Mastocytosis encompasses a rare group of diseases characterized by the accumulation of mast cells, primarily in the skin or internal organs. In the 2016 revised WHO classification, mastocytosis is divided into cutaneous mastocytosis (CM), systemic mastocytosis (CM), and localized mast cell tumor. Cutaneous mastocytosis (CM) includes maculo-papular CM/urticaria pigmentosa (UP), diffuse CM and cutaneous mastocytoma. Urticaria pigmentosa is the most common skin variant. It presents with erythematous brownish macules or papules, often accompanied by pruritus. A case of a 48-year-old woman with disseminated, mildly pruritic, sharply demarcated, livid-brownish macules on the skin of the trunk and extremities is presented. A positive Darier symptom was established. Laboratory tests revealed granulocytosis (73%) and lymphocytosis (19.8%). Serum tryptase and 24-hour urine 5-hydroxyindoleacetic acid were not elevated. The diagnosis of urticaria pigmentosa was confirmed by the histopathological examination revealing perivascular infiltrates of mast cells, mainly in the deep dermis. Screening performed did not detect systemic involvement. Symptomatic treatment with H1 and H2 blockers and topical corticosteroid was carried out. Avoidance of triggers is recommended. The patient's condition has improved. Both a historical review of mastocytosis and a revised classification, as well as the epidemiology, etiology with triggering factors, clinical presentation, laboratory investigations, and management of urticaria pigmentosa are presented.
| Published in | International Journal of Clinical Dermatology (Volume 7, Issue 1) |
| DOI | 10.11648/j.ijcd.20240701.16 |
| Page(s) | 30-35 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Mastocytosis, Urticaria Pigmentosa, Cutaneous Mastocytosis, Systemic Mastocytosis, KIT Gene Mutations, Symptomatic Treatment
| [1] | Caplan R. The natural course of urticaria pigmentosa. Arch Dermatol. 1963; 87: 146–157. |
| [2] | Brockow K, Akin C, Huber M, et al. Assessment of the extent of cutaneous involvement in children and adults with mastocytosis: relationship to symptomatology, tryptase levels, and bone marrow pathology. J Am Acad Dermatol. 2003; 48(4): 508–516. |
| [3] | Ben-Amitai D, Metzker A, Cohen HA. Pediatric cutaneous mastocytosis: a review of 180 patients. Isr Med Assoc J. 2005; 7(5): 320-322. |
| [4] | González-Díaz S, Arias-Cruz A, Mejia K, et al. Urticaria Pigmentosa. Case Report. World Allergy Organ J. 2012; 5(Suppl 2): S203–S204. |
| [5] | Brockow K. Epidemiology, Prognosis, and Risk Factors in Mastocytosis. Immunol Allergy Clin North America. 2014; 34(2): 283–295. |
| [6] | Heinze A, Kuemmet TJ, Chiu YE, et al. Longitudinal Study of Pediatric Urticaria Pigmentosa. Pediatr Dermatol. 2017; 34(2): 144-149. |
| [7] | Kayiran MA, Akdeniz N. Diagnosis and treatment of urticaria in primary care. North Clin Istanb. 2019; 6(1): 93-99. |
| [8] | Valent P, Escribano L, Broesby-Olsen S, et al. Proposed diagnostic algorithm for patients with suspected mastocytosis: A proposal of the European Competence Network on Mastocytosis. Allergy. 2014; 69(10): 1267–1274. |
| [9] | Theoharides TC, Valent P, Akin C. Mast Cells, Mastocytosis, and Related Disorders. N Engl J Med. 2015; 373(2): 163–172. |
| [10] | Pardanani A. Systemic mastocytosis in adults: 2017 update on diagnosis, risk stratification and management. Am J Hematol. 2016; 91(11): 1146-1159. |
| [11] | Wagner N, Staubach P. Mastocytosis – pathogenesis, clinical manifestation and treatment, 2018 Deutsche Dermatologische Gesellschaft (DDG). Publ John Wiley & Sons Ltd., JDDG. |
| [12] | Hartmann K, Escribano L, Grattan, et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology. J Allergy Clin Immunol. 2016; 137(1): 35-45. |
| [13] | Valent P, Oude Elberink JNG, Gorska A, et al. The Data Registry of the European Competence Network on Mastocytosis (ECNM): Set Up, Projects, and Perspectives. J Allergy Clin Immunol Pract. 2019; 7(1): 81–87. |
