Background: Scrotal trauma represents a rare but serious urological emergency with potential consequences on fertility, endocrine function, and overall quality of life. Atypical cases such as self-mutilation, human bites, animal horn injuries, or war-related wounds pose significant diagnostic and therapeutic challenges. Methods: We report four unusual cases of scrotal trauma managed in a university teaching hospital. Clinical, surgical, therapeutic, and follow-up data were retrospectively analyzed. A targeted literature review was conducted to support the discussion on multidisciplinary management strategies. Results: The first case involved bilateral testicular self-amputation in a patient with paranoid schizophrenia, treated with surgical debridement, hemostatic ligation, testosterone replacement therapy, and psychiatric follow-up. The second case described a bull horn injury in a teenage cattle breeder, presenting with grade III left scrotal trauma (AAST), managed surgically. The third case involved bilateral scrotal human bite injuries sustained during a school altercation, treated with wound closure, antibiotic prophylaxis, serological monitoring, and medico-legal documentation. The fourth case concerned a soldier injured by an improvised explosive device (IED), presenting with extensive penoscrotal tissue loss and left testicular destruction, managed by damage control surgery and followed by andrological, orthopedic, and psychological care. Conclusion: Atypical scrotal trauma requires prompt, individualized, and multidisciplinary diagnostic and therapeutic approaches. Early surgical exploration, tailored psychological support, and specific risk prevention measures are essential to optimize both functional and psychosexual outcomes in these patients.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Scrotal trauma is rare but can severely compromise endocrine function, fertility, and bodily integrity. It typically occurs in sports or accidental contexts
[1]
European Association of Urology. EAU Guidelines on Urological Trauma. 2025. Available from:
. However, certain unusual circumstances-such as human bites, self-inflicted injuries, or war-related wounds-challenge conventional protocols and demand urgent, multidisciplinary, and individualized management.
We report four atypical cases of scrotal trauma occurring under unique circumstances: a bull horn injury during cattle feeding, a human bite sustained during a school altercation, self-mutilation in a patient with schizophrenia, and complex scrotal injuries caused by an improvised explosive device (IED) during counterterrorism operations.
These atypical scenarios highlight a wide range of concerns, including life-threatening emergencies, infectious risks, underlying psychiatric conditions, medico-legal and psychosocial implications, and the need for hormonal replacement therapy or reconstructive surgery.
2. Methods
We report four unusual cases of scrotal trauma managed in a university teaching hospital. Clinical, surgical, therapeutic, and follow-up data were retrospectively analyzed. A targeted literature review was conducted to support the discussion on multidisciplinary management strategies.
3. Case Presentations
3.1. Case 1: Scrotal Self-mutilation in a Patient with Schizophrenia
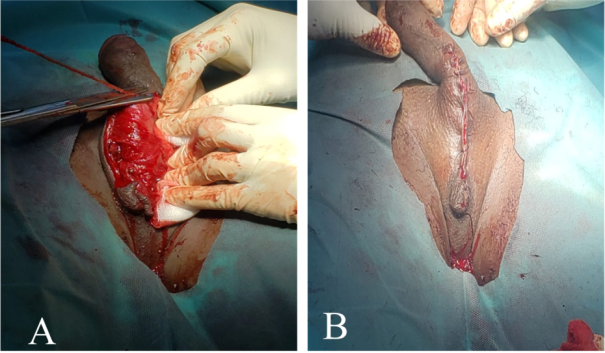
Figure 1. Genital self-mutilation with complete emasculation in a patient with schizophrenia. A) Initial presentation; B) Postoperative appearance.
Mr. Z. O., a 29-year-old male with a history of mental illness reported by relatives, was admitted to the urology emergency department following genital self-mutilation using a razor blade approximately 3 hours prior. General examination revealed psychomotor agitation, hemorrhagic shock with hypotension (BP 80/50 mmHg), tachycardia (110 bpm), and tachypnea (24 breaths/min). Immediate hemodynamic resuscitation was initiated in the operating room, stabilizing vital signs. Physical examination showed complete bilateral testicular amputation at the spermatic cords, with hemorrhagic and soil-contaminated wound edges (Figure 1). Copious irrigation with isotonic saline was performed, followed by ligation of the spermatic cords, wound debridement, and skin closure. Psychiatric evaluation confirmed paranoid schizophrenia; neuroleptic therapy and regular psychiatric follow-up were started. Antibiotic prophylaxis with amoxicillin-clavulanic acid was administered, along with testosterone enanthate substitution (250 mg IM every three weeks). Tetanus immunization was updated. The patient was followed up at 3 and 6 months without complaints or recurrence.
