Objective: To evaluate the outcome of pregnancy in patients who developed chikungunya infection during the antenatal period and to evaluate the severity of chikungunya infection in pregnant women. Material and methodology - This retrospective, record-based, observational study recruited, a total of 47 antenatal women who were admitted to the Obst & gynae department in Lady Harding Medical College, hospital and tested chikungunya IgM Antibody positive during the chikungunya outbreak from September 2016 to September 2017 and an equal number of women with fever, but without chikungunya (IgM negative) who were admitted during the same period comparable in age and parity, were taken as a control group. The details of the admitted antenatal women were taken from the medical record section. ELISA IgM was taken as a positive case. The records included a detailed history, examination, investigations, delivery details, and maternal and perinatal outcomes. The pregnancy and neonatal outcomes were compared between pregnant women with fever, with Chikungunya IgM positive and negative. All the data was compiled in a Microsoft Excel sheet using the latest SPSS version. Result- In this study, 356 pregnant women with fever during the study period who were hospitalized were enrolled out of whom 47 had chikungunya IgM positive (13.2%). Out of 309 Chikungunya IgM-negative pregnant women (86.79%), 47 patients were randomly selected as a control group. Out of these 47 patients, one patient required intensive care unit (ICU) and later succumbed, whereas none were transferred to the ICU in the control group. One case of vertical transmission was reported amongst positive neonates. We found that overall chikungunya infection in pregnancy was not significantly associated with any adverse outcomes as compared to controls. However, admission to the Intensive Care Unit and neonatal ICU was greater in women with Chikungunya infection in comparison to women without infection. Conclusion- Although Chikungunya infection during pregnancy does not appear to increase Fetomaternal complications, careful monitoring is needed during the maternal viremia period.
| Published in | International Journal of Infectious Diseases and Therapy (Volume 10, Issue 2) |
| DOI | 10.11648/j.ijidt.20251002.13 |
| Page(s) | 47-55 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
CHIKV (Chikungunya Virus), Intrauterine Death, Morbidity, ICU Admission, Pregnancy, Preterm Delivery
Maternal parameters | CHIKUNGUNYA | Chi-square test P value | ||
|---|---|---|---|---|
Positive | Negative | |||
N (%) | N (%) | |||
Anemia | Yes | 21 (44.7%) | 28 (59.5%) | 0.176 |
No | 26 (55.3%) | 19 (41.3%) | ||
Oligohydramnios | Yes | 6 (12.8%) | 3 (6.5%) | 0.486* |
No | 41 (87.2%) | 44 (93.5%) | ||
PROM (Premature rupture of membrane) | Yes | 4 (8.5%) | 3 (6.5%) | 1.000* |
No | 43 (91.5%) | 44 (93.5%) | ||
Gestational age at presentation | 1st Trimester | 3 (6.4%) | 2 (4.3%) | 0.294 |
2nd trimester | 9 (19.1%) | 4 (8.7%) | ||
3rd Trimester | 35 (74.5%) | 41 (87.23%) | ||
Labor | Spontaneous | 10 (21.3%) | 20 (43.5%) | 0.022 |
Induced | 37 (78.7%) | 27 (57.44%) | ||
Maternal Outcome | Stable | 46 (97.9%) | 47 (100.0%) | 1.000 |
Dead | 1 (2.1%) | 0 (0.0%) | ||
Mode of delivery | NVD | 30 (63.8%) | 26 (56.5%) | 0.101 |
LSCS | 10 (21.3%) | 19 (40.4%) | ||
IUD | 3 (6.4%) | 0 (0.0%) | ||
Fetus expulsion | 4 (8.5%) | 2 (4.3%) | ||
Fetal outcomes | CHIKUNGUNYA | Chi-square test P value | ||
|---|---|---|---|---|
Positive N (%) | Negative N (%) | |||
Baby outcome | Live | 38 (80.9%) | 43 (93.5%) | 0.163 |
Abortion | 4 (8.5%) | 2 (4.3%) | ||
IUD | 5 (10.6%) | 2 (4.3%) | ||
Liquor | MSL | 6 (14.3%) | 14 (29.7%) | 0.112 |
Clear | 36 (85.7%) | 33 (71.7%) | ||
NICU admission | Yes | 35 (74.5%) | 0 (0.0%) | <0.001 |
