Background: Ganglioneuromas are rare, benign tumors derived from neural crest cells of the sympathetic nervous system. These tumors are typically found in the posterior mediastinum and retroperitoneum, and are characterized by well-differentiated ganglion and Schwann cells. Presacral ganglioneuromas are extremely uncommon, with few cases documented in the literature. Their rarity and nonspecific clinical presentation can pose diagnostic challenges. It is worth mentioning that there are few cases in the literature report ganglioneuroma in association with MEN type 2B. Case Presentation: We report the case of a 30-year-old female who presented with a three-month history of mild lower abdominal discomfort and non-radicular lower back pain. Her physical examination was unremarkable, and routine laboratory investigations, including tumor markers and catecholamine levels, were within normal limits. Initial ultrasonography was inconclusive. However, contrast-enhanced computed tomography (CT) revealed a well-circumscribed, 5 × 3 cm lesion in the presacral region, causing widening of the right middle sacral foramina. Magnetic resonance imaging (MRI) further characterized the mass as isointense on T1-weighted imaging and heterogeneously hyperintense on T2-weighted imaging, with peripheral enhancement after gadolinium administration. Given its location and imaging characteristics, the lesion was surgically excised via microscopic resection. The postoperative course was uneventful, and the patient was discharged in stable condition. Histopathologic analysis confirmed the diagnosis of ganglioneuroma, revealing mature ganglion cells embedded in a schwannian stroma with fibrous and edematous areas. Conclusion: This case underscores the importance of considering ganglioneuroma in the differential diagnosis of presacral masses. Timely imaging and surgical intervention are key to effective management and favorable outcomes. We present a rare case of a presacral ganglioneuroma in a 30-year-old female patient who experienced mild lower abdominal discomfort and non-radicular lower back pain over a three-month period, without significant neurological symptoms. Diagnostic imaging revealed a presacral lesion at the S2-3 level, leading to a surgical intervention that resulted in a subtotal excision of the mass. Histopathological analysis confirmed the diagnosis of ganglioneuroma. This case underscores the importance of considering presacral ganglioneuroma in the differential diagnosis of presacral lesions, given their subtle presentation and potential complications.
| Published in | Journal of Cancer Treatment and Research (Volume 13, Issue 2) |
| DOI | 10.11648/j.jctr.20251302.11 |
| Page(s) | 23-26 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Presacral Mass, Ganglioneuroma, Abdominal Pain, Back Pain, Surgery
MEN | Multiple Endocrine Neoplasia |
CT | Computed Tomography |
HU | Hounsfield Unit |
MRI | Magnetic Resonance Imaging |
T1WI | T1-weighted Image |
T2WI | T2-weighted Image |
GAD | Gadolinium |
H&E | Hematoxylin and Eosin |
| [1] | Kamatam, N., Rayappan, E., Smile, S. & Vivekanandan, R. (2016), Large ganglioneuroma presenting as presacral mass, BJR|Case Reports, 2 (4), 20150361, |
| [2] | Mounasamy, V., Thacker, M. M., Humble, S. et al (2006). Ganglioneuromas of the sacrum-a report of two cases with radiologic-pathologic correlation. Skeletal Radiol 35, 117-121. |
| [3] | Cerullo, G. (2007). Presacral Ganglioneuroma: A case report and review of literature. World Journal of Gastroenterology, 13(14), 2129. |
| [4] | Basak, F., Kilic, A., Su Dur, M., Sisik, A., & Kivanc, A. (2019). A clinical and surgical challenge: Retrorectal tumors. Journal of Cancer Research and Therapeutics, 15(1), 132. |
| [5] | Yang, B.-L. (2010). Retrorectal tumors in adults: Magnetic resonance imaging findings. World Journal of Gastroenterology, 16(46), 5822. |
| [6] | Shenoy, S. (2018). Diagnosis and management of Presacral (Retrorectal) tumors. Journal of Gastrointestinal Cancer, 49(3), 373-378. |
| [7] | Körfer D, & Jentschura D. (2023). Surgical Management of Presacral Tumors: Report of 5 Cases With Video Vignette of Laparoscopic Removal. Surg Laparosc Endosc Percutan Tech, 1; 33(2): 198-201. |
| [8] | Hayes, F. A., Green, A. A., & Rao, B. N. (1989). Clinical manifestations of ganglioneuroma. Cancer, 63(6), 1211-1214. |
| [9] | Modha, A., Paty, P., & Bilsky, M. H. (2005). Presacral ganglioneuromas. Report of five cases and review of the literature. Journal of neurosurgery. Spine, 2(3), 366-371. |
| [10] | Leeson, M. C., & Hite, M. (1989). Ganglioneuroma of the sacrum. Clinical orthopaedics and related research, (246), 102-105. |