3.2. Case 2: Scrotal Trauma by Bovine Goring
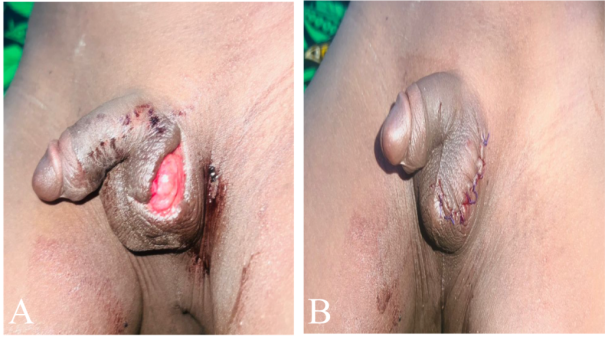
O. Z., a 14-year-old adolescent cattle breeder with no prior medical history, presented to the urology emergency unit with left scrotal trauma sustained while feeding his ox. He suffered a direct horn impact to the left scrotum, without loss of consciousness or associated injuries. General status was World Health Organization (WHO) stage 1 with stable hemodynamics. Physical exam revealed an American Association for the Surgery of Trauma (AAST) grade III scrotal wound with visible disruption of the left tunica vaginalis but no testicular extrusion, local edema, moderate pain, and no active bleeding (Figure 2). Under spinal anesthesia, surgical exploration and debridement were performed. Left tunica vaginalis lesions with hemorrhagic edges were confirmed; testis and adnexa were intact without hematoma. Right hemiscrotum was normal. Management included thorough saline irrigation, surgical debridement, closure of tunica vaginalis, dressing, oral antibiotic prophylaxis (amoxicillin-clavulanic acid 1 g twice daily for 7 days), and analgesia with paracetamol. Tetanus vaccination was updated and antitetanus serum administered. Postoperative recovery was uneventful. Follow-up at days 3 and 7 showed no infection; wound healing was satisfactory. At 1 and 6 months, no functional or cosmetic sequelae were noted.
Figure 2. Left scrotal bull horn injury in a teenage cattle breeder. A) Initial presentation; B) Postoperative appearance.
3.3. Case 3: Human Scrotal Bite During School Altercation
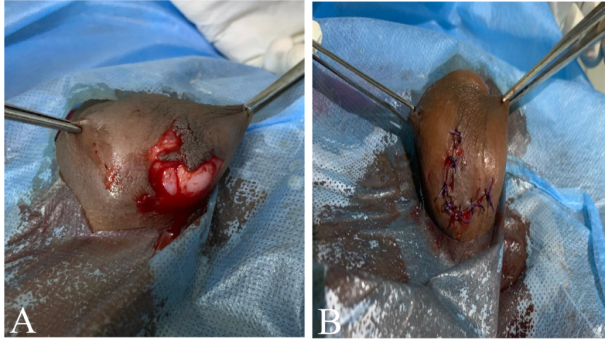
A. S., a 13-year-old adolescent, was brought to the urology emergency by his parents after sustaining bilateral scrotal injuries from a human bite during a school fight. On admission, he was conscious and hemodynamically stable. Vaccinations were up to date, including tetanus and hepatitis B. Physical examination revealed a V-shaped wound involving both hemiscrota down to the exposed tunica vaginalis (Figure 3). Immediate serologies for HIV, HBs antigen, and HCV antibodies were performed on both victim and aggressor with parental consent; all results were negative. Surgical exploration revealed intact testicles and spermatic cords without hematoma. Debridement and closure of the tunica vaginalis were performed. Antibiotic prophylaxis with amoxicillin-clavulanic acid was prescribed. A medical certificate was issued, and the school administration informed. Psychological support was provided. Scheduled serological follow-up at 6 weeks, 3 months, and 6 months remained negative. Wound healing progressed satisfactoril.
