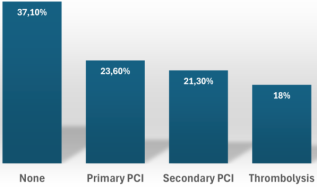
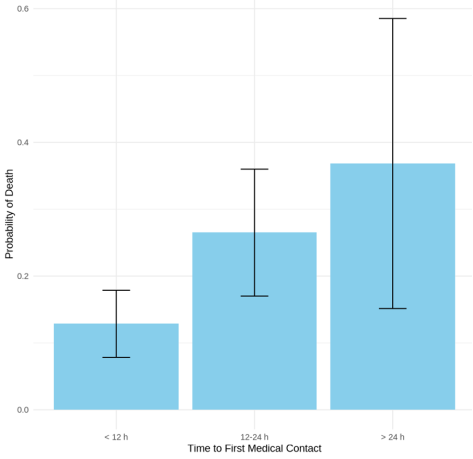
Low-and middle-income countries (LMICs) face many challenges regarding the timely management of STEMI, and the COVID-19 pandemic has impacted our already fragile health systems. The aim of this study was to assess the delays in managing STEMI during COVID-19 and evaluate the 6-month mortality rates related to these delays. A retrospective cross-sectional study was conducted over two years starting from January 2020 at a tertiary center in Dakar, Senegal. All patients referred for STEMI during the study period were included. Statistical analysis was performed using R, version 4.4.0 (R Foundation for Statistical Computing). A total of 273 patients were enrolled during the study period (65.9% males, mean age: 59 ± 12.4). Diabetes Mellitus was present in 37.7% of cases. Only 1 out of 5 patients (20.5%) reached medical attention within 1 hour after symptoms onset, and the time from first medical contact to ECG was < 10 minutes in 39 % of cases. Primary PCI within the first 24 hours was performed in 23.5% of cases. Factors significantly associated with late hospital admission (<12h) were first medical contact < 1h (P 0.0009, OR: 4.06 95% CI; 1.8-9.64), time to first ECG < 10 minutes (P 0.002, OR: 2.79 95% CI; 1.45-5.41) and number of facilities visited < 2 (P 0.004, OR: 3.4 95% CI 1.51-8.22). The 6-month mortality rate was 18.7%, and the probability of death increased with a more significant delay in first medical contact. Our study found persisting delays in STEMI management in Senegal. Establishing a standard of care for STEMI in Senegal is mandatory to overcome healthcare system weaknesses and improve the outcomes of our STEMI patients.
| Published in | International Journal of Cardiovascular and Thoracic Surgery (Volume 10, Issue 3) |
| DOI | 10.11648/j.ijcts.20241003.11 |
| Page(s) | 29-35 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Acute Coronary Syndromes, COVID-19, Management Delays, LMICs
Parameters | Value |
|---|---|
Age (Mean value ± SD) | 59 ± 12.4 |
Male (%) | 65.9 |
Emergency Medical Services awareness (%) | 14 |
Place of living | |
Urban (%) | 93.1 |
Rural (%) | 6.9 |
Work status | |
Self-employed (%) | 62.3 |
Civil servant (%) | 12.8 |
Unemployed (%) | 10.6 |
Cardiovascular risk factors | |
Hypertension (%) | 44 |
Dyslipidemia (%) | 1.8 |
Diabetes mellitus (%) | 37.7 |
Tobacco use (%) | 30.8 |
Sedentary (%) | 70.3 |
Clinical data | |
Typical chest pain (%) | 34.8 |
Shortness of breath | 23.4 |
KILLIP 1 (%) | 91.6 |
KILLIP 2 (%) | 5.9 |
KILLIP 3 (%) | 2.2 |
KILLIP 4 (%) | 0.4 |
Culprit arteries | |
Left anterior Descending Artery (%) | 66.7 |
Right coronary Artery (%) | 39.9 |
Circumflex artery | 33.7 |
Treatment received before referral | |
Thrombolysis (%) | 4 |
Aspirin (%) | 70.3 |
Clopidogrel (%) | 68.9 |
Pain Killer (%) | 52 |
Angiotensin Convertor Inhibitor (%) | 5.5 |
Beta-blockers (%) | 2.6 |
Statins (%) | 12.1 |
Transportation Means | |
Taxi (%) | 81.7 |
Personal car (%) | 17.2 |
