Introduction: Patient health condition diagnosis and monitoring using conventional healthcare services delivery is typically time-consuming tiring, expensive and limited in accuracy. Wearable Technology (WT) based on flexible electronics has gained tremendous attention in recent years for Remote Patient Monitoring (RPM) due to its satisfactory features. This technology provides opportunity for disease pre-diagnosis and immediate therapy in order to avoid health crisis. Temperature, as one of the pivotal body vitals for timely detection of abnormality in the human body needs to be continuously measured and monitored. With advent of WT, increase in population, increase in epidemics globally, need for more patient’s participation, increased demand on Physician time and service delivery call for RPM. Attention. Global epidemiology and burden of fever necessitated the Development of Remote Upper Arm Temperature Monitoring (RUATM) Device in adults. Methodology: The device employed DS18D20 temperature sensor, an ESP32 microcontroller, 16*2 Liquid Crystal Display and RUATM server of the developed RUATM mobile application (RUATMiOS). Graphic User Interface (GUI) of RUATMiOS is fed from the system server through its socket. Remotely located physician can access temperature readings of the client on android phones and personal computers for remote monitoring of the patient’s health condition. The RUATM system was tested on 24 individuals from University College Hospital (UCH), Ibadan under supervision of a medical doctor. Its workability, sensitivity, specificity and accuracy was determined. Moreover, its performances compliance with OMCare digital clinical thermometer, an existing was conducted to validate employability of the device in medical service delivery. Results and Discussion: Results of clinical trial of the RUATM system produced Mean readings of 35.41± 0.74 and 35.99± 0.51 for RUATM and clinical thermometer, respectively. Pearson correlation of performance of RUATM system on the digital clinical thermometer was 0.67. This correlation coefficient depicts strong relationships with readings from clinical thermometer. This implies that the developed RUATM device can be effectively used for temperature measurement, and remote temperature monitoring in patients. Recommendations: The developed RUATM system can be enhanced through miniaturization of its size and weight, increased precision, for improved affordability and market competitiveness. GSM communication can also be incorporated because of areas without internet connectivity.
| Published in | International Journal of Biomedical Science and Engineering (Volume 13, Issue 3) |
| DOI | 10.11648/j.ijbse.20251303.16 |
| Page(s) | 87-96 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Remote Patient Monitoring, Vitals, Temperature, Healthcare Service Delivery
S/N | Country | Cases (%) | Death (%) |
|---|---|---|---|
1. | Angola | 3.4 | 2.4 |
2. | Benin | 2.0 | 1.7 |
3. | Burundi | 1.5 | 0.9 |
4. | Burkina Faso | 3.3 | 3.4 |
5. | Central African Republic | 0.7 | 0.8 |
6. | Cameroon | 2.7 | 2.3 |
7. | Chad | 1.4 | 2.0 |
8. | Cote d’ivoire | 3.0 | 2.4 |
9. | Democratic Republic of Congo | 12.3 | 12.6 |
10 | Ethiopia | 1.7 | 1.5 |
11. | Guinea | 1.8 | 1.6 |
12. | Ghana | 2.2 | 2.0 |
13. | India | 1.7 | 1.2 |
14. | Kenya | 1.3 | 1.9 |
15. | Liberia | 0.8 | 0.6 |
16. | Madagascar | 1.6 | 1.6 |
17. | Malawi | 1.7 | 1.2 |
18. | Mali | 3.1 | 3.3 |
19. | Mozambique | 4.1 | 3.8 |
20. | Niger | 3.2 | 3.9 |
21. | Nigeria | 26.6 | 31.3 |
22. | Rwanda | 1.2 | 1.2 |
23. | South Sudan | 1.2 | 1.2 |
24. | Sudan | 1.3 | 1.2 |
25 | Senegal | 0.7 | |
26. | Sierra Leone | 1.1 | 1.4 |
27. | Togo | 0.8 | 0.6 |
28 | Uganda | 5.1 | 3.2 |
29. | United Republic of Tanzania | 3.1 | 4.1 |