Figure 3. Human bite injury exposing both tunica vaginalis layers. A) Initial presentation; B) Postoperative appearance.
3.4. Case 4: Scrotal Trauma Due to Improvised Explosive Device (IED)
Mr. J. P., a 27-year-old soldier, was brought by ambulance to the emergency department 2 hours after an IED explosion during an anti-terrorism patrol. He was conscious and hemodynamically stable on admission. Micturition was normal with no hematuria or urethrorrhagia. Examination revealed extensive soft tissue destruction of the external genitalia, involving the penis, scrotum, and perineum. There was left testicular disintegration and right tunica albuginea injury with hemorrhagic edges (Figure 4). Moderate suprapubic tenderness prompted thoraco-abdominopelvic CT scan, which showed pubic symphysis diastasis without pelvic instability. Conservative orthopedic management with close clinical monitoring was chosen. In the operating room, left spermatic cord ligation and left orchiectomy were performed, along with extensive debridement, irrigation with saline, and right tunica albuginea repair. Orthopedic consultation recommended conservative treatment with clinical and radiological follow-up. Antibiotic prophylaxis with amoxicillin-clavulanic acid and tetanus immunization were administered. Planned future interventions include scrotal reconstruction and penile skin grafting based on healing. Andrological follow-up will assess residual testicular function and fertility potential. Specialized post-traumatic psychological care was initiated.
Figure 4. Severe penoscrotal degloving following improvised explosive device (IED) injury in a deployed soldier. A) Immediate aspect after debridement and primary closure; B) Healing phase aspect.
Antibiotics, HIV-HBV-HCV testing for both children, psychological support
Negative serologies at 6 weeks, 3 and 6 months. Good outcome
4: IED explosion
27 years old, military personnel, on duty
Improvised explosive device blast
Extensive genital/perineal injury, left testicular disintegration, right tunica albuginea lesion
Left orchidectomy, right tunica suture, debridement
IV antibiotics, tetanus prophylaxis, orthopedic, psychological and andrological follow-up
Scrotal reconstruction and skin graft planned. Ongoing follow-up
4. Discussion
Scrotal trauma, although infrequent in routine urological practice, represents a major medico-surgical emergency due to its potentially severe functional, aesthetic, and psychological consequences. Management relies on rapid diagnosis, thorough lesion assessment, and often urgent surgical exploration, in accordance with the latest guidelines of the European Association of Urology (EAU, 2025)
[1]
European Association of Urology. EAU Guidelines on Urological Trauma. 2025. Available from:
. The four cases presented in this series highlight atypical mechanisms rarely described in the literature, each raising specific clinical challenges that require a personalized and multidisciplinary approach.
Genital self-mutilation, as illustrated here in a schizophrenic patient, is an exceptionally rare and dramatic situation. Several authors have emphasized its scarcity in the literature
[2]
Moufid K, Joual A, Debbagh A, Bennani S, Mrini ME. Genital self-mutilation: about 3 cases. Prog Urol. 2004.
[3]
Sarr A, Sow Y, Ndiaye B, Koldimadji M, Ouedraogo B, Diao B, et al. Male genital self-mutilation: about two cases. Sexologies. 2015 Apr; 24(2): 65‑8. Available from:
. These cases constitute simultaneous urological and psychiatric emergencies. The study by Adli et al.
[4]
Adli G, Rahman IA, Djatisoesanto W. Male genital trauma caused by self-mutilation: A first case series report in Indonesia. Int J Surg Case Rep. 2023 May; 106: 108196.
confirms that genital self-mutilation demands a holistic medico-psychiatric response. Accurate psychiatric diagnosis and rigorous follow-up are essential to optimize functional outcomes and prevent recurrences. The literature stresses the importance of rapid hemorrhage control, prophylactic infection treatment, and hormonal replacement therapy (HRT) in cases of complete castration. Williams et al. (2015)
[5]
Williams M, Rosner I, Chen Y, Cullen J, Jezior J, Dean R. Testosterone recovery after polytrauma and scrotal injury in patients from Operation Enduring Freedom and Operation Iraqi Freedom. J Urol. 2015 Feb; 193(2): 618‑22. Available from: http://www.jurology.com/doi/10.1016/j.juro.2014.08.105
[5]
provided valuable data guiding HRT after severe scrotal trauma, showing that natural testosterone recovery may occur in some patients after an average delay of 4.5 months post-trauma, but HRT remains mandatory in cases of major testicular injury, bilateral orchiectomy, or slow recovery velocity (< 4 ng/dL/day).