No | 12 (25.5%) | 47 (100.0%) | ||
APGAR <7 at 5 minutes | 5 (10.6%) | 4 (8.5%) | 0.154 | |
Cord blood IgM Positive | 35 neonates of the positive group, were admitted to NICU | 1 (2.1%) | - | |
CHIKUNGUNYA | N | Mean baby Birth weight (grams) | SD | Unpaired t test P value |
|---|---|---|---|---|
Positive | 47 | 2075.213 | 873.5221 | 0.001 |
Negative | 47 | 2585.217 | 573.8244 |
Signs and symptoms associated with fever | CHIKUNGUNYA | Chi-square test P value | ||
|---|---|---|---|---|
Positive | Negative | |||
N (%) | N (%) | |||
Fever spikes | Single | 19 (40.4%) | 29 (63.0%) | 0.029 |
Multiple | 28 (59.6%) | 18 (38.29%) | ||
Rashes | Yes | 7 (14.9%) | 0 (0.0%) | 0.012* |
No | 40 (85.1%) | 47 (100.0%) | ||
Arthralgia | Yes | 19 (40.4%) | 4 (8.7%) | <0.001 |
No | 28 (59.6%) | 43 (91.3%) | ||
Headache | Yes | 29 (61.7%) | 7 (15.2%) | <0.001 |
No | 18 (38.3%) | 40 (85.10%) | ||
Retro-orbital pain | Yes | 12 (25.5%) | 3 (6.5%) | 0.013 |
No | 35 (74.5%) | 44 (93.5%) | ||
Vomiting | Yes | 7 (14.9%) | 3 (6.5%) | 0.316* |
No | 40 (85.1%) | 44 (93.5%) | ||
Condition on delivery | CHIKUNGUNYA | Unpaired t-test P value | |
|---|---|---|---|
Positive | Negative | ||
Mean± SD | Mean± SD | 873.5221 | |
Hemoglobin | 9.8±2.2 | 9.9±1.3 | 0.844 |
TLC | 9297.8±4282.2 | 8952.0±3001.9 | 0.655 |
Platelet count | 1.6±0.8 | 2.3±1.4 | 0.009 |
CKV | Chikungunya Virus |
IgM | Immunoglobulin-M |
N | Number |
| [1] | Basurko, C.; Hcini, N.; Demar, M.; et al. Symptomatic Chikungunya Virus Infection and Pregnancy Outcomes: A Nested Case-Control Study in French Guiana. Viruses 2022, 14, 2705. |
| [2] | Gupta S, Gupta N. Short-term pregnancy outcomes in patients’ chikungunya infection: An observational study. J Family Med Prim Care 2019; 8: 985-7. |
| [3] | Lenglet Y, Barau G, Robillard PY et al. Infection à Chikungunya chez la femme enceinte et risque de transmission maternofetal [Chikungunya infection in pregnancy: Evidence for intrauterine infection in pregnant women and vertical transmission in the parturient. Survey of the Reunion Island outbreak]. J Gynecol Obstet Biol Reprod (Paris). 2006 Oct; 35(6): 578-83. French. |
| [4] | Fritel X, Rollot O, Gerardin P, Gauzere Ba et al. (2010) Chikungunya virus infection during pregnancy, Reunion, France, 2006. Emerg Infect Dis. 2010 Mar; 16(3): 418-25. |
| [5] | Laoprasopwattana K, Suntharasaj T, Petmanee P, et al. (2016) Chikungunya and dengue virus infections during pregnancy: seroprevalence, coincidence and maternal-fetal transmission, southern Thailand, 2009-2010. Epidemiol Infect. 2016 Jan; 144(2): 381-8. |
| [6] | Foeller ME, Nosrat C, Krystosik A, Noel T, et al. (2020) Chikungunya infection in pregnancy - reassuring maternal and perinatal outcomes: a retrospective observational study. BJOG. 2021 May; 128(6): 1077-1086. |
| [7] | Kelly Aparecida Kanunfre Malta, Mussya Cisotto Rocha, Rodrigo Medeiros de Souza et al. (2022) Silent circulation of Chikungunya virus among pregnant women and newborns in the Western Brazilian Amazon before the first outbreak of chikungunya fever. 2022, March; Rev Inst Med Trop São Paulo. 2022; 64: e25 pg 1-8. |
| [8] | Laoprasopwattana, Kamolwish & Kaewjungwad, Lamy & Geater, Alan. (2012). Differential Diagnosis of Chikungunya, Dengue Viral Infection and Other Acute Febrile Illnesses in Children. The Pediatric Infectious Disease journal. 31(5): 459-63. |
| [9] | Natália Salomão, Michelle Brendolin, Kíssila Rabelo, et al. (2021) Spontaneous Abortion and Chikungunya Infection: Pathological Findings. Viruses 2021, 13, 554. |
| [10] | Elizabeth M. Traverse, Hannah K. Hopkins, Vedana Vaidhyanathan et al. Cardiomyopathy and Death Following Chikungunya Infection: An Increasingly Common Outcome. Trop. Med. Infect. Dis. 2021, 6, 108. |