| [11] | Marmor, E., Fourney, D. R., Rhines, L. D., Skibber, J. M., Fuller, G. N., & Gokaslan, Z. L. (2002). Sacrococcygeal ganglioneuroma. Journal of spinal disorders & techniques, 15(3), 265-268. |
| [12] | Andersen, H. J., Hansen, L. G., Lange, P., & Teglbjaerg, P. S. (1986). Presacral ganglioneuroma. Case report. Acta chirurgica Scandinavica, 152, 777-778. |
| [13] | MacCarty, C. S., Waugh, J. M., Coventry, M. B., & Cope, W. F., Jr (1965). Surgical treatment of sacral and presacral tumors other than sacrococcygeal chordoma. Journal of neurosurgery, 22(5), 458-464. |
| [14] | Richardson, R. R., Reyes, M., Sanchez, R. A., Torres, H., & Vela, S. (1986). Ganglioneuroma of the sacrum. A case report. Spine, 11(1), 87-89. |
| [15] | Lee, D., Choe, W. J., & Lim, S. D. (2017). Ganglioneuroma of the Sacrum. Korean Journal of Spine, 14(3), 106-108. |
| [16] | Rycyk-Bojarzyńska, A., Kasztelan-Szczerbińska, B., Cichoż-Lach, H., & Jargieło, A. (2024). Ganglioneuromatous polyposis associated with type 2 B multiple endocrine neoplasia (MEN 2B) - case report. Annals of agricultural and environmental medicine: AAEM, 31(2), 302-305. |
APA Style
Najjar, A. K., Salman, A. A., Aldarawish, A. M., Abdul-Samee’ Bakri, I. (2025). Presacral Ganglioneuroma in a 30-Year-Old Female: Case Report and Literature Review. Journal of Cancer Treatment and Research, 13(2), 23-26. https://doi.org/10.11648/j.jctr.20251302.11
ACS Style
Najjar, A. K.; Salman, A. A.; Aldarawish, A. M.; Abdul-Samee’ Bakri, I. Presacral Ganglioneuroma in a 30-Year-Old Female: Case Report and Literature Review. J. Cancer Treat. Res. 2025, 13(2), 23-26. doi: 10.11648/j.jctr.20251302.11
@article{10.11648/j.jctr.20251302.11,
author = {Alaa Khaled Najjar and Ayman Ahmad Salman and Asad Mohammad Aldarawish and Izzeddin Abdul-Samee’ Bakri},
title = {Presacral Ganglioneuroma in a 30-Year-Old Female: Case Report and Literature Review
},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {2},
pages = {23-26},
doi = {10.11648/j.jctr.20251302.11},
url = {https://doi.org/10.11648/j.jctr.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251302.11},
abstract = {Background: Ganglioneuromas are rare, benign tumors derived from neural crest cells of the sympathetic nervous system. These tumors are typically found in the posterior mediastinum and retroperitoneum, and are characterized by well-differentiated ganglion and Schwann cells. Presacral ganglioneuromas are extremely uncommon, with few cases documented in the literature. Their rarity and nonspecific clinical presentation can pose diagnostic challenges. It is worth mentioning that there are few cases in the literature report ganglioneuroma in association with MEN type 2B. Case Presentation: We report the case of a 30-year-old female who presented with a three-month history of mild lower abdominal discomfort and non-radicular lower back pain. Her physical examination was unremarkable, and routine laboratory investigations, including tumor markers and catecholamine levels, were within normal limits. Initial ultrasonography was inconclusive. However, contrast-enhanced computed tomography (CT) revealed a well-circumscribed, 5 × 3 cm lesion in the presacral region, causing widening of the right middle sacral foramina. Magnetic resonance imaging (MRI) further characterized the mass as isointense on T1-weighted imaging and heterogeneously hyperintense on T2-weighted imaging, with peripheral enhancement after gadolinium administration. Given its location and imaging characteristics, the lesion was surgically excised via microscopic resection. The postoperative course was uneventful, and the patient was discharged in stable condition. Histopathologic analysis confirmed the diagnosis of ganglioneuroma, revealing mature ganglion cells embedded in a schwannian stroma with fibrous and edematous areas. Conclusion: This case underscores the importance of considering ganglioneuroma in the differential diagnosis of presacral masses. Timely imaging and surgical intervention are key to effective management and favorable outcomes. We present a rare case of a presacral ganglioneuroma in a 30-year-old female patient who experienced mild lower abdominal discomfort and non-radicular lower back pain over a three-month period, without significant neurological symptoms. Diagnostic imaging revealed a presacral lesion at the S2-3 level, leading to a surgical intervention that resulted in a subtotal excision of the mass. Histopathological analysis confirmed the diagnosis of ganglioneuroma. This case underscores the importance of considering presacral ganglioneuroma in the differential diagnosis of presacral lesions, given their subtle presentation and potential complications.},
