kingstar | Proprietary | 11073-10441 |
Room temperature | Texas TM101 | Proprietary | 11073-10471 |
PT INR | Proprietary | 11073-10418 | |
GHS | Philips emulator | GHS | Device dependent |
Pre-Ramazan | Ramazan | Post-Ramazan | ||||
|---|---|---|---|---|---|---|
Dias | Sys | Dias | Sys | Dias | Sys | |
Mean | 131.8 | 71.4 | 127 | 69.1 | 126.6 | 68.9 |
S.D. | 26.2 | 16.1 | 21.3 | 14.5 | 19.3 | 14.2 |
Maximum | 242 | 147 | 209 | 165 | 194 | 134 |
Minimum | 69 | 32 | 63 | 32 | 74 | 33 |
Pre-Ramazan-Ramazan | Ramazan-Post-Ramadan | ||
|---|---|---|---|
Dias | Sys | Dias | Sys |
0.0005 | 0.008 | 0.4 | 0.4 |
Threshold | Number measurements | Diastolic | Systolic | ||
|---|---|---|---|---|---|
200 | 80 | 100 | 50 | ||
Pre-Ramazan | 482 | ||||
Number | 4 | 3 | 28 | 21 | |
Percentage | 0.8 | 0.6 | 5.8 | 4.4 | |
Ramazan | 677 | ||||
Number | 2 | 1 | 19 | 21 | |
Percentage | 0.3 | 0.1 | 2.8 | 3.1 | |
Post-Ramazon | 832 | ||||
Number | 0 | 2 | 15 | 61 | |
Percentage | 0.0 | 0.2 | 1.8 | 7.3 | |
BG | Blood Glucose |
BLE | Bluetooth Low Energy |
BP | Blood Pressure |
CHF | Congestive Heart Failure |
COPD | Chronic Obstructive Pulmonary Disease |
EUI-64 | Extended Unique Identifier |
GHS | General Health Sensor |
IHE | Integrating the Healthcare Enterprise |
INR | International Normalized Ratio |
PCD | Point of Care Device |
PT | Prothrombin Time |
RPM | Remote Patient Monitoring |
| [1] | J Fursse, M Clarke, R Jones: “Early Experiences of the Use of Remote Patient Monitoring for the Long Term Management of Chronic Disease”, Journal of Telemedicine & Telecare, 14: 122-4, 2008. |
| [2] | M Clarke, RW Jones, J Fursse, N Connelly-Brown, U Sharma: “Evaluation of the National Health Services (NHS) Direct Telehealth programme: cost-effectiveness analysis”, Telemedicine Journal and eHealth, 24(1): 67-77, 2018, |
| [3] |
P Onyeachu, M Clarke: “A Patient Technology Acceptance Model (PTAM) for Adoption of Telehealth”, Digital Medicine and Healthcare Technology March 2022;
https://doi.org/10.5772/dmht.02 communication. |
| [4] | ISO/IEEE 11073-10206 - Health informatics - Device Interoperability - Part 10206: Personal Health Device Communication - Abstract Content Information Model. |
| [5] | ISO/IEEE 11073-10101 - Health informatics -- Point-of-care medical device communication -- Part 10101: Nomenclature. |
| [6] |
Integrating the Healthcare Enterprise IHE Patient Care Device (PCD) Technical Framework Volume 2.
http://www.ihe.net/uploadedFiles/Documents/PCD/IHE_PCD_TF_Vol2.pdf (last accessed 19-12-2024). |
| [7] |
HL7 Messaging Standard Version 2.6.
http://www.hl7.org/implement/standards/product_brief.cfm?product_id=145 (last accessed 19-12-2024). |
| [8] | Mazidi M, Rezaie P, Chaudhri O, Karimi E, Nematy M. The effect of Ramadan fasting on cardiometabolic risk factors and anthropometrics parameters: A systematic review. Pak J Med Sci. 2015; 31(5): 1250-1255. |
| [9] | Nematy M, Alinezhad-Namaghi M, Rashed MM, et al. Effects of Ramadan fasting on cardiovascular risk factors: a prospective observational study. Nutr J. 2012; 11: 69. Published 2012 Sep 10. |
APA Style
Clarke, M., Gokalp, H., Gedikli, O. (2025). Remote Patient Monitoring of Patients with Complex Medical Conditions. International Journal of Biomedical Science and Engineering, 13(3), 72-79. https://doi.org/10.11648/j.ijbse.20251303.14
ACS Style
Clarke, M.; Gokalp, H.; Gedikli, O. Remote Patient Monitoring of Patients with Complex Medical Conditions. Int. J. Biomed. Sci. Eng. 2025, 13(3), 72-79. doi: 10.11648/j.ijbse.20251303.14
@article{10.11648/j.ijbse.20251303.14,
author = {Malcolm Clarke and Hulya Gokalp and Omer Gedikli},
title = {Remote Patient Monitoring of Patients with Complex Medical Conditions
},
journal = {International Journal of Biomedical Science and Engineering},
volume = {13},
number = {3},
pages = {72-79},
doi = {10.11648/j.ijbse.20251303.14},
url = {https://doi.org/10.11648/j.ijbse.20251303.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijbse.20251303.14},