| [11] | Atiene S. Sagay, Szu-Chia Hsieh, Yu-Ching Dai, et al. (2024) Chikungunya virus antepartum transmission and abnormal infant outcomes in a cohort of pregnant women in Nigeria; Int J Infect Dis. 2024 February; 139: 92–100. |
| [12] | Kumar S, Agrawal G, Wazir S, Kumar A, Dubey S, Balde M, et al. (2019) Experience of perinatal and neonatal Chikungunya virus (CHIKV) infection in a tertiary care neonatal center during an outbreak in North India in 2016: a case series. J Trop Pediatr 2019; 65: 169–75. |
| [13] | Bettis AA, L’Azou Jackson M, Yoon IK, Breugelmans JG, Goios A, Gubler DJ, et al. (2022) The global epidemiology of chikungunya from 1999 to 2020: a systematic literature review to inform the development and introduction of vaccines. PLoS Negl Trop Dis 2022; 16: e0010069. |
| [14] | Contopoulos-Ioannidis D, Newman-Lindsay S, Chow C, LaBeaud AD. (2018) Mother-to-child transmission of Chikungunya virus: a systematic review and meta-analysis. PLoS Negl Trop Dis 2018; 12: e0006510. |
| [15] | Jain J, Nayak K, Tanwar N, Gaind R, Gupta B, Shastri JS, et al. (2017) Clinical, serological, and virological analysis of 572 chikungunya patients from 2010 to 2013 in India. Clin Infect Dis 2017; 65: 133–40. |
| [16] | Malek A Role of IgG antibodies in association with placental function and immunologic diseases in human pregnancy. Expert Rev Clin Immunol 2013; 9: 235–49. |
APA Style
Muntaha, Shweta, Poonam. (2025). Fetomaternal Outcomes in Pregnancy in Women with Chikungunya - A Retrospective Observational Study in a Tertiary Care. International Journal of Infectious Diseases and Therapy, 10(2), 47-55. https://doi.org/10.11648/j.ijidt.20251002.13
ACS Style
Muntaha; Shweta; Poonam. Fetomaternal Outcomes in Pregnancy in Women with Chikungunya - A Retrospective Observational Study in a Tertiary Care. Int. J. Infect. Dis. Ther. 2025, 10(2), 47-55. doi: 10.11648/j.ijidt.20251002.13
@article{10.11648/j.ijidt.20251002.13,
author = {Muntaha and Shweta and Poonam},
title = {Fetomaternal Outcomes in Pregnancy in Women with Chikungunya - A Retrospective Observational Study in a Tertiary Care
},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {10},
number = {2},
pages = {47-55},
doi = {10.11648/j.ijidt.20251002.13},
url = {https://doi.org/10.11648/j.ijidt.20251002.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20251002.13},
abstract = {Objective: To evaluate the outcome of pregnancy in patients who developed chikungunya infection during the antenatal period and to evaluate the severity of chikungunya infection in pregnant women. Material and methodology - This retrospective, record-based, observational study recruited, a total of 47 antenatal women who were admitted to the Obst & gynae department in Lady Harding Medical College, hospital and tested chikungunya IgM Antibody positive during the chikungunya outbreak from September 2016 to September 2017 and an equal number of women with fever, but without chikungunya (IgM negative) who were admitted during the same period comparable in age and parity, were taken as a control group. The details of the admitted antenatal women were taken from the medical record section. ELISA IgM was taken as a positive case. The records included a detailed history, examination, investigations, delivery details, and maternal and perinatal outcomes. The pregnancy and neonatal outcomes were compared between pregnant women with fever, with Chikungunya IgM positive and negative. All the data was compiled in a Microsoft Excel sheet using the latest SPSS version. Result- In this study, 356 pregnant women with fever during the study period who were hospitalized were enrolled out of whom 47 had chikungunya IgM positive (13.2%). Out of 309 Chikungunya IgM-negative pregnant women (86.79%), 47 patients were