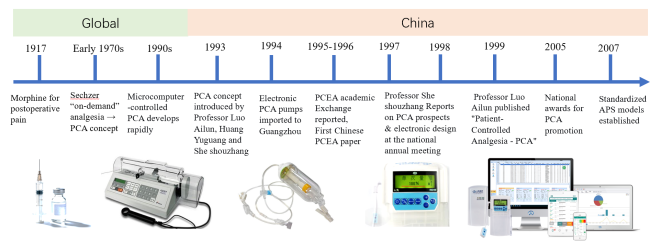
Postoperative pain management is a cornerstone of perioperative medicine, and the accuracy of pain assessment directly determines analgesic efficacy. For decades, Chinese clinical practice has relied heavily on translated versions of foreign pain assessment scales, which often suffer from inadequate cultural adaptation, strong subjectivity, and a unidimensional focus on pain intensity. In 1993, the concept of patient-controlled analgesia (PCA) was introduced in China, followed by widespread clinical adoption by 1998. In 2011, China developed the world's first artificial intelligence PCA (Ai-PCA) pump, with subsequent expert consensus documents published in 2018 and 2024. Leveraging accumulated experience with Ai-PCA, a Chinese research team developed the Smart Patient-Controlled Analgesia Outcome Chinese Pain Assessment Scale (S-CPAS) in 2025. This innovative, intelligent assessment system marks a paradigm shift from subjective, experience-based evaluation to data-driven, multidimensional assessment. The S-CPAS integrates the Pain Comprehensive Index (PCI) – covering pain intensity, functional impacts, adverse reactions, pump operational quality, sedation, and muscle strength – with patient satisfaction scores. It has demonstrated good reliability and validity in multicenter studies. This review systematically examines the past, present, and future of clinical applications of postoperative pain assessment scales in China. We discuss the historical evolution of postoperative analgesia, the limitations of traditional tools, and the core innovations of the S-CPAS in individualization, precision, and intelligence. Future directions include the integration of S-CPAS with the Virtual Pain Unit (VPU) and Acute Pain Service (APS) collaborative management model to enable precision multimodal analgesia (PMA). Other emerging trends are the use of wearable sensors, multimodal physiological monitoring, machine learning-based pain trajectory prediction, and out-of-hospital remote analgesia management. We call for widespread adoption of the S-CPAS-based intelligent assessment platform to promote standardized, high-quality postoperative pain management in China and to contribute to the “Healthy China” strategy.
| Published in | International Journal of Pain Research (Volume 2, Issue 2) |
| DOI | 10.11648/j.ijpr.20260202.14 |
| Page(s) | 61-69 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Postoperative Pain, Pain Assessment Scale, Intelligent Patient-controlled Analgesia, Precision Multimodal Analgesia, S-CPAS
Component / Dimension | Number of items | Scoring method | Clinical function / Remarks |
|---|---|---|---|
Part 1: Pain Comprehensive Index (PCI) | |||
A. Postoperative pain assessment | 10 | 0–10 linear analog scale (0 = no pain/no impact; 10 = worst pain/complete impact) | Covers resting pain, activity pain, functional exercise pain, and impact on breathing, eating, sleep, walking, communication, depression, anxity. |
B. Postoperative adverse reaction assessment | 8 (after deletion of low-incidence items: headache, urinary retention) | 0–10 linear analog scale (0 = none; 10 = most severe) | Quantifies nausea, vomiting, repiratory depression, drowsiness, dizziness, pruritus, constipation, agitation. Monitors opioid-related side effects. |
C. PCA pump operational quality evaluation | 6 (after deletion of "staff follow-up") | 0–10 linear analog scale (0 = worst; 10 = best) | Assesses patient understanding, analgesic need satisfaction, relief after single/multiple presses, frquency of device failures, impact of failures on analgesia. |
R. Ramsay Sedation Score | 1 | Ordinal scale (1–6: 1 = anxious/agitated; 6 = deep sleep, no response) | Prevents excessive sedation; targets moderate sedation (score 3) to rduce stress and improve comfort. |