| [14] | Nettleship E, Tay W. Reports of Medical and Surgical Practice in the Hospitals of Great Britain. Br Med J. 1869; 2(455): 323–324. |
| [15] | Unna, P. Beiträge zur Anatomie und Pathogenese der Urticaria simplex und pigmentosa. MSCCH Prakt Dermatol Suppl Dermatol Stud. 1887; 3: 9. |
| [16] | Sézary A, Levy-Coblentz G, Chauvillon P. Dermographisme et mastocytose. Bull Soc Fr Dermatol Syphiligr. 1936; 43: 359–361. |
| [17] | Valent P, Akin C, Metcalfe DD. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood. 2017; 129(11): 1420-1427. |
| [18] | Castells M, Metcalfe DD, Escribano L. Diagnosis and treatment of cutaneous mastocytosis in children: practical recommendations. Am J Clin Dermatol. 2011; 12(4): 259-270. |
| [19] | Nagata H, Worobec AS, Oh CK, et al. Identification of a point mutation in the catalytic domain of the protooncogene c-kit in peripheral blood mononuclear cells of patients who have mastocytosis with an associated hematologic disorder. Proc Natl Acad Sci USA. 1995; 92(23): 10560–10564. |
| [20] | Akin C, Kirschenbaum AS, Semere T, et al. Analysis of the surface expression of c-kit and occurrence of the c-kit Asp816Val activating mutation in T cells, B cells, and myelomono-cytic cells in patients with mastocytosis. Exp Hematol 2000; 28(2): 140–147. |
| [21] | Sundstrom M, Vliagoftis H, Karlberg P, et al. Functional and phenotypic studies of two variants of a human mast cell line with a distinct set of mutations in the c-kit proto-oncogene. Immunology. 2003; 108(1): 89–97. |
| [22] | Cruse G, Metcalfe DD, Olivera A. Functional Deregulation of KIT. Immunol Allergy Clin North Am. 2014; 34(2): 219–237. |
| [23] | Arock M, Sotlar, K, Akin C, et al. KIT mutation analysis in mast cell neoplasms: Recommendations of the European Competence Network on Mastocytosis. Leukemia. 2015; 29(6): 1223–1232. |
| [24] | Avshalumov K, Pichardo R, Jorizzo JL, et al. Bullous mastocytosis: report of a patient and a brief review of the literature. Am J Dermatopathol. 2008; 30(5): 455-57. |
| [25] | Nirmal B, Krishnaram AS, Muthu Y, et al. Dermatoscopy of Urticaria Pigmentosa with and without Darier's Signin Skin of Colour. Indian Dermatol Online J. 2019; 10(5): 577-579. |
| [26] | Garriga MM, Friedman MM, Metcalfe DD. A survey of the number and distribution of mast cells in the skin of patients with mast cell disorders. J Allergy Clin Immunol. 1988; 82(3 Pt 1): 425–432. |
| [27] | Horny HP, Sotlar K, Valent P. Mastocytosis: state of the art. Pathobiology. 2007; 74(2): 121–132. |
| [28] | Horny HP, Akin C, Arber D, et al. Mastocytosis. In: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Eds: Swerdlow SH, Campo E, Harris NL et al..; IARC Press. Lyon, France; 2017: 62–69. |
| [29] | Orlova AS, Shkurlatovskaia KM, Silina EV, et al. Laboratory tests in diagnosis of Mastocytosis: Literature review and case report. 2020; |
| [30] | Metcalfe DD. The treatment of mastocytosis. J Invest Dermatol 1991; 96(3): 55S–56S. |
| [31] | Arock M, Akin C, Hermine O, et al. Current treatment options in patients with mastocytosis: status in 2015 and future perspectives. Eur J Haematol 2015; 94(6): 474-490. |
| [32] | Valent P, Akin C, Hartmann K, et al. Advances in the Classification and Treatment of Mastocytosis: Current Status and Outlook toward the Future. Cancer Res. 2017; 77(6): 1261-1270. |
| [33] | Brazzelli V, Grassi S, Merante S, et al. Narrow-band UVB phototherapy and psoralen-ultraviolet A photochemotherapy in the treatment of cutaneous mastocytosis: a study in 20 patients. Photodermatol Photoimmunol Photomed. 2016; 32(5-6): 238-246. |
| [34] | Pyatilova P, Teplyuk N, Olisova O, et al. Efficacy of PUVA in Russian patients with mastocytosis: A case series and review of literature. Int J Dermatol. 2018; 57(9): e59–e64. |
| [35] | Correia O, Duarte AF, Quirino P, et al. Cutaneous mastocytosis: Two pediatric cases treated with topical pimecrolimus. Dermatol Online J. 2010 May 15; 16(5): 8. |