30. | Zambia | 1.4 | 1.4 |
31. | Others | 4.4 | 3.7 |
S/N | RUATM | Clinical Thermometer (OMCare) | S/N | RUATM | Clinical Thermometer (OMCare) |
|---|---|---|---|---|---|
1. | 36.19 | 36.20 | 13. | 35.38 | 36.20 |
2. | 35.50 | 35.10 | 14 | 36.06 | 36.20 |
3. | 36.08 | 36.80 | 15. | 36.50 | 36.60 |
4. | 35.56 | 35.80 | 16. | 36.19 | 36.50 |
5. | 34.90 | 34.80 | 17. | 36.31 | 36.50 |
6. | 35.31 | 35.90 | 18. | 35.69 | 35.80 |
7. | 36.31 | 36.10 | 19. | 36.50 | 36.40 |
8. | 35.25 | 35.40 | 20. | 35.38 | 35.80 |
9. | 35.44 | 35.50 | 21. | 36.38 | 36.70 |
10. | 35.13 | 36.70 | 22. | 35.44 | 35.40 |
11. | 35.25 | 35.90 | 23. | 36.19 | 36.10 |
12. | 38.81 | 35.80 | 24. | 35.38 | 35.60 |
BMI | Body Mass Index |
RPM | Remote Patient Monitoring |
CAD | Computer Aided Design |
TP | True Positive |
FP | False Positive |
TN | True Negative |
FN | False Negative |
LCD | Liquid Crystal Display |
RUATM | Remote Upper Arm Temperature Monitoring |
S/N | Authors and Year | Characteristics/ Features | Location of Measurements | Sensor(s) employed | Communi Cation | Accuracy | Limitation | Recommendation |
|---|---|---|---|---|---|---|---|---|
1. | Etienne [12] . | Ingestible temperature-sensing pill, Bland-Altman | Wrist-worn | and Regression | ||||
2. | Ghassemi [19] . | Temperature measurement | NA | MAX30205, Arduino UNO | GSM (SMS) | 0.1°C | I Km distance and 2.4 to 3.6 volts | Distance limitation |
3. | Ko Ko [22] | Temperature, Heart rate, Blood pressure, SPO2, Blood sugar | Hand held | |||||
4. | Alam [20] . | Heart beat (Photo diode) and temperature (LM35 IC) | Fingertip | Wireless Body Area Network (GSM 850MHz) | 5 volts | |||
5. | Fajrin [23] . | Temperature (DS18B20) | Any part of the body. | Atmega328 | GSM (SMS) and Bluetooth | 0.829% | ||
6. | Parihar, Tonge and Ganorkar [21] . | Temperature (LM35) and heartbeat (LM358) | Atmega328 | LCD and nRF module | NA | It was a proposed framework | Recommended for implementation | |
7. | Alam, Sutan and Alam [20] | Temperature and heartbeat (optical technology) | Fingertip | LM35 IC and IR sensors. PIC16F73 microcontroller, Wireless Area Network | GSM (SMS) to remote physician | NA | It was compared to ascertain its reliability |
| [1] | Mayada, Mohzir and Ahmed, (2023). Performance evaluation of a low-cost real time COVID-19 health monitoring system. Journal of Electrical System and Information Technology, 10(30): 1-13. |
| [2] | Claggett J., Stacie P., Joshi A., Ponzio T., and Kirkendall E., (2024). An infrastructure Framework for Remote Patient Monitoring Interventions and Research. Journal of Medical Internet Research, vol. 26, pp. 1-14. |
| [3] | Manta, O., Vasileiou, N., Giannakopoulou, O., Bromis, K., Kouris, I., Haritou, M., Koumakis, L., Spanoudakis, G., Nicolae, I., Nechifor, C., Kokkonidis, M., Vakalelis, M., Goletsis, Y., Roumpi, M., Fotiadis, D., Galanis, H., Dimitrakopoulos, P., Matsopoulos, G. and Koutsouris, D., (2024). Architectural Design for Enhancing Remote Patient Monitoring in Heart Failure: A Case Study of the RETENTION Project. In Proceedings of the 17th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2024) - Volume 2, pages 708-715. |
| [4] | Card A., (2023). Realizing the potential of remote patient monitoring. Definitive Healthcare: Discover Opportunity, 1-23. |
| [5] | Thomas E. E., Taylor M. L., Bandury A., Snowell C. L., Haydon H. M., Rejas V. M. G, Smith A. C. and Caffery L. J., (2021). Factors influencing the effectiveness of remote patient monitoring. Biomedical Journal, Vol. 11, pp. 1-9. |
| [6] | Boyd S. (2024). Wearable Technology for Health Monitoring and Diagnostics. Journal of Computing and Engineering, issue No. 5, 33-44. |