year = {2025}
}
TY - JOUR T1 - Presacral Ganglioneuroma in a 30-Year-Old Female: Case Report and Literature Review AU - Alaa Khaled Najjar AU - Ayman Ahmad Salman AU - Asad Mohammad Aldarawish AU - Izzeddin Abdul-Samee’ Bakri Y1 - 2025/07/16 PY - 2025 N1 - https://doi.org/10.11648/j.jctr.20251302.11 DO - 10.11648/j.jctr.20251302.11 T2 - Journal of Cancer Treatment and Research JF - Journal of Cancer Treatment and Research JO - Journal of Cancer Treatment and Research SP - 23 EP - 26 PB - Science Publishing Group SN - 2376-7790 UR - https://doi.org/10.11648/j.jctr.20251302.11 AB - Background: Ganglioneuromas are rare, benign tumors derived from neural crest cells of the sympathetic nervous system. These tumors are typically found in the posterior mediastinum and retroperitoneum, and are characterized by well-differentiated ganglion and Schwann cells. Presacral ganglioneuromas are extremely uncommon, with few cases documented in the literature. Their rarity and nonspecific clinical presentation can pose diagnostic challenges. It is worth mentioning that there are few cases in the literature report ganglioneuroma in association with MEN type 2B. Case Presentation: We report the case of a 30-year-old female who presented with a three-month history of mild lower abdominal discomfort and non-radicular lower back pain. Her physical examination was unremarkable, and routine laboratory investigations, including tumor markers and catecholamine levels, were within normal limits. Initial ultrasonography was inconclusive. However, contrast-enhanced computed tomography (CT) revealed a well-circumscribed, 5 × 3 cm lesion in the presacral region, causing widening of the right middle sacral foramina. Magnetic resonance imaging (MRI) further characterized the mass as isointense on T1-weighted imaging and heterogeneously hyperintense on T2-weighted imaging, with peripheral enhancement after gadolinium administration. Given its location and imaging characteristics, the lesion was surgically excised via microscopic resection. The postoperative course was uneventful, and the patient was discharged in stable condition. Histopathologic analysis confirmed the diagnosis of ganglioneuroma, revealing mature ganglion cells embedded in a schwannian stroma with fibrous and edematous areas. Conclusion: This case underscores the importance of considering ganglioneuroma in the differential diagnosis of presacral masses. Timely imaging and surgical intervention are key to effective management and favorable outcomes. We present a rare case of a presacral ganglioneuroma in a 30-year-old female patient who experienced mild lower abdominal discomfort and non-radicular lower back pain over a three-month period, without significant neurological symptoms. Diagnostic imaging revealed a presacral lesion at the S2-3 level, leading to a surgical intervention that resulted in a subtotal excision of the mass. Histopathological analysis confirmed the diagnosis of ganglioneuroma. This case underscores the importance of considering presacral ganglioneuroma in the differential diagnosis of presacral lesions, given their subtle presentation and potential complications. VL - 13 IS - 2 ER -
Department of Neurosurgery, Al-Makassed Islamic Charitable Society Hospital, Jerusalem, Palestine
Department of Neurosurgery, Al-Makassed Islamic Charitable Society Hospital, Jerusalem, Palestine
Department of Neurosurgery, Al-Makassed Islamic Charitable Society Hospital, Jerusalem, Palestine
Department of Pathology, Al-Makassed Islamic Charitable Society Hospital, Jerusalem, Palestine
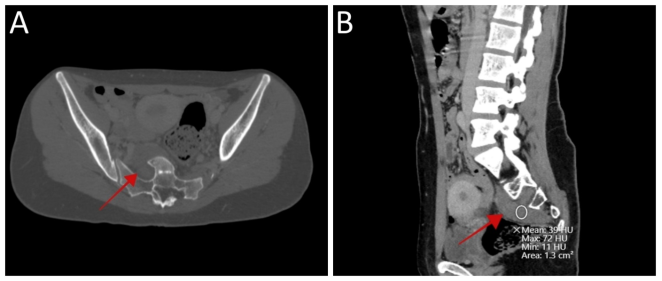
Figure 1. Pre-operative CT scan with contrast displaying well-circumscribed lesion in the presacral area with a rim of peripheral enhancement causing widening of the right middle neural sacral foramina and remodeling of the adjacent structures with no calcifications (red arrow) and the mean Hounsfield unit is 39: (A) axial view and (B) sagittal view. [CT = computed tomography, HU = Hounsfield unit]
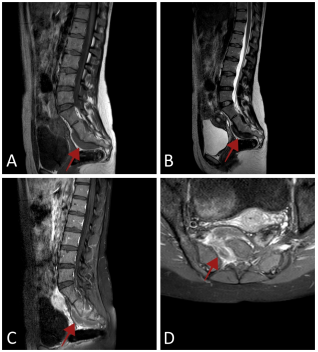
Figure 2. Pre-operative pelvic MRI exhibiting: (A) an isointense presacral lesion opposite to S2-S3 level on sagittal T1WI, (B) a heterogeneous hyppintense on sagittal T2WI, and (C: sagittal and D: axial) a peripheral enhancement after GAD administration on T1WI.
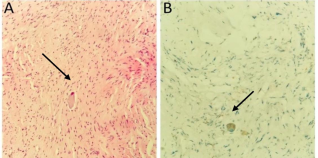
Figure 3. Histopathological slide showing: (A) an intersecting bundles of schwann cells (arrow) and scattered nests and clusters of ganglion cells [H&E stain, original magnification ×20], and (B) synaptophysin immunostain highlights ganglion cell (arrow).
Information