abstract = {Remote patient monitoring is frequently used to monitor patients with chronic disease, but patients are often only monitored for a single disease (CHF, COPD, diabetes) using systems designed to monitor only parameters for that disease. However many patients have multiple diseases that must be managed together; systems need to be designed to monitor a multiplicity of parameters. Moreover most patients are elderly and are averse to technology, and so the system has to be designed to be extremely simple to use. We describe our system, designed for simplicity of use and to support multiple types of device to monitor complex conditions. We describe how IEEE 11073 standards were used to integrate proprietary devices to our gateway to create a platform that is plug-and-play interoperable with our data server. We present preliminary results from our clinical study monitoring 68 CHF patients who were taking daily measurements of blood pressure and weight to investigate effects of behavioral change during Ramazan. There was a small decrease in mean diastolic and systolic blood pressure from pre-Ramazan to Ramazan that was significant (diastolic 131.8, 127.0, P=0.0005; systolic 71.4, 69.1. P=0.008), however there was no significant change from Ramazan to post-Ramazan (P=0.4). There was also a reduction in the number of incidents of systolic and diastolic blood pressure exceeding threshold values from pre-Ramazan to Ramazan.},
year = {2025}
}
TY - JOUR T1 - Remote Patient Monitoring of Patients with Complex Medical Conditions AU - Malcolm Clarke AU - Hulya Gokalp AU - Omer Gedikli Y1 - 2025/08/16 PY - 2025 N1 - https://doi.org/10.11648/j.ijbse.20251303.14 DO - 10.11648/j.ijbse.20251303.14 T2 - International Journal of Biomedical Science and Engineering JF - International Journal of Biomedical Science and Engineering JO - International Journal of Biomedical Science and Engineering SP - 72 EP - 79 PB - Science Publishing Group SN - 2376-7235 UR - https://doi.org/10.11648/j.ijbse.20251303.14 AB - Remote patient monitoring is frequently used to monitor patients with chronic disease, but patients are often only monitored for a single disease (CHF, COPD, diabetes) using systems designed to monitor only parameters for that disease. However many patients have multiple diseases that must be managed together; systems need to be designed to monitor a multiplicity of parameters. Moreover most patients are elderly and are averse to technology, and so the system has to be designed to be extremely simple to use. We describe our system, designed for simplicity of use and to support multiple types of device to monitor complex conditions. We describe how IEEE 11073 standards were used to integrate proprietary devices to our gateway to create a platform that is plug-and-play interoperable with our data server. We present preliminary results from our clinical study monitoring 68 CHF patients who were taking daily measurements of blood pressure and weight to investigate effects of behavioral change during Ramazan. There was a small decrease in mean diastolic and systolic blood pressure from pre-Ramazan to Ramazan that was significant (diastolic 131.8, 127.0, P=0.0005; systolic 71.4, 69.1. P=0.008), however there was no significant change from Ramazan to post-Ramazan (P=0.4). There was also a reduction in the number of incidents of systolic and diastolic blood pressure exceeding threshold values from pre-Ramazan to Ramazan. VL - 13 IS - 3 ER -
Department of Electrical and Electronic Engineering, Ondokuz Mayis University, Samsun, Turkey
Department of Electrical and Electronic Engineering, Ondokuz Mayis University, Samsun, Turkey
Figure 1. Simple interface.

Figure 2. Simple interface.
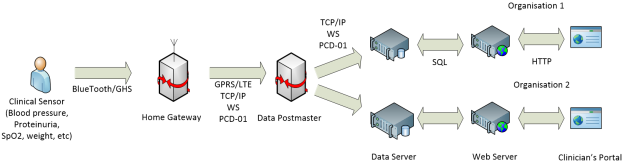
Figure 3. System Architecture.
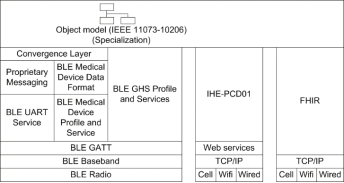
Figure 4. Integration of Devices.

Figure 5. Patient Management.
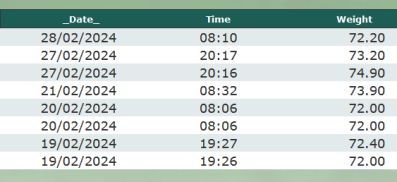
Figure 6. Tabular Display of Patient Data.
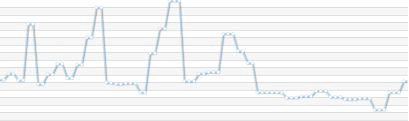
Figure 7. Blood Glucose following change to medication.
Figure 8. Blood Pressure variation in CHF Patient.
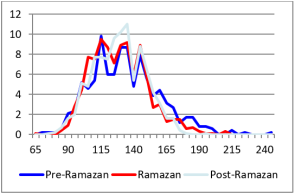
Figure 9. Distribution Diastolic Blood Pressure.
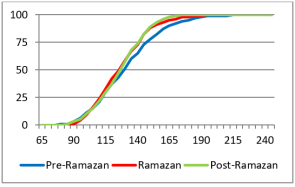
Figure 10. Cumulative Frequency Diastolic Blood Pressure.
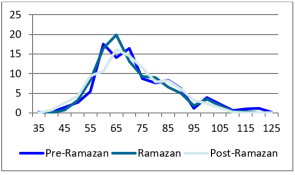
Figure 11. Distribution Systolic Blood Pressure.
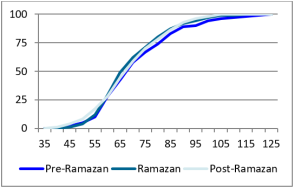
Figure 12. Cumulative Frequency Systolic Blood Pressure.
Information