| [7] | Adeghe, E. P., Okolo, C. A., Ojeyinka O. T., (2024). A review of wearable technology in healthcare: Monitoring patient health and enhancing outcomes. Open access research journal of Multidisciplinary Studies, 07(01): 142-148. |
| [8] | Ding S. and Wang X., (2020). Medical Remote Monitoring of Multiple Physiological Parameters Based on Wireless Embedded Internet. IEEE Special Section on Deep Learning Algorithms for Internet of Medical Things. Vol. 8 pp. 78279-78292. |
| [9] | Stevenson L. W., Ross H. J., Rathman L. D., and Boehmer, J. P., (2023). Remote Monitoring for Heart Failure Management at Home. Journal of the American College of Cardiology, 81(23): 2272-2291. |
| [10] | Sun G., Matsui T., Watai Y., Kim S., Kirimoto T., Suzuki S. and Hakozaki Y., (2018), Vital- Scope: Design and Evaluation of a Smart Vital Sign Monitor for Simultaneous Measurement of Pulse Rate, respiratory Rate, and Body temperature for Patient Monitoring. Journal of Sensors, pp. 1-7. |
| [11] | Son S., Yao B. R. and Zhang H. Y., (2023). Reference Standards for Digital Infrared Thermography Measuring Surface Temperature of the Upper Limbs. Bioengineering, 10(671): 1-16. |
| [12] | Etienne S., Oliveras R., Schiboni G., Durrer L., Rochat F., Eib P., Zahner M., Osthoff M., Bassetti S. and Eckstein J. (2023). " Free-living core body temperature monitoring using a wrist -worn sensor after COVID-19 booster vaccination: a pilot study." Biomedical Engineering, 22(23): 1-12. |
| [13] | World health Organization (2023). World Health Statistics 2023: Monitoring health for SDGs, Sustainable Development Goals, World Health Organization, pp. 41-42. |
| [14] | World Health Organization (2024). World Health Statistics 2024: Monitoring health for SDGs, Sustainable Development Goals, World Health Organization, pp. 12-22. |
| [15] | Biokanyo K., Zungeru A. M., Sigwent, B., Yahya, Lebekwe C. (2023). Remote Patient Monitoring System: Applications, Architecture, and Challenges. Information Technology and Engineering, Vol., 20 pp. 1-29. Website: |
| [16] | Qiao D., Ayesa A., Z. F. M. R. J. N., (2022). Remote vital signs measurement using smartphone video camera, |
| [17] | Khairi, N. A., Jambek, A. B., Boon, T. W., and Hashim, U. (2013), "Design and analysis of a wireless temperature monitoring system.", RSM 2013 IEEE Regional Symposium on Micro and Nanoelectronics, |
| [18] | Mazdeyasma S., Ghassemi P. and Wang Q., (2023). Best Practicess for Body Temperature Measurement with Infrared Thermography: External Factors Affecting Accuracy, Sensor, 23, 8011. |
| [19] | Alam M. W., Sultana T. and Alam M. S. (2016). A Heartbeat and Temperature Measuring System for Remote Health Monitoring using Wireless Body Area Network. International Journal of Bio-Science and Bio-Technology, 8(1): 171-190. |
| [20] | Parihar V. R., Tonge, A. Y. and Ganorkar, P. D. (2017). Heartbeat and Temperature Monitoring System for Remote Patients using Arduino. International Journal of Advanced Engineering Research and Science (IJAERS), 4(5): 55-58. |
| [21] | Ko Ko H. Y, Tripathi N. K., Mozumder C., Muengtaweepongsa S. and Pal I., (2023). Real-Time Remote Patient Monitoring and Alarming System for Noncommunicable Lifestyle Diseases, Hindawi, Internaional Journal of Telemedicine and Applications, pp. 1-13. |
| [22] | Fajrin H. R., Ilahi M. R., Handoko B. S. and Sari I. P. (2019). Body Temperature Monitoring Based Telemedicine. The 1st International Conference on Engineering and Applied Science, Journal of Physics: Conference Series, Vol. 1381, pp. 1-11. |
| [23] | Tayal M., Mukherjee A., Chauhan U., Uniyal M., Garg S., Singh A., Bhadoria A. S. and Kant R., (2020). Evaluation of Remote Monitoring Device for Monitoring Vital Parameters against Reference Standard: A Diagnostic Validation Study for COVID-19 Preparedness. Indian Journal of Community Medicine, 45(2): 234-249. |
APA Style