J. Muscle strength assessment | 1 | Ordinal scale (0–5: 0 = no contraction; 5 = normal strength against full resistance) | Guides early mobilization and functional exercise; monitors pain-related limitation of movment. |
Part 2: Analgesia satisfaction | 5 | 0–10 linear analog scale (0 = extremely dissatisfied; 10 = very satisfied); average of 5 items = final satisfaction score | Patient-centered outcome: satisfaction with pump use, rescue effect, staff response time, whole-process service, overall analgesic effect. |
Integrated intelligent functions | |||
Automatic data collection | – | Real-time capture of Ai-PCA pump parameters (press frequency, alarms, drug usage, etc.) | Eliminates recall bias; ensures objectivity. |
Quality Control Platform | – | Generates PCI and satisfaction curves (blue low curve = pain control; red high curve = satisfaction) | Enables paperless, information-driven, intelligent follow-up. |
Analgesia Quality Index (AQI) | – | Real-time intelligent scoring (0–100) based on multiple parameters; | Reflects quality control awareness, technical level, management standardization. |
AI | Artificial Intelligence |
APS | Acute Pain Service |
AQI | Analgesia Quality Index |
ERAS | Enhanced Recovery After Surgery |
PCA | Patient-controlled Analgesia |
PCEA | Patient-controlled Epidural Analgesia |
PMA | Precision Multimodal Analgesia |
PCI | Pain Comprehensive Index |
PCASS | Patient-controlled Analgesia System Solution |
S-CPAS | Smart Patient-controlled Analgesia Outcome Chinese Pain Assessment Scale |
VPU | Virtual Pain Unit |
VAS | Visual Analog Scale |
| [1] | Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020; 161(9): 1976-1982. |
| [2] | Sloman R, Wruble AW, Rosen G, et al. Determination of clinically meaningful levels of pain reduction in patients experiencing acute postoperative pain. Pain Manag Nurs. 2006; 7: 153-158. |
| [3] | Samuel L, Laura E, Ashish D, et al. Reliability, validity, and responsiveness of multidimensional pain assessment tools used in postoperative adult patients: a systematic review of measurement properties. JBI Evid Synth. 2021; 19(2): 284-307. |
| [4] | Wang Y, Chu QJ, Zheng B, et al. Development and validation of the Smart Patient-Controlled Analgesia Outcome Chinese Pain Assessment Scale: a multicenter clinical study. Chinese Journal of Painology. 2026; 22(1): 30-43. |
| [5] | Sechzer PH. Studies in pain with the analgesic-demand system. Anesth Analg. 1971; 50(1): 1-10. |
| [6] | Ji YL. Brief report on the first pain treatment symposium of the Chinese Society of Anesthesiology. Journal of Medical Research. 1989; 17(12): 22-24. |
| [7] | Shi Shouzhang. Clinical Application Research Progress of Patient-Controlled Analgesia (Part One) [J]. Guangzhou Pharmaceutical, 1999, 30(1): 3-5. |
| [8] | She SZ, Liu JY, Xu LX, et al. Observation of clinical effects of different buprenorphine combinations for epidural patient-controlled analgesia (PCEA). Chinese Journal of Pain Medicine. 1996; 2(3): 203-205. |
| [9] | She SZ, Liu JY, Liu R, et al. Clinical study of PCEA after combined spinal-epidural anesthesia. Chinese Journal of Anesthesiology. 1998; 18(6): 378-379. |
| [10] | She SZ, Xu XB, Xiao JB, et al. Effect of continuous epidural infusion of ropivacaine at different rates on morphine PCA consumption. Chinese Journal of Anesthesiology. 2000; 20(9): 708-711. |
| [11] | She SZ, Liu JY, Wang J, et al. Pharmacokinetic study of lidocaine during epidural patient-controlled analgesia. Chinese Journal of Anesthesiology. 1997; 17(9): 557-560. |
| [12] | She SZ, Liu JY, Xu LX, et al. Comparison of different fentanyl combinations for postoperative epidural patient-controlled analgesia. Chinese Journal of Anesthesiology. 1997; 17(49): 245-248. |
| [13] | She SZ, Liu JY, Hu SJ, et al. Clinical effects and plasma concentration of different PCA doses of epidural morphine. Chinese Journal of Anesthesiology. 1999; 19(6): 708-711. |