Bus (%) | 1.1 |
Time to First Medical Contact | |
< 1 hour (%) | 20.5 |
1-6 hours (%) | 36.2 |
6-12 hours (%) | 5.9 |
12 -24 hours (%) | 30.4 |
>24 hours (%) | 7 |
Time from First Medical Contact to ECG | |
Within 10 mn (%) | 39.0 |
>10 mn (%) | 61.0 |
Type of facilities visited. | |
Health district (%) | 47.6 |
Public hospital (%) | 27.1 |
Private hospital (%) | 18.7 |
Others (%) | 6.6 |
Number of facilities visited before admission | |
< 1 (%) | 72.2 |
>2 (%) | 28.8 |
95% Confidence Interval | ||||
|---|---|---|---|---|
Variables | Estimate | P value | Lower | Higher |
Intercept | 0,09 | <0.0001 | 0,03 | 0,23 |
Time to first ECG < 10 mn | 2,79 | 0,002 | 1,45 | 5,41 |
Number of facilities visited < 2 | 3,4 | 0,004 | 1,51 | 8,22 |
First medical contact < 1h | 4,06 | 0,0009 | 1,8 | 9,64 |
Patient coming from a rural area | 0,65 | 0,18 | 0,34 | 1,23 |
Non-diabetics patients | 1,67 | 0,14 | 0,85 | 3,32 |
ECG | Electrocardiogram |
EMS | Emergency Medical Services |
FMC | First Medical Contact |
LDL Cholesterol | Low Density Level Cholesterol |
LMICs | Low and Middle-Income Countries |
PCI | Percutaneous Coronary Intervention |
STEMI | ST-Elevation Myocardial Infarction |
| [1] | C.-C. F. Tam, C.-W. D. Siu, H. F. Tse, Challenges in Management of ST Elevation Myocardial Infarction during COVID-19 Pandemic, Cardiol Plus 6(2021) 218–230. |
| [2] | G. De Luca, H. Suryapranata, J. P. Ottervanger, E. M. Antman, Time Delay to Treatment and Mortality in Primary Angioplasty for Acute Myocardial Infarction, Circulation 109(2004) 1223–1225. |
| [3] | S. Koul, P. Andell, A. Martinsson, J. Gustav Smith, J. van der Pals, F. Scherstén, T. Jernberg, B. Lagerqvist, D. Erlinge, Delay from first medical contact to primary PCI and all-cause mortality: a nationwide study of patients with ST-elevation myocardial infarction., J Am Heart Assoc 3(2014) e000486. |
| [4] | K. H. Scholz, S. K. G. Maier, L. S. Maier, B. Lengenfelder, C. Jacobshagen, J. Jung, C. Fleischmann, G. S. Werner, H. G. Olbrich, R. Ott, H. Mudra, K. Seidl, P. C. Schulze, C. Weiss, J. Haimerl, T. Friede, T. Meyer, Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial, Eur Heart J 39(2018) 1065. |
| [5] | L. Beza, S. L. Leslie, B. Alemayehu, R. Gary, Acute coronary syndrome treatment delay in low to middle-income countries: A systematic review, Int J Cardiol Heart Vasc 35 (2021). |
| [6] | M. F. Yuyun, K. Sliwa, A. P. Kengne, A. O. Mocumbi, G. Bukhman, Cardiovascular Diseases in Sub-Saharan Africa Compared to High-Income Countries: An Epidemiological Perspective., Glob Heart 15(2020) 15. |
| [7] | A. E. Moran, K. Y. Tzong, M. H. Forouzanfar, G. A. Rothy, G. A. Mensah, M. Ezzati, C. J. L. Murray, M. Naghavi, Variations in ischemic heart disease burden by age, country, and income: the Global Burden of Diseases, Injuries, and Risk Factors 2010 study., Glob Heart 9(2014) 91–9. |
| [8] | B. Seligman, R. Vedanthan, V. Fuster, Acute coronary syndromes in low- and middle-income countries: Moving forward., Int J Cardiol 217 Suppl (2016) S10-2. |