Olusean, A. B., Johnson, A. M., Stanley, M. O., Osita, A. C. (2025). Development of a Remote Upper Arm Temperature Monitoring Device in Adults. International Journal of Biomedical Science and Engineering, 13(3), 87-96. https://doi.org/10.11648/j.ijbse.20251303.16
ACS Style
Olusean, A. B.; Johnson, A. M.; Stanley, M. O.; Osita, A. C. Development of a Remote Upper Arm Temperature Monitoring Device in Adults. Int. J. Biomed. Sci. Eng. 2025, 13(3), 87-96. doi: 10.11648/j.ijbse.20251303.16
AMA Style
Olusean AB, Johnson AM, Stanley MO, Osita AC. Development of a Remote Upper Arm Temperature Monitoring Device in Adults. Int J Biomed Sci Eng. 2025;13(3):87-96. doi: 10.11648/j.ijbse.20251303.16
@article{10.11648/j.ijbse.20251303.16,
author = {Adegoke Benjamin Olusean and Ayoola Mayowa Johnson and Michael Obaro Stanley and Anyaeche Christopher Osita},
title = {Development of a Remote Upper Arm Temperature Monitoring Device in Adults
},
journal = {International Journal of Biomedical Science and Engineering},
volume = {13},
number = {3},
pages = {87-96},
doi = {10.11648/j.ijbse.20251303.16},
url = {https://doi.org/10.11648/j.ijbse.20251303.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijbse.20251303.16},
abstract = {Introduction: Patient health condition diagnosis and monitoring using conventional healthcare services delivery is typically time-consuming tiring, expensive and limited in accuracy. Wearable Technology (WT) based on flexible electronics has gained tremendous attention in recent years for Remote Patient Monitoring (RPM) due to its satisfactory features. This technology provides opportunity for disease pre-diagnosis and immediate therapy in order to avoid health crisis. Temperature, as one of the pivotal body vitals for timely detection of abnormality in the human body needs to be continuously measured and monitored. With advent of WT, increase in population, increase in epidemics globally, need for more patient’s participation, increased demand on Physician time and service delivery call for RPM. Attention. Global epidemiology and burden of fever necessitated the Development of Remote Upper Arm Temperature Monitoring (RUATM) Device in adults. Methodology: The device employed DS18D20 temperature sensor, an ESP32 microcontroller, 16*2 Liquid Crystal Display and RUATM server of the developed RUATM mobile application (RUATMiOS). Graphic User Interface (GUI) of RUATMiOS is fed from the system server through its socket. Remotely located physician can access temperature readings of the client on android phones and personal computers for remote monitoring of the patient’s health condition. The RUATM system was tested on 24 individuals from University College Hospital (UCH), Ibadan under supervision of a medical doctor. Its workability, sensitivity, specificity and accuracy was determined. Moreover, its performances compliance with OMCare digital clinical thermometer, an existing was conducted to validate employability of the device in medical service delivery. Results and Discussion: Results of clinical trial of the RUATM system produced Mean readings of 35.41± 0.74 and 35.99± 0.51 for RUATM and clinical thermometer, respectively. Pearson correlation of performance of RUATM system on the digital clinical thermometer was 0.67. This correlation coefficient depicts strong relationships with readings from clinical thermometer. This implies that the developed RUATM device can be effectively used for temperature measurement, and remote temperature monitoring in patients. Recommendations: The developed RUATM system can be enhanced through miniaturization of its size and weight, increased precision, for improved affordability and market competitiveness. GSM communication can also be incorporated because of areas without internet connectivity.