| [14] | Xu XB, She SZ, Liu JY, et al. Effect of different concentrations of ropivacaine combined with morphine for postoperative PCEA on patients’ ventilation function. Journal of Clinical Anesthesiology. 2001; 17(4): 411-413. |
| [15] | She SZ. Standardized construction of acute pain treatment system. Chinese Journal of Pain Medicine. 2006; 12(2): 68-69. |
| [16] | Hong X, Huang YG, Luo AL. Standardized management of postoperative analgesia. Chinese Journal of Anesthesiology. 2005; 25(10): 798-799. |
| [17] | Ruan XC, She SZ, Xu LX, et al. Ten years’ experience in standardized management of acute pain treatment. Chinese Journal of Pain Medicine. 2006; 12(2): 69-70. |
| [18] | Wan L, Zhao Q, Chen J, et al. Chinese expert consensus on the application of pain assessment scales (2020 edition). Chinese Journal of Painology. 2020; 16(3): 177-187. |
| [19] | Boring BL, Walsh KT, Nanavaty N, et al. How and Why Patient Concerns Influence Pain Reporting: A Qualitative Analysis of Personal Accounts and Perceptions of Others' Use of Numerical Pain Scales. Front Psychol. 2021; 12: 663890. |
| [20] | Jensen MP, Miró J, Euasobhon P. Assessing pain intensity: critical questions for researchers and clinicians. Anaesthesia. 2024; 79(2): 114-118. |
| [21] | Xie WW, Wang Y, Chu QJ, et al. Current status and future of clinical application of postoperative acute pain assessment scales in adults. Chinese Journal of Painology. 2025; 21(4): 559-565. |
| [22] | Zhao YP, Xiong LZ. Chinese expert consensus and pathway management guidelines for enhanced recovery after surgery (2018 edition). Chinese Journal of Practical Surgery. 2018; 38(1): 1-20. |
| [23] | Pain Group of Chinese Society of Anesthesiology. Clinical practice guidelines for postoperative pain management in adults (2024 edition). Chinese Journal of Anesthesiology. 2025; 21(9): 1045-1079. |
| [24] | Dolin SJ, Cashman JN, Bland JM. Effectiveness of acute postoperative pain management: I. Evidence from published data. Br J Anaesth. 2002; 89(3): 409-423. |
| [25] | Gan TJ, Habib AS, Miller TE, et al. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. 2014; 30(1): 149-160. |
| [26] | van Boekel RL, Steegers MA, Verbeek-van Noord I, et al. Acute pain services and postsurgical pain management in the Netherlands: a survey. Pain Pract. 2015; 15(5): 447-454. |
| [27] | Cao HZ, Huang WQ, Peng SL, et al. Effect of intelligent PCA management on quality of postoperative analgesia in patients. Chinese Journal of Anesthesiology. 2018; 38(9): 1077-1081. |
| [28] | Zhang QF, Zhang R, He M, et al. A survey of perioperative pain treatment and management in China. Chinese Journal of Anesthesiology. 2017; 37(12): 1409-1413. |
| [29] | She SZ, Yu WF, Huang YG, et al. Expert consensus on clinical application standards of patient-controlled analgesia. Chinese Journal of Painology. 2024; 20(4): 509-526. |
| [30] | She SZ, Zheng B, Cao HZ, et al. Application of the innovative Chinese smart patient-controlled analgesia outcome pain assessment scale to promote the quality of clinical precision multimodal analgesia. Chinese Journal of Painology. 2026; 22(1): 1-4. |
| [31] | Cao HZ, Liu M, She SZ. Innovation of intelligent patient-controlled analgesia system and the regulations and standards it complies with. Guangdong Medical Journal. 2020; 41(11): 1088-1091. |
| [32] | She SZ, Yao SL, Yu WF, et al. Patient-controlled analgesia should develop towards standardized high-quality development in the direction of digital and intelligent medicine. Chinese Journal of Painology. 2024; 20(4): 481-483. |
| [33] | She SZ, Zheng B, Cao HZ, et al. Interpretation and implementation prospects of the “Expert Consensus on Clinical Application Standards of Patient-Controlled Analgesia” based on intelligent analgesia technology. Chinese Journal of Painology. 2025; 21(2): 281-285. |