| [36] | Valent P, Akin C, Gleixner KV, et al. Multidisciplinary Challenges in Mastocytosis and How to Address with Personalized Medicine Approaches. Int J Mol Sci. 2019; 20(12): 1-17. |
| [37] | Broesby-OlsenS, Dybedal I, Gulen T, et al. Multidisciplinary management of mastocytosis: Nordic expert group consensus. Acta Derm Venereol. 2016; 96(5): 602-612. |
| [38] | Dewachter P, Castells MC, Hepner DL, et al. Perioperative management of patients with mastocytosis. Anesthesiology. 2014; 120(3): 753-759. |
| [39] | Matito A, Morgado JM, SanchezLP, et al. Management of anesthesia in adult and pediatric mastocytosis: A study of the spanish network on mastocytosis (REMA) based on 726 anesthetic procedures. Int Arch Allergy Immunol 2015; 167(1): 47-56. |
| [40] | Zanoni G, Zanotti R, Schena D, et al. Vaccination management in children and adults with mastocytosis. Clin Exp Allergy. 2017; 47(4): 593-596. |
| [41] | Turk J, Oates JA, Roberts LJ. Intervention with epinephrine in hypotension associated with mastocytosis. J Allergy Clin Immunol. 1983; 71(2): 189–192. |
APA Style
Yungareva, I., Broshtilova, V., Smilov, N., Trenovski, A., Velevska, Y., et al. (2024). Urticaria Pigmentosa – A Case Report with a Review of the Literature. International Journal of Clinical Dermatology, 7(1), 30-35. https://doi.org/10.11648/j.ijcd.20240701.16
ACS Style
Yungareva, I.; Broshtilova, V.; Smilov, N.; Trenovski, A.; Velevska, Y., et al. Urticaria Pigmentosa – A Case Report with a Review of the Literature. Int. J. Clin. Dermatol. 2024, 7(1), 30-35. doi: 10.11648/j.ijcd.20240701.16
AMA Style
Yungareva I, Broshtilova V, Smilov N, Trenovski A, Velevska Y, et al. Urticaria Pigmentosa – A Case Report with a Review of the Literature. Int J Clin Dermatol. 2024;7(1):30-35. doi: 10.11648/j.ijcd.20240701.16
@article{10.11648/j.ijcd.20240701.16,
author = {Irina Yungareva and Valentina Broshtilova and Nencho Smilov and Aleksandar Trenovski and Yoanna Velevska and Petar Vatov and Sonya Marina},
title = {Urticaria Pigmentosa – A Case Report with a Review of the Literature
},
journal = {International Journal of Clinical Dermatology},
volume = {7},
number = {1},
pages = {30-35},
doi = {10.11648/j.ijcd.20240701.16},
url = {https://doi.org/10.11648/j.ijcd.20240701.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20240701.16},
abstract = {Mastocytosis encompasses a rare group of diseases characterized by the accumulation of mast cells, primarily in the skin or internal organs. In the 2016 revised WHO classification, mastocytosis is divided into cutaneous mastocytosis (CM), systemic mastocytosis (CM), and localized mast cell tumor. Cutaneous mastocytosis (CM) includes maculo-papular CM/urticaria pigmentosa (UP), diffuse CM and cutaneous mastocytoma. Urticaria pigmentosa is the most common skin variant. It presents with erythematous brownish macules or papules, often accompanied by pruritus. A case of a 48-year-old woman with disseminated, mildly pruritic, sharply demarcated, livid-brownish macules on the skin of the trunk and extremities is presented. A positive Darier symptom was established. Laboratory tests revealed granulocytosis (73%) and lymphocytosis (19.8%). Serum tryptase and 24-hour urine 5-hydroxyindoleacetic acid were not elevated. The diagnosis of urticaria pigmentosa was confirmed by the histopathological examination revealing perivascular infiltrates of mast cells, mainly in the deep dermis. Screening performed did not detect systemic involvement. Symptomatic treatment with H1 and H2 blockers and topical corticosteroid was carried out. Avoidance of triggers is recommended. The patient's condition has improved. Both a historical review of mastocytosis and a revised classification, as well as the epidemiology, etiology with triggering factors, clinical presentation, laboratory investigations, and management of urticaria pigmentosa are presented.