Trauma caused by bovine goring is poorly documented, particularly regarding external genitalia. Literature primarily reports animal bites such as those from dogs or donkeys, sometimes requiring reconstructive surgery or penile glans amputation
[6]
Boughaleb A, Tariqi R, El Boté H. An unusual etiology of testicular avulsion: A case report. Int J Surg Case Rep. 2024 Aug; 121: 109942.
Ouattara A, Yaméogo C, Paré AK, Kaboré AF, Ky D, Kabré B, et al. Domestic donkey bite of genitalia: an unusual etiology of penile glans amputation in Burkina Faso (case report and literature review). Pan Afr Med J. 2020 May 12; 36.
. Though rarely reported, goring injuries may be more dangerous due to the kinetic energy of the impact. They are more frequently described at the thoracoabdominal level, with scrotal involvement being exceptional
[8]
Martínez Hernández A, Martínez Ramos D, García Moreno MV, Abdlekader Mohamed N, López Loscos E, Aliaga Hilario E, et al. Bull horn injuries: a 40-year retrospective study with 572 patients. Am J Surg. 2021 Aug; 222(2): 446‑52. Available from:
. Cattle horns can cause penetrating, contaminated wounds with a high risk of infection. Goring injuries require special attention as they can cause complex internal lesions that may be initially inapparent. Management mandates systematic surgical exploration even if the initial clinical exam seems reassuring to assess the integrity of the testis, epididymis, and spermatic cord
[9]
Morey AF, Metro MJ, Carney KJ, Miller KS, McAninch JW. Consensus on genitourinary trauma: external genitalia. BJU Int. 2004 Sep; 94(4): 507‑15.
. Most cattle-related injuries occur during direct handling without protective measures. Effective prevention relies on educating farmers about risks, designing secured enclosures with protective barriers, and organizing feeding areas to reduce direct contact with animals.
In the pediatric context, human scrotal bite injuries are rare but carry a high infectious risk. The polymicrobial flora of the human oral cavity- including Streptococcus spp., Staphylococcus aureus, Eikenella corrodens, and various strict anaerobes-makes inoculation particularly hazardous
[10]
Brook I. Microbiology and management of human and animal bite wound infections. Prim Care Clin Off Pract. 2003 Mar; 30(1): 25‑39. Available from:
. Beyond local wound management and systematic antibiotic prophylaxis, rigorous infectious status evaluation of both victim and aggressor is mandatory. Post-exposure prophylaxis (PEP) for HIV and vaccination or immunoglobulin administration against hepatitis B may be required based on serological status, according to the EAU 2025 guidelines
[1]
European Association of Urology. EAU Guidelines on Urological Trauma. 2025. Available from:
. Per 2024 WHO and CDC updates, in cases of positive or unknown HIV status with significant exposure, PEP must be initiated within 72 hours and consist of a 28-day triple antiretroviral regimen
[11]
World Health Organization. Guidelines for HIV post-exposure prophylaxis. Available from:
. If the aggressor carries hepatitis B surface antigen and the victim is inadequately immunized, combined immunoglobulin and vaccination are indicated. Conversely, if tests are negative and the victim fully vaccinated, serological monitoring at 6 weeks, 3 months, and 6 months is recommended. The medico-legal implications require issuance of a detailed medical certificate at admission.
War-related genital trauma, especially from improvised explosive devices (IEDs), is frequent in military settings
[12]
Hudak SJ, Hakim S. Operative management of wartime genitourinary injuries at Balad Air Force Theater Hospital, 2005 to 2008. J Urol. 2009 Jul; 182(1): 180‑3.