},
year = {2025}
}
TY - JOUR T1 - Development of a Remote Upper Arm Temperature Monitoring Device in Adults AU - Adegoke Benjamin Olusean AU - Ayoola Mayowa Johnson AU - Michael Obaro Stanley AU - Anyaeche Christopher Osita Y1 - 2025/09/15 PY - 2025 N1 - https://doi.org/10.11648/j.ijbse.20251303.16 DO - 10.11648/j.ijbse.20251303.16 T2 - International Journal of Biomedical Science and Engineering JF - International Journal of Biomedical Science and Engineering JO - International Journal of Biomedical Science and Engineering SP - 87 EP - 96 PB - Science Publishing Group SN - 2376-7235 UR - https://doi.org/10.11648/j.ijbse.20251303.16 AB - Introduction: Patient health condition diagnosis and monitoring using conventional healthcare services delivery is typically time-consuming tiring, expensive and limited in accuracy. Wearable Technology (WT) based on flexible electronics has gained tremendous attention in recent years for Remote Patient Monitoring (RPM) due to its satisfactory features. This technology provides opportunity for disease pre-diagnosis and immediate therapy in order to avoid health crisis. Temperature, as one of the pivotal body vitals for timely detection of abnormality in the human body needs to be continuously measured and monitored. With advent of WT, increase in population, increase in epidemics globally, need for more patient’s participation, increased demand on Physician time and service delivery call for RPM. Attention. Global epidemiology and burden of fever necessitated the Development of Remote Upper Arm Temperature Monitoring (RUATM) Device in adults. Methodology: The device employed DS18D20 temperature sensor, an ESP32 microcontroller, 16*2 Liquid Crystal Display and RUATM server of the developed RUATM mobile application (RUATMiOS). Graphic User Interface (GUI) of RUATMiOS is fed from the system server through its socket. Remotely located physician can access temperature readings of the client on android phones and personal computers for remote monitoring of the patient’s health condition. The RUATM system was tested on 24 individuals from University