},
year = {2024}
}
TY - JOUR T1 - Urticaria Pigmentosa – A Case Report with a Review of the Literature AU - Irina Yungareva AU - Valentina Broshtilova AU - Nencho Smilov AU - Aleksandar Trenovski AU - Yoanna Velevska AU - Petar Vatov AU - Sonya Marina Y1 - 2024/06/19 PY - 2024 N1 - https://doi.org/10.11648/j.ijcd.20240701.16 DO - 10.11648/j.ijcd.20240701.16 T2 - International Journal of Clinical Dermatology JF - International Journal of Clinical Dermatology JO - International Journal of Clinical Dermatology SP - 30 EP - 35 PB - Science Publishing Group SN - 2995-1305 UR - https://doi.org/10.11648/j.ijcd.20240701.16 AB - Mastocytosis encompasses a rare group of diseases characterized by the accumulation of mast cells, primarily in the skin or internal organs. In the 2016 revised WHO classification, mastocytosis is divided into cutaneous mastocytosis (CM), systemic mastocytosis (CM), and localized mast cell tumor. Cutaneous mastocytosis (CM) includes maculo-papular CM/urticaria pigmentosa (UP), diffuse CM and cutaneous mastocytoma. Urticaria pigmentosa is the most common skin variant. It presents with erythematous brownish macules or papules, often accompanied by pruritus. A case of a 48-year-old woman with disseminated, mildly pruritic, sharply demarcated, livid-brownish macules on the skin of the trunk and extremities is presented. A positive Darier symptom was established. Laboratory tests revealed granulocytosis (73%) and lymphocytosis (19.8%). Serum tryptase and 24-hour urine 5-hydroxyindoleacetic acid were not elevated. The diagnosis of urticaria pigmentosa was confirmed by the histopathological examination revealing perivascular infiltrates of mast cells, mainly in the deep dermis. Screening performed did not detect systemic involvement. Symptomatic treatment with H1 and H2 blockers and topical corticosteroid was carried out. Avoidance of triggers is recommended. The patient's condition has improved. Both a historical review of mastocytosis and a revised classification, as well as the epidemiology, etiology with triggering factors, clinical presentation, laboratory investigations, and management of urticaria pigmentosa are presented. VL - 7 IS - 1 ER -
Department of Skin and Venereal Diseases, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Department of Internal Medicine, Pharmacology and Clinical Pharmacology, Pediatrics, Epidemiology, Infectious Diseases and Dermatology, Faculty of Medicine, Sofia University, Sofia, Bulgaria
Clinic of Urology, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Department of Anesthesiology and Intensive Care, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria
Department of Infectious Diseases, Parasitology and Dermatovenereology, Medical University, Varna, Bulgaria
Department of Surgical Diseases, Unit of Urology, Medical University, Varna, Bulgaria
Department of Skin and Venereal Diseases, Medical Institute of the Ministry of Internal Affairs, Sofia, Bulgaria

Figure 1. Disseminated livid-brownish macules on the trunk and extremities of the patient.

Figure 2. Sharply demarcated, livid-brownish macules, up to 1.4 cm/d in size, on the trunk of the patient.

Figure 3. Positive Darier’s sign.
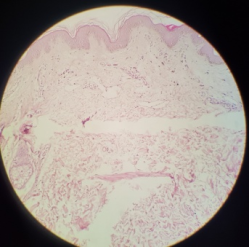
Figure 4. Histopathological examination showed mild superficial and deep perivascular infiltrates (H&E, x 100).
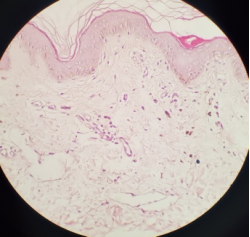
Figure 5. Oval, kidney-shaped mast cells, arranged around the widely dilated venules (H&E, x 200).
Information