[12]
, often associated with complex pelvic injuries. These injuries involve extensive tissue destruction, major infection risk, and associated orthopedic lesions. The EAU recommends surgical exploration, wound irrigation, orchidectomy if indicated, and planning for delayed reconstruction
[1]
European Association of Urology. EAU Guidelines on Urological Trauma. 2025. Available from:
. This tactical approach prioritizes life-saving emergency hemostasis and delayed reconstruction in sequential stages to maximize survival. Andrological and psychological follow-up is crucial to minimize long-term functional and psychosexual sequelae.
5. Conclusion
Atypical scrotal traumas represent urgent medico-surgical conditions with significant functional, aesthetic, and psychological implications. This case series highlights the diversity of injury mechanisms, ranging from self-mutilation and war-related trauma to animal and human assaults. Prompt, multidisciplinary, and individualized management is essential to preserve urogenital and psychosexual prognosis. Surgical exploration often remains indispensable, even in the absence of obvious testicular rupture. Psychological support and andrological rehabilitation should systematically be included in the patient’s follow-up.
Moufid K, Joual A, Debbagh A, Bennani S, Mrini ME. Genital self-mutilation: about 3 cases. Prog Urol. 2004.
[3]
Sarr A, Sow Y, Ndiaye B, Koldimadji M, Ouedraogo B, Diao B, et al. Male genital self-mutilation: about two cases. Sexologies. 2015 Apr; 24(2): 65‑8. Available from:
Adli G, Rahman IA, Djatisoesanto W. Male genital trauma caused by self-mutilation: A first case series report in Indonesia. Int J Surg Case Rep. 2023 May; 106: 108196.
Williams M, Rosner I, Chen Y, Cullen J, Jezior J, Dean R. Testosterone recovery after polytrauma and scrotal injury in patients from Operation Enduring Freedom and Operation Iraqi Freedom. J Urol. 2015 Feb; 193(2): 618‑22. Available from: http://www.jurology.com/doi/10.1016/j.juro.2014.08.105
[6]
Boughaleb A, Tariqi R, El Boté H. An unusual etiology of testicular avulsion: A case report. Int J Surg Case Rep. 2024 Aug; 121: 109942.
Ouattara A, Yaméogo C, Paré AK, Kaboré AF, Ky D, Kabré B, et al. Domestic donkey bite of genitalia: an unusual etiology of penile glans amputation in Burkina Faso (case report and literature review). Pan Afr Med J. 2020 May 12; 36.
Martínez Hernández A, Martínez Ramos D, García Moreno MV, Abdlekader Mohamed N, López Loscos E, Aliaga Hilario E, et al. Bull horn injuries: a 40-year retrospective study with 572 patients. Am J Surg. 2021 Aug; 222(2): 446‑52. Available from:
Hudak SJ, Hakim S. Operative management of wartime genitourinary injuries at Balad Air Force Theater Hospital, 2005 to 2008. J Urol. 2009 Jul; 182(1): 180‑3.