| [34] | Wang Q, Cao HZ, Xiong LZ. PCA intellectualization and improvement of postoperative analgesia quality. Chinese Journal of Anesthesiology. 2018; 38(3): 257-258. |
| [35] | Jiang JJ, Wang YM, Zhang H. Progress in clinical application of information technology in postoperative pain assessment and intelligent management. Guangdong Medical Journal. 2023; 44(12): 1453-1458. |
| [36] | She SZ. Efforts to promote the rapid development of intelligent patient-controlled analgesia technology. Chinese Journal of Painology. 2023; 19(1): 3-5. |
| [37] | Xiao W, Wang TL. Concept and clinical practice of precision multimodal analgesia. Beijing Medical Journal. 2025; 47(3): 181-183. |
| [38] | Zhang LS. A call for promoting basic and original research in pain science in China. Chinese Journal of Painology. 2025; 21(5): 641-642. |
| [39] | She SZ. Innovation leads the clinical application research of intelligent patient-controlled analgesia. Guangdong Medical Journal. 2023; 44(3): 265-270. |
| [40] | Khalifa A, Hussein R. Artificial Intelligence For 6P Medicine: Consolidating AI Needs of Predictive, Preventive, Personalized, Participatory, Precision, and Public Health Trajectories. J Med Syst. 2026; 50(1): 56. |
APA Style
She, S., Zheng, B., Cao, H., Chu, Q., Wang, T., et al. (2026). New Advances in the Clinical Application of Postoperative Analgesia and Pain Assessment Scales in China. International Journal of Pain Research, 2(2), 61-69. https://doi.org/10.11648/j.ijpr.20260202.14
ACS Style
She, S.; Zheng, B.; Cao, H.; Chu, Q.; Wang, T., et al. New Advances in the Clinical Application of Postoperative Analgesia and Pain Assessment Scales in China. . 2026, 2(2), 61-69. doi: 10.11648/j.ijpr.20260202.14
@article{10.11648/j.ijpr.20260202.14,
author = {Shouzhang She and Bin Zheng and Hanzhong Cao and Qinjun Chu and Tianlong Wang and Weifeng Yu},
title = {New Advances in the Clinical Application of Postoperative Analgesia and Pain Assessment Scales in China},
journal = {International Journal of Pain Research},
volume = {2},
number = {2},
pages = {61-69},
doi = {10.11648/j.ijpr.20260202.14},
url = {https://doi.org/10.11648/j.ijpr.20260202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijpr.20260202.14},
abstract = {Postoperative pain management is a cornerstone of perioperative medicine, and the accuracy of pain assessment directly determines analgesic efficacy. For decades, Chinese clinical practice has relied heavily on translated versions of foreign pain assessment scales, which often suffer from inadequate cultural adaptation, strong subjectivity, and a unidimensional focus on pain intensity. In 1993, the concept of patient-controlled analgesia (PCA) was introduced in China, followed by widespread clinical adoption by 1998. In 2011, China developed the world's first artificial intelligence PCA (Ai-PCA) pump, with subsequent expert consensus documents published in 2018 and 2024. Leveraging accumulated experience with Ai-PCA, a Chinese research team developed the Smart Patient-Controlled Analgesia Outcome Chinese Pain Assessment Scale (S-CPAS) in 2025. This innovative, intelligent assessment system marks a paradigm shift from subjective, experience-based evaluation to data-driven, multidimensional assessment. The S-CPAS integrates the Pain Comprehensive Index (PCI) – covering pain intensity, functional impacts, adverse reactions, pump operational quality, sedation, and muscle strength – with patient satisfaction scores. It has demonstrated good reliability and validity in multicenter studies. This review systematically examines the past, present, and future of clinical applications of postoperative pain assessment scales in China. We discuss the historical evolution of postoperative analgesia, the limitations of traditional tools, and the core innovations of the S-CPAS in individualization, precision, and intelligence. Future directions include the integration of S-CPAS with the Virtual Pain Unit (VPU) and Acute Pain Service (APS) collaborative management model to enable precision multimodal analgesia (PMA). Other emerging trends are the use of wearable sensors, multimodal physiological monitoring, machine learning-based pain trajectory prediction, and out-of-hospital remote analgesia management. We call for widespread adoption of the S-CPAS-based intelligent assessment platform to promote standardized, high-quality postoperative pain management in China and to contribute to the “Healthy China” strategy.},