| [9] | M. Kakou-Guikahue, R. N’Guetta, J. B. Anzouan-Kacou, E. Kramoh, R. N’Dori, S. A. Ba, M. Diao, M. Sarr, A. Kane, A. Kane, F. Damorou, D. Balde, M. B. Diarra, M. Djiddou, G. Kimbally-Kaki, P. Zabsonre, I. A. Toure, M. Houénassi, H. Gamra, B. Chajai, B. Gerardin, R. Pillière, P. Aubry, M. C. Iliou, R. Isnard, P. Leprince, Y. Cottin, E. Bertrand, Y. Juillière, J. J. Monsuez, Optimizing the management of acute coronary syndromes in sub-Saharan Africa: A statement from the AFRICARDIO 2015 Consensus Team, Arch Cardiovasc Dis 109(2016) 376–383. |
| [10] | H. Yao, A. Ekou, T. Niamkey, S. H. Gan, I. Kouamé, Y. Afassinou, E. Ehouman, C. Touré, M. Zeller, Y. Cottin, R. N’guetta, Acute Coronary Syndromes in Sub-Saharan Africa: A 10-Year Systematic Review, J Am Heart Assoc 11(2022). |
| [11] | M. Dioum, I. KA, J. Salvador Mingou, P. Nguirane Ndiaye, F. Aw, M. Bamba Ndiaye, S. Antoine Sarr, M. Bodian, A. Alassane Ngaïdé, A. Mbaye, B. Diack, M. Diao, A. Kane, S. Abdou Ba, Care time Delays in Acute Coronary Syndromes with Persistent St Elevation (stem) and the Delaying Factors: Prospective STUDY About 50 Cases in the Cardiology Department of Aristide le Dante Hospital., Cardiology Research and Reports 2(2020) 01–04. |
| [12] | R. Gupta, S. Yusuf, Challenges in management and prevention of ischemic heart disease in low socioeconomic status people in LLMICs., BMC Med 17(2019) 209. |
| [13] | S. Yusuf, S. Rangarajan, K. Teo, S. Islam, W. Li, L. Liu, J. Bo, Q. Lou, F. Lu, T. Liu, L. Yu, S. Zhang, P. Mony, S. Swaminathan, V. Mohan, R. Gupta, R. Kumar, K. Vijayakumar, S. Lear, S. Anand, A. Wielgosz, R. Diaz, A. Avezum, P. Lopez-Jaramillo, F. Lanas, K. Yusoff, N. Ismail, R. Iqbal, O. Rahman, A. Rosengren, A. Yusufali, R. Kelishadi, A. Kruger, T. Puoane, A. Szuba, J. Chifamba, A. Oguz, M. McQueen, M. McKee, G. Dagenais, PURE Investigators, Cardiovascular risk and events in 17 low-, middle-, and high-income countries., N Engl J Med 371(2014) 818–27. |
| [14] | D. K. Moser, L. P. Kimble, M. J. Alberts, A. Alonzo, J. B. Croft, K. Dracup, K. R. Evenson, A. S. Go, M. M. Hand, R. U. Kothari, G. A. Mensah, D. L. Morris, A. M. Pancioli, B. Riegel, J. J. Zerwic, Reducing delay in seeking treatment by patients with acute coronary syndrome and stroke: a scientific statement from the American Heart Association Council on cardiovascular nursing and stroke council., Circulation 114(2006) 168–82. |
| [15] | S. J. Wilson, M. J. Connolly, Z. Elghamry, C. Cosgrove, S. Firoozi, P. Lim, R. Sharma, J. C. Spratt, Effect of the COVID-19 Pandemic on ST-Segment–Elevation Myocardial Infarction Presentations and In-Hospital Outcomes, Circ Cardiovasc Interv 13 (2020). |