randomly selected as a control group. Out of these 47 patients, one patient required intensive care unit (ICU) and later succumbed, whereas none were transferred to the ICU in the control group. One case of vertical transmission was reported amongst positive neonates. We found that overall chikungunya infection in pregnancy was not significantly associated with any adverse outcomes as compared to controls. However, admission to the Intensive Care Unit and neonatal ICU was greater in women with Chikungunya infection in comparison to women without infection. Conclusion- Although Chikungunya infection during pregnancy does not appear to increase Fetomaternal complications, careful monitoring is needed during the maternal viremia period.
},
year = {2025}
}
TY - JOUR T1 - Fetomaternal Outcomes in Pregnancy in Women with Chikungunya - A Retrospective Observational Study in a Tertiary Care AU - Muntaha AU - Shweta AU - Poonam Y1 - 2025/06/23 PY - 2025 N1 - https://doi.org/10.11648/j.ijidt.20251002.13 DO - 10.11648/j.ijidt.20251002.13 T2 - International Journal of Infectious Diseases and Therapy JF - International Journal of Infectious Diseases and Therapy JO - International Journal of Infectious Diseases and Therapy SP - 47 EP - 55 PB - Science Publishing Group SN - 2578-966X UR - https://doi.org/10.11648/j.ijidt.20251002.13 AB - Objective: To evaluate the outcome of pregnancy in patients who developed chikungunya infection during the antenatal period and to evaluate the severity of chikungunya infection in pregnant women. Material and methodology - This retrospective, record-based, observational study recruited, a total of 47 antenatal women who were admitted to the Obst & gynae department in Lady Harding Medical College, hospital and tested chikungunya IgM Antibody positive during the chikungunya outbreak from September 2016 to September 2017 and an equal number of women with fever, but without chikungunya (IgM negative) who were admitted during the same period comparable in age and parity, were taken as a control group. The details of the admitted antenatal women were taken from the medical record section. ELISA IgM was taken as a positive case. The records included a detailed history, examination, investigations, delivery details, and maternal and perinatal outcomes. The pregnancy and neonatal outcomes were compared between pregnant women with fever, with Chikungunya IgM positive and negative. All the data was compiled in a Microsoft Excel sheet using the latest SPSS version. Result- In this study, 356 pregnant women with fever during the study period who were hospitalized were enrolled out of whom 47 had chikungunya IgM positive (13.2%). Out of 309 Chikungunya IgM-negative pregnant women (86.79%), 47 patients were randomly selected as a control group. Out of these 47 patients, one patient required intensive care unit (ICU) and later succumbed, whereas none were transferred to the ICU in the control group. One case of vertical transmission was reported amongst positive neonates. We found that overall chikungunya infection in pregnancy was not significantly associated with any adverse outcomes as compared to controls. However, admission to the Intensive Care Unit and neonatal ICU was greater in women with Chikungunya infection in comparison to women without infection. Conclusion- Although Chikungunya infection during pregnancy does not appear to increase Fetomaternal complications, careful monitoring is needed during the maternal viremia period. VL - 10 IS - 2 ER -
Department of Obstetrics and Gynaecology, Lady Harding Medical College, Delhi, India
Department of Obstetrics and Gynaecology, Lady Harding Medical College, Delhi, India
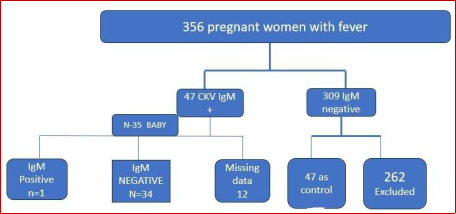
Figure 1. Flow chart of case selection.