[13]
Blackbourne LH. Combat damage control surgery. Crit Care Med. 2008 Jul; 36(Suppl): S304‑10. Available from:
Sawadogo, H., Yameogo, C. A. M. K. D., Kirakoya, B., Ouedraogo, S., Pare, A., et al. (2025). Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature. International Journal of Clinical Urology, 9(2), 130-136. https://doi.org/10.11648/j.ijcu.20250902.14
Sawadogo, H.; Yameogo, C. A. M. K. D.; Kirakoya, B.; Ouedraogo, S.; Pare, A., et al. Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature. Int. J. Clin. Urol.2025, 9(2), 130-136. doi: 10.11648/j.ijcu.20250902.14
Sawadogo H, Yameogo CAMKD, Kirakoya B, Ouedraogo S, Pare A, et al. Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature. Int J Clin Urol. 2025;9(2):130-136. doi: 10.11648/j.ijcu.20250902.14
@article{10.11648/j.ijcu.20250902.14,
author = {Hassami Sawadogo and Clotaire Alexis Marie Kiemdiba Donega Yameogo and Brahima Kirakoya and Salif Ouedraogo and Abdoul-Karim Pare and Adama Ouattara},
title = {Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {130-136},
doi = {10.11648/j.ijcu.20250902.14},
url = {https://doi.org/10.11648/j.ijcu.20250902.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.14},
abstract = {Background: Scrotal trauma represents a rare but serious urological emergency with potential consequences on fertility, endocrine function, and overall quality of life. Atypical cases such as self-mutilation, human bites, animal horn injuries, or war-related wounds pose significant diagnostic and therapeutic challenges. Methods: We report four unusual cases of scrotal trauma managed in a university teaching hospital. Clinical, surgical, therapeutic, and follow-up data were retrospectively analyzed. A targeted literature review was conducted to support the discussion on multidisciplinary management strategies. Results: The first case involved bilateral testicular self-amputation in a patient with paranoid schizophrenia, treated with surgical debridement, hemostatic ligation, testosterone replacement therapy, and psychiatric follow-up. The second case described a bull horn injury in a teenage cattle breeder, presenting with grade III left scrotal trauma (AAST), managed surgically. The third case involved bilateral scrotal human bite injuries sustained during a school altercation, treated with wound closure, antibiotic prophylaxis, serological monitoring, and medico-legal documentation. The fourth case concerned a soldier injured by an improvised explosive device (IED), presenting with extensive penoscrotal tissue loss and left testicular destruction, managed by damage control surgery and followed by andrological, orthopedic, and psychological care. Conclusion: Atypical scrotal trauma requires prompt, individualized, and multidisciplinary diagnostic and therapeutic approaches. Early surgical exploration, tailored psychological support, and specific risk prevention measures are essential to optimize both functional and psychosexual outcomes in these patients.
},
year = {2025}
}
TY - JOUR
T1 - Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature
AU - Hassami Sawadogo
AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo
AU - Brahima Kirakoya
AU - Salif Ouedraogo
AU - Abdoul-Karim Pare
AU - Adama Ouattara
Y1 - 2025/09/25
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250902.14
DO - 10.11648/j.ijcu.20250902.14
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 130
EP - 136
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250902.14
AB - Background: Scrotal trauma represents a rare but serious urological emergency with potential consequences on fertility, endocrine function, and overall quality of life. Atypical cases such as self-mutilation, human bites, animal horn injuries, or war-related wounds pose significant diagnostic and therapeutic challenges. Methods: We report four unusual cases of scrotal trauma managed in a university teaching hospital. Clinical, surgical, therapeutic, and follow-up data were retrospectively analyzed. A targeted literature review was conducted to support the discussion on multidisciplinary management strategies. Results: The first case involved bilateral testicular self-amputation in a patient with paranoid schizophrenia, treated with surgical debridement, hemostatic ligation, testosterone replacement therapy, and psychiatric follow-up. The second case described a bull horn injury in a teenage cattle breeder, presenting with grade III left scrotal trauma (AAST), managed surgically. The third case involved bilateral scrotal human bite injuries sustained during a school altercation, treated with wound closure, antibiotic prophylaxis, serological monitoring, and medico-legal documentation. The fourth case concerned a soldier injured by an improvised explosive device (IED), presenting with extensive penoscrotal tissue loss and left testicular destruction, managed by damage control surgery and followed by andrological, orthopedic, and psychological care. Conclusion: Atypical scrotal trauma requires prompt, individualized, and multidisciplinary diagnostic and therapeutic approaches. Early surgical exploration, tailored psychological support, and specific risk prevention measures are essential to optimize both functional and psychosexual outcomes in these patients.