| [16] | O. Rodríguez-Leor, B. Cid-Álvarez, A. Pérez de Prado, X. Rossello, S. Ojeda, A. Serrador, R. López-Palop, J. Martín-Moreiras, J. R. Rumoroso, Á. Cequier, B. Ibáñez, I. Cruz-González, R. Romaguera, R. Moreno, M. Villa, R. Ruíz-Salmerón, F. Molano, C. Sánchez, E. Muñoz-García, L. Íñigo, J. Herrador, A. Gómez-Menchero, A. Gómez-Menchero, J. Caballero, S. Ojeda, M. Cárdenas, L. Gheorghe, J. Oneto, F. Morales, F. Valencia, J. R. Ruíz, J. A. Diarte, P. Avanzas, J. Rondán, V. Peral, L. V. Pernasetti, J. Hernández, F. Bosa, P. L. M. Lorenzo, F. Jiménez, J. M. de la T. Hernández, J. Jiménez-Mazuecos, F. Lozano, J. Moreu, E. Novo, J. Robles, J. M. Moreiras, F. Fernández-Vázquez, I. J. Amat-Santos, J. A. Gómez-Hospital, J. García-Picart, B. G. del Blanco, A. Regueiro, X. Carrillo-Suárez, H. Tizón, M. Mohandes, J. Casanova, V. Agudelo-Montañez, J. F. Muñoz, J. Franco, R. del Castillo, P. Salinas, J. Elizaga, F. Sarnago, S. Jiménez-Valero, F. Rivero, J. F. Oteo, E. Alegría-Barrero, Á. Sánchez-Recalde, V. Ruíz, E. Pinar, E. Pinar, A. Planas, B. L. Ledesma, A. Berenguer, A. Fernández-Cisnal, P. Aguar, F. Pomar, M. Jerez, F. Torres, R. García, A. Frutos, J. M. R. Nodar, K. García, R. Sáez, A. Torres, M. Tellería, M. Sadaba, J. R. L. Mínguez, J. C. R. Merchán, J. Portales, R. Trillo, G. Aldama, S. Fernández, M. Santás, M. P. P. Pérez, Impact of COVID-19 on ST-segment elevation myocardial infarction care. The Spanish experience, Revista Española de Cardiología (English Edition) 73(2020) 994–1002. |
| [17] | K. H. Scholz, B. Lengenfelder, C. Thilo, A. Jeron, S. Stefanow, U. Janssens, J. Bauersachs, P. C. Schulze, K. D. Winter, J. Schröder, J. vom Dahl, N. von Beckerath, K. Seidl, T. Friede, T. Meyer, Impact of COVID-19 outbreak on regional STEMI care in Germany, Clinical Research in Cardiology 109(2020) 1511–1521. |
| [18] | U. Primessnig, B. M. Pieske, M. Sherif, Increased mortality and worse cardiac outcome of acute myocardial infarction during the early COVID-19 pandemic, ESC Heart Fail 8(2021) 333–343. |
| [19] | C. S. Kwok, C. P. Gale, T. Kinnaird, N. Curzen, P. Ludman, E. Kontopantelis, J. Wu, T. Denwood, N. Fazal, J. Deanfield, M. A. de Belder, M. Mamas, Impact of COVID-19 on percutaneous coronary intervention for ST-elevation myocardial infarction, Heart 106(2020) 1805–1811. |
| [20] | T. A. Kite, P. F. Ludman, C. P. Gale, J. Wu, A. Caixeta, J. Mansourati, M. Sabate, P. Jimenez-Quevedo, L. Candilio, P. Sadeghipour, A. M. Iniesta, S. P. Hoole, N. Palmer, A. Ariza-Solé, A. Namitokov, H. H. Escutia-Cuevas, F. Vincent, O. Tica, M. Ngunga, I. Meray, A. Morrow, M. M. Arefin, S. Lindsay, G. Kazamel, V. Sharma, A. Saad, G. Sinagra, F. A. Sanchez, M. Roik, S. Savonitto, M. Vavlukis, S. Sangaraju, I. S. Malik, S. Kean, N. Curzen, C. Berry, G. W. Stone, B. J. Gersh, A. H. Gershlick, International Prospective Registry of Acute Coronary Syndromes in Patients With COVID-19, J Am Coll Cardiol 77(2021) 2466–2476. |
| [21] | S. Garcia, L. Stanberry, C. Schmidt, S. Sharkey, M. Megaly, M. S. Albaghdadi, P. M. Meraj, R. Garberich, F. A. Jaffer, A. C. Stefanescu Schmidt, S. R. Dixon, J. J. Rade, T. Smith, M. Tannenbaum, J. Chambers, F. Aguirre, P. P. Huang, D. J. Kumbhani, T. Koshy, D. N. Feldman, J. Giri, P. Kaul, C. Thompson, H. Khalili, B. Maini, K. R. Nayak, M. G. Cohen, S. Bangalore, B. Shah, T. D. Henry, Impact of COVID-19 pandemic on STEMI care: An expanded analysis from the United States, Catheterization and Cardiovascular Interventions 98(2021) 217–222. |