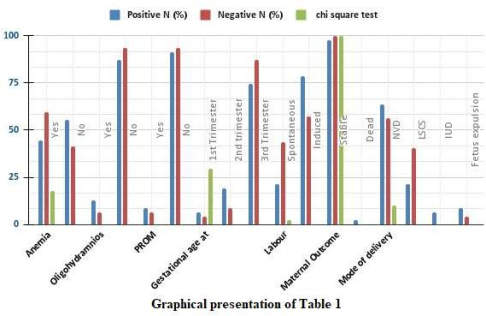
Figure 2.
Graphical representation of the maternal outcome of chikungunya-positive and negative patients.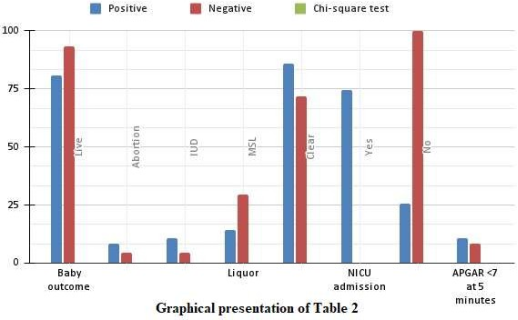
Figure 3.
Graphical representation of neonatal outcome in Chikungunya positive and negative patient.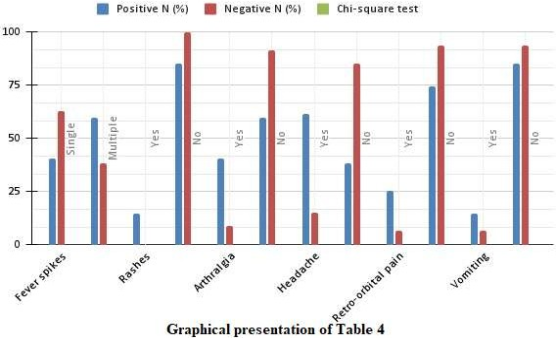
Figure 4.
Symptomatology of Pregnant Women.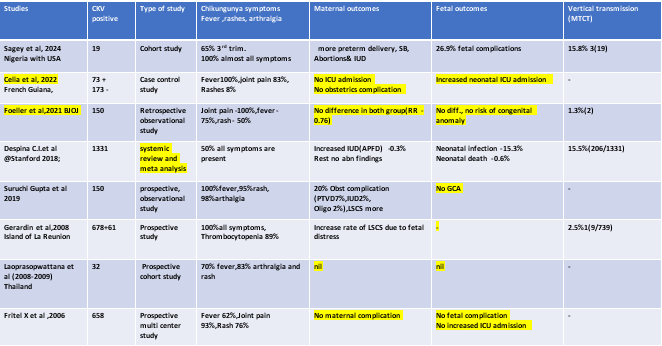
Figure 5. Comparative outcomes of different studies.
Information