VL - 9
IS - 2
ER -
Sawadogo, H., Yameogo, C. A. M. K. D., Kirakoya, B., Ouedraogo, S., Pare, A., et al. (2025). Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature. International Journal of Clinical Urology, 9(2), 130-136. https://doi.org/10.11648/j.ijcu.20250902.14
Sawadogo, H.; Yameogo, C. A. M. K. D.; Kirakoya, B.; Ouedraogo, S.; Pare, A., et al. Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature. Int. J. Clin. Urol.2025, 9(2), 130-136. doi: 10.11648/j.ijcu.20250902.14
Sawadogo H, Yameogo CAMKD, Kirakoya B, Ouedraogo S, Pare A, et al. Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature. Int J Clin Urol. 2025;9(2):130-136. doi: 10.11648/j.ijcu.20250902.14
@article{10.11648/j.ijcu.20250902.14,
author = {Hassami Sawadogo and Clotaire Alexis Marie Kiemdiba Donega Yameogo and Brahima Kirakoya and Salif Ouedraogo and Abdoul-Karim Pare and Adama Ouattara},
title = {Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {130-136},
doi = {10.11648/j.ijcu.20250902.14},
url = {https://doi.org/10.11648/j.ijcu.20250902.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.14},
abstract = {Background: Scrotal trauma represents a rare but serious urological emergency with potential consequences on fertility, endocrine function, and overall quality of life. Atypical cases such as self-mutilation, human bites, animal horn injuries, or war-related wounds pose significant diagnostic and therapeutic challenges. Methods: We report four unusual cases of scrotal trauma managed in a university teaching hospital. Clinical, surgical, therapeutic, and follow-up data were retrospectively analyzed. A targeted literature review was conducted to support the discussion on multidisciplinary management strategies. Results: The first case involved bilateral testicular self-amputation in a patient with paranoid schizophrenia, treated with surgical debridement, hemostatic ligation, testosterone replacement therapy, and psychiatric follow-up. The second case described a bull horn injury in a teenage cattle breeder, presenting with grade III left scrotal trauma (AAST), managed surgically. The third case involved bilateral scrotal human bite injuries sustained during a school altercation, treated with wound closure, antibiotic prophylaxis, serological monitoring, and medico-legal documentation. The fourth case concerned a soldier injured by an improvised explosive device (IED), presenting with extensive penoscrotal tissue loss and left testicular destruction, managed by damage control surgery and followed by andrological, orthopedic, and psychological care. Conclusion: Atypical scrotal trauma requires prompt, individualized, and multidisciplinary diagnostic and therapeutic approaches. Early surgical exploration, tailored psychological support, and specific risk prevention measures are essential to optimize both functional and psychosexual outcomes in these patients.
},
year = {2025}
}
TY - JOUR
T1 - Uncommon Scrotal Trauma: Insights from Four Distinct Cases and Review of the Literature
AU - Hassami Sawadogo
AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo
AU - Brahima Kirakoya
AU - Salif Ouedraogo
AU - Abdoul-Karim Pare
AU - Adama Ouattara
Y1 - 2025/09/25
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250902.14
DO - 10.11648/j.ijcu.20250902.14
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 130
EP - 136
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250902.14
AB - Background: Scrotal trauma represents a rare but serious urological emergency with potential consequences on fertility, endocrine function, and overall quality of life. Atypical cases such as self-mutilation, human bites, animal horn injuries, or war-related wounds pose significant diagnostic and therapeutic challenges. Methods: We report four unusual cases of scrotal trauma managed in a university teaching hospital. Clinical, surgical, therapeutic, and follow-up data were retrospectively analyzed. A targeted literature review was conducted to support the discussion on multidisciplinary management strategies. Results: The first case involved bilateral testicular self-amputation in a patient with paranoid schizophrenia, treated with surgical debridement, hemostatic ligation, testosterone replacement therapy, and psychiatric follow-up. The second case described a bull horn injury in a teenage cattle breeder, presenting with grade III left scrotal trauma (AAST), managed surgically. The third case involved bilateral scrotal human bite injuries sustained during a school altercation, treated with wound closure, antibiotic prophylaxis, serological monitoring, and medico-legal documentation. The fourth case concerned a soldier injured by an improvised explosive device (IED), presenting with extensive penoscrotal tissue loss and left testicular destruction, managed by damage control surgery and followed by andrological, orthopedic, and psychological care. Conclusion: Atypical scrotal trauma requires prompt, individualized, and multidisciplinary diagnostic and therapeutic approaches. Early surgical exploration, tailored psychological support, and specific risk prevention measures are essential to optimize both functional and psychosexual outcomes in these patients.
VL - 9
IS - 2
ER -