year = {2026}
}
TY - JOUR T1 - New Advances in the Clinical Application of Postoperative Analgesia and Pain Assessment Scales in China AU - Shouzhang She AU - Bin Zheng AU - Hanzhong Cao AU - Qinjun Chu AU - Tianlong Wang AU - Weifeng Yu Y1 - 2026/05/26 PY - 2026 N1 - https://doi.org/10.11648/j.ijpr.20260202.14 DO - 10.11648/j.ijpr.20260202.14 T2 - International Journal of Pain Research JF - International Journal of Pain Research JO - International Journal of Pain Research SP - 61 EP - 69 PB - Science Publishing Group SN - 3070-1562 UR - https://doi.org/10.11648/j.ijpr.20260202.14 AB - Postoperative pain management is a cornerstone of perioperative medicine, and the accuracy of pain assessment directly determines analgesic efficacy. For decades, Chinese clinical practice has relied heavily on translated versions of foreign pain assessment scales, which often suffer from inadequate cultural adaptation, strong subjectivity, and a unidimensional focus on pain intensity. In 1993, the concept of patient-controlled analgesia (PCA) was introduced in China, followed by widespread clinical adoption by 1998. In 2011, China developed the world's first artificial intelligence PCA (Ai-PCA) pump, with subsequent expert consensus documents published in 2018 and 2024. Leveraging accumulated experience with Ai-PCA, a Chinese research team developed the Smart Patient-Controlled Analgesia Outcome Chinese Pain Assessment Scale (S-CPAS) in 2025. This innovative, intelligent assessment system marks a paradigm shift from subjective, experience-based evaluation to data-driven, multidimensional assessment. The S-CPAS integrates the Pain Comprehensive Index (PCI) – covering pain intensity, functional impacts, adverse reactions, pump operational quality, sedation, and muscle strength – with patient satisfaction scores. It has demonstrated good reliability and validity in multicenter studies. This review systematically examines the past, present, and future of clinical applications of postoperative pain assessment scales in China. We discuss the historical evolution of postoperative analgesia, the limitations of traditional tools, and the core innovations of the S-CPAS in individualization, precision, and intelligence. Future directions include the integration of S-CPAS with the Virtual Pain Unit (VPU) and Acute Pain Service (APS) collaborative management model to enable precision multimodal analgesia (PMA). Other emerging trends are the use of wearable sensors, multimodal physiological monitoring, machine learning-based pain trajectory prediction, and out-of-hospital remote analgesia management. We call for widespread adoption of the S-CPAS-based intelligent assessment platform to promote standardized, high-quality postoperative pain management in China and to contribute to the “Healthy China” strategy. VL - 2 IS - 2 ER -
Department of Anesthesiology, Guangzhou First People's Hospital, Guangzhou, China
Department of Anesthesiology, Tumor Hospital Affiliated to Nantong University, Nantong, China
Department of Anesthesiology and Perioperative Medicine, Zhengzhou Central Hospital, Zhengzhou, China
Department of Anesthesiology, Xuanwu Hospital, Capital Medical University, Beijing, China
Department of Anesthesiology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China;Department of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China
Information