College Hospital (UCH), Ibadan under supervision of a medical doctor. Its workability, sensitivity, specificity and accuracy was determined. Moreover, its performances compliance with OMCare digital clinical thermometer, an existing was conducted to validate employability of the device in medical service delivery. Results and Discussion: Results of clinical trial of the RUATM system produced Mean readings of 35.41± 0.74 and 35.99± 0.51 for RUATM and clinical thermometer, respectively. Pearson correlation of performance of RUATM system on the digital clinical thermometer was 0.67. This correlation coefficient depicts strong relationships with readings from clinical thermometer. This implies that the developed RUATM device can be effectively used for temperature measurement, and remote temperature monitoring in patients. Recommendations: The developed RUATM system can be enhanced through miniaturization of its size and weight, increased precision, for improved affordability and market competitiveness. GSM communication can also be incorporated because of areas without internet connectivity. VL - 13 IS - 3 ER -
Department of Biomedical Engineering, Faculty of Technology, University of Ibadan, Ibadan, Nigeria
Department of Biomedical Engineering, Faculty of Technology, University of Ibadan, Ibadan, Nigeria
Department of Pharmacology and Therapeutics, College of Medicine, University College Hospital, University of Ibadan, Ibadan, Nigeria
Department of Industrial Production Engineering, Faculty of Technology, University of Ibadan, Ibadan, Nigeria
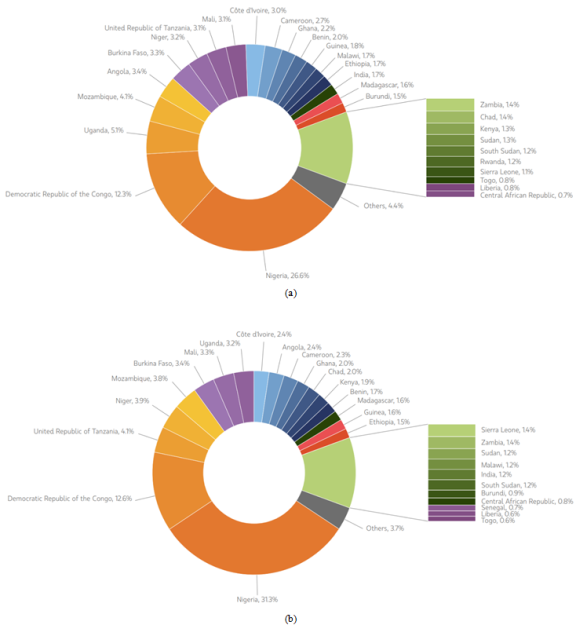
Figure 1. a. African Cases of Malaria in every 1,000. b. African cases of death in every 1000.
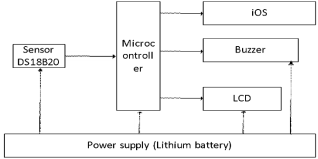
Figure 2. Block diagram of UARTM.
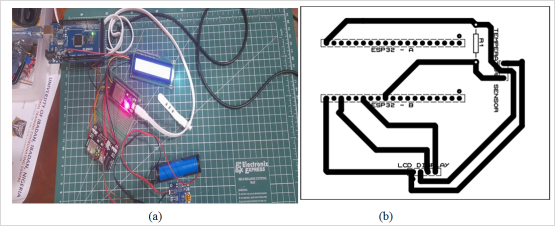
Figure 3. Circuitry of the UARTM system.
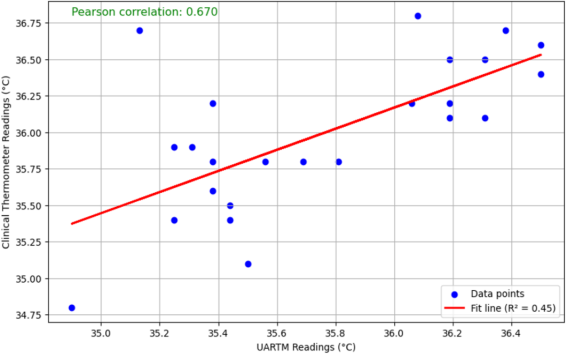
Figure 4. Scatter Plots of Data of the Readings of UARTM and digital clinical thermometer.
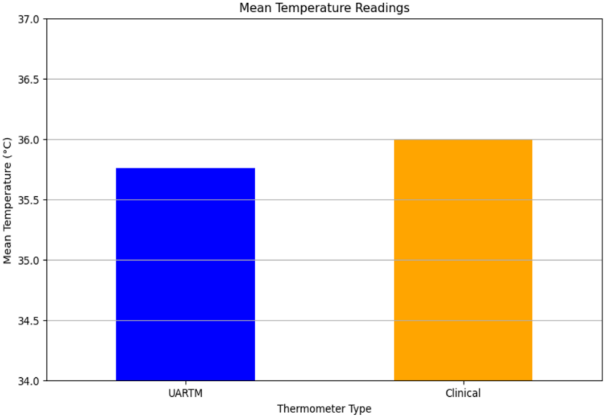
Figure 5. Bar chart of UARTM and digital clinical thermometer.
Information