| [22] | S. Garcia, M. S. Albaghdadi, P. M. Meraj, C. Schmidt, R. Garberich, F. A. Jaffer, S. Dixon, J. J. Rade, M. Tannenbaum, J. Chambers, P. P. Huang, T. D. Henry, Reduction in ST-Segment Elevation Cardiac Catheterization Laboratory Activations in the United States During COVID-19 Pandemic, J Am Coll Cardiol 75(2020) 2871–2872. |
| [23] | G. De Luca, M. Verdoia, M. Cercek, L. O. Jensen, M. Vavlukis, L. Calmac, T. Johnson, G. R. Ferrer, V. Ganyukov, W. Wojakowski, T. Kinnaird, C. van Birgelen, Y. Cottin, A. IJsselmuiden, B. Tuccillo, F. Versaci, K.-J. Royaards, J. Ten Berg, M. Laine, M. Dirksen, M. Siviglia, G. Casella, P. Kala, J. L. Díez Gil, A. Banning, V. Becerra, C. De Simone, A. Santucci, X. Carrillo, A. Scoccia, G. Amoroso, A. Lux, T. Kovarnik, P. Davlouros, J. Mehilli, G. Gabrielli, X. F. Rios, N. Bakraceski, S. Levesque, G. Cirrincione, V. Guiducci, M. Kidawa, L. Spedicato, L. Marinucci, P. Ludman, F. Zilio, G. Galasso, E. Fabris, M. Menichelli, A. Garcia-Touchard, S. Manzo, G. Caiazzo, J. Moreu, J. S. Forés, L. Donazzan, L. Vignali, R. Teles, E. Benit, P. Agostoni, F. Bosa Ojeda, H. Lehtola, S. Camacho-Freiere, A. Kraaijeveld, Y. Antti, M. Boccalatte, P. Deharo, I. L. Martínez-Luengas, B. Scheller, D. Alexopoulos, R. Moreno, E. Kedhi, G. Uccello, B. Faurie, A. Gutierrez Barrios, F. S. Di Uccio, B. Wilbert, P. Smits, G. Cortese, G. Parodi, D. Dudek, Impact of COVID-19 Pandemic on Mechanical Reperfusion for Patients With STEMI, J Am Coll Cardiol 76(2020) 2321–2330. |
| [24] | D. Xiang, X. Xiang, W. Zhang, S. Yi, J. Zhang, X. Gu, Y. Xu, K. Huang, X. Su, B. Yu, Y. Wang, W. Fang, Y. Huo, J. Ge, Management and Outcomes of Patients With STEMI During the COVID-19 Pandemic in China, J Am Coll Cardiol 76(2020) 1318–1324. |
| [25] | N. Shrestha, T. Pilgrim, A. Basnet, P. Karki, S. Cook, P. Urban, Percutaneous coronary intervention for acute coronary syndromes in eastern Nepal: a preliminary report, Swiss Med Wkly (2013). |
| [26] | D. Xavier, P. Pais, P. J. Devereaux, C. Xie, D. Prabhakaran, K. S. Reddy, R. Gupta, P. Joshi, P. Kerkar, S. Thanikachalam, K. K. Haridas, T. M. Jaison, S. Naik, A. K. Maity, S. Yusuf, CREATE registry investigators, Treatment and outcomes of acute coronary syndromes in India (CREATE): a prospective analysis of registry data., Lancet 371(2008) 1435–42. |
| [27] | D.-Y. Kim, Z. Wala, S. Islam, R. Islam, M. Ahn, Clinical characteristics and outcomes of ST-segment elevation myocardial infarction in a low income setting in rural Bangladesh., Int J Cardiol Heart Vasc 23(2019) 100376. |
| [28] | A. Medagama, R. Bandara, C. De Silva, M. P. Galgomuwa, Management of acute coronary syndromes in a developing country; time for a paradigm shift? an observational study., BMC Cardiovasc Disord 15(2015) 133. |
APA Style
Gaye, N. D., Ngaide, A. A., Mingou, J. S., Ngningue, A., Ndiaye, M. B., et al. (2024). Management Delays and Outcomes in ST-Elevation Myocardial Infarction (STEMI) in the COVID-19 Era in Senegal: Insights from a Tertiary Center. International Journal of Cardiovascular and Thoracic Surgery, 10(3), 29-35. https://doi.org/10.11648/j.ijcts.20241003.11
ACS Style
Gaye, N. D.; Ngaide, A. A.; Mingou, J. S.; Ngningue, A.; Ndiaye, M. B., et al. Management Delays and Outcomes in ST-Elevation Myocardial Infarction (STEMI) in the COVID-19 Era in Senegal: Insights from a Tertiary Center. Int. J. Cardiovasc. Thorac. Surg. 2024, 10(3), 29-35. doi: 10.11648/j.ijcts.20241003.11
AMA Style
Gaye ND, Ngaide AA, Mingou JS, Ngningue A, Ndiaye MB, et al. Management Delays and Outcomes in ST-Elevation Myocardial Infarction (STEMI) in the COVID-19 Era in Senegal: Insights from a Tertiary Center. Int J Cardiovasc Thorac Surg. 2024;10(3):29-35. doi: 10.11648/j.ijcts.20241003.11
@article{10.11648/j.ijcts.20241003.11,
author = {Ngone Diaba Gaye and Aliou Alassane Ngaide and Joseph Salvador Mingou and Ameth Ngningue and Mouhamadou Bamba Ndiaye and Alassane Mbaye and Abdoul Kane},
title = {Management Delays and Outcomes in ST-Elevation Myocardial Infarction (STEMI) in the COVID-19 Era in Senegal: Insights from a Tertiary Center
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {10},
number = {3},
pages = {29-35},
doi = {10.11648/j.ijcts.20241003.11},
url = {https://doi.org/10.11648/j.ijcts.20241003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20241003.11},
abstract = {Low-and middle-income countries (LMICs) face many challenges regarding the timely management of STEMI, and the COVID-19 pandemic has impacted our already fragile health systems. The aim of this study was to assess the delays in managing STEMI during COVID-19 and evaluate the 6-month mortality rates related to these delays. A retrospective cross-sectional study was conducted over two years starting from January 2020 at a tertiary center in Dakar, Senegal. All patients referred for STEMI during the study period were included. Statistical analysis was performed using R, version 4.4.0 (R Foundation for Statistical Computing). A total of 273 patients were enrolled during the study period (65.9% males, mean age: 59 ± 12.4). Diabetes Mellitus was present in 37.7% of cases. Only 1 out of 5 patients (20.5%) reached medical attention within 1 hour after symptoms onset, and the time from first medical contact to ECG was < 10 minutes in 39 % of cases. Primary PCI within the first 24 hours was performed in 23.5% of cases. Factors significantly associated with late hospital admission (<12h) were first medical contact < 1h (P 0.0009, OR: 4.06 95% CI; 1.8-9.64), time to first ECG < 10 minutes (P 0.002, OR: 2.79 95% CI; 1.45-5.41) and number of facilities visited < 2 (P 0.004, OR: 3.4 95% CI 1.51-8.22). The 6-month mortality rate was 18.7%, and the probability of death increased with a more significant delay in first medical contact. Our study found persisting delays in STEMI management in Senegal. Establishing a standard of care for STEMI in Senegal is mandatory to overcome healthcare system weaknesses and improve the outcomes of our STEMI patients.
},
year = {2024}
}
TY - JOUR T1 - Management Delays and Outcomes in ST-Elevation Myocardial Infarction (STEMI) in the COVID-19 Era in Senegal: Insights from a Tertiary Center AU - Ngone Diaba Gaye AU - Aliou Alassane Ngaide AU - Joseph Salvador Mingou AU - Ameth Ngningue AU - Mouhamadou Bamba Ndiaye AU - Alassane Mbaye AU - Abdoul Kane Y1 - 2024/09/11 PY - 2024 N1 - https://doi.org/10.11648/j.ijcts.20241003.11 DO - 10.11648/j.ijcts.20241003.11 T2 - International Journal of Cardiovascular and Thoracic Surgery JF - International Journal of Cardiovascular and Thoracic Surgery JO - International Journal of Cardiovascular and Thoracic Surgery SP - 29 EP - 35 PB - Science Publishing Group SN - 2575-4882 UR - https://doi.org/10.11648/j.ijcts.20241003.11 AB - Low-and middle-income countries (LMICs) face many challenges regarding the timely management of STEMI, and the COVID-19 pandemic has impacted our already fragile health systems. The aim of this study was to assess the delays in managing STEMI during COVID-19 and evaluate the 6-month mortality rates related to these delays. A retrospective cross-sectional study was conducted over two years starting from January 2020 at a tertiary center in Dakar, Senegal. All patients referred for STEMI during the study period were included. Statistical analysis was performed using R, version 4.4.0 (R Foundation for Statistical Computing). A total of 273 patients were enrolled during the study period (65.9% males, mean age: 59 ± 12.4). Diabetes Mellitus was present in 37.7% of cases. Only 1 out of 5 patients (20.5%) reached medical attention within 1 hour after symptoms onset, and the time from first medical contact to ECG was < 10 minutes in 39 % of cases. Primary PCI within the first 24 hours was performed in 23.5% of cases. Factors significantly associated with late hospital admission (<12h) were first medical contact < 1h (P 0.0009, OR: 4.06 95% CI; 1.8-9.64), time to first ECG < 10 minutes (P 0.002, OR: 2.79 95% CI; 1.45-5.41) and number of facilities visited < 2 (P 0.004, OR: 3.4 95% CI 1.51-8.22). The 6-month mortality rate was 18.7%, and the probability of death increased with a more significant delay in first medical contact. Our study found persisting delays in STEMI management in Senegal. Establishing a standard of care for STEMI in Senegal is mandatory to overcome healthcare system weaknesses and improve the outcomes of our STEMI patients. VL - 10 IS - 3 ER -
Department of Cardiovascular Rehabilitation, Ibra Mamadou Wane Medical Center, Dakar, Senegal; School of Medicine, Cheikh Anta Diop University, Dakar, Senegal
School of Medicine, Cheikh Anta Diop University, Dakar, Senegal; Department of Cardiology, Dalal Jam Hospital, Guediawaye, Senegal
School of Medicine, Cheikh Anta Diop University, Dakar, Senegal; Department of Cardiology, Dalal Jam Hospital, Guediawaye, Senegal
School of Medicine, Cheikh Anta Diop University, Dakar, Senegal
School of Medicine, Cheikh Anta Diop University, Dakar, Senegal
School of Medicine, Cheikh Anta Diop University, Dakar, Senegal; Department of Cardiology, Idrissa Pouye General Hospital, Dakar, Senegal
School of Medicine, Cheikh Anta Diop University, Dakar, Senegal; Department of Cardiology, Dalal Jam Hospital, Guediawaye, Senegal
Information