2. Background
Before this paper looks at its main objective of the psychological impact of treating breast cancer with the patient fully awake, here’s a short review of the plethora of scientific papers published on the psychological impact of breast cancer diagnosis, including pre-treatment diagnostics, the treatment itself and post treatment including higher rates of suicide. There is no question that major advances have been made in the diagnosis and treatment of breast cancer since Dr. Vincent DeVita Jr. made his famous pronouncement that in the past all women with breast cancer underwent mastectomy with just skin covering bone and then they died.
| [1] | New Yorker Magazine, Dec 7th 2015, Dr. Vincent Devita. |
[1]
.
More recent papers like ‘Suicide risk among female breast cancer survivors:
| [2] | Frontiers in Oncology, 2022 Nov 24: 12: 986822. |
[2]
A population-based study sheds dramatic light on a summing up of all efforts. That article refers to a paper entitled ‘Trends in health-related quality of life of female breast cancer survivors using the Medical Expenditure Panel Survey (MEPS), 2008-2016.’
| [3] | Medical Expenditure Survey (MEPS), 2008-2026. |
[3]
And they say, “Despite all of the attention being paid to breast cancer survivorship, recent years have shown a very slight improvement in quality of life.”
The paper’s main focus, however, is the higher rate of suicide seen in breast cancer patients, especially in the younger age group. Other papers like ‘Breast Cancer: The Psychological Impact of Diagnosis, Treatment, and Remission’ published in Cureus 2024 Oct 4; 16
| [4] | Cureus 2024, Oct 4: 16 (10). |
[4]
discuss the following, “The psychological status of the patient must be addressed by the Multi-Disciplinary Team (MDT) during treatment.” All of the papers discuss the side effects of breast cancer including not only those affecting the patient but family members and friends. To name just a few, anxiety (just scheduling a mammogram), depression, loss of body image and femininity, fear of disfigurement, fear of chemo brain, fear of losing a husband or not ever getting one, fear of leaving children behind, fear of intimacy, and death. This list is not exhaustive.
If we couple all these together and more recent papers like, ‘Home Recovery After Mastectomy (HRAM) Gaining momentum,’ the so called “drive-by mastectomy’, published in clinicaloncology.com Breast Cancer/Article 10-22,
| [5] | Clinicaloncology.com Breast Cancer Article 10-22. |
[5]
it’s not hard to envision a nurse wheeling a patient out to the parking lot after her outpatient mastectomy and saying, “It’s ok, you will heal fine.’ Then the patient gets home and is alone except for a husband who doesn’t know what to do, and the distress mounts by the minute of what is happening, and what will happen, since the vast majority don’t have a (MDT) waiting at the patient’s home.
The authors of this paper don’t have an issue about whether a patient undergoing mastectomy can go home safely as an outpatient. But after more than a 1000 years of advances in treating cancer, ‘drive by mastectomy’ is what is touted? It is a conclusion of this paper that women universally deserve much better. On another note, one of the conclusions of a paper published in the Int J Surg, 024 Mar 1; 1 10(2): 1392-1401
| [6] | Int J Surg, 024 Mar 1: 1 10 (2): 1392-1401. |
[6]
called, ‘Breast-conserving surgery is associated with a lower incidence of suicide among females with breast cancer in the United State: a population-based retrospective cohort study.’ In the conclusion, the authors state that BCS (breast conserving surgery) was associated with a significantly lower incidence of suicide among females with breast cancer. BCS offers a compelling option for improving the quality of life and self-esteem of patients with cancer and provides a novel perspective on cancer management.”
The point of this paper is that the cardinal sin of the medical-industrial complex, aka the ‘system,’ is they don’t ask and won’t pursue under any circumstances to just push the envelope to its maximum, and that is making it possible to successfully treat breast cancer without surgery, chemotherapy, or radiation. That is where Lavender Breast Centers come in. See our two published papers located on our website at thelavenderproject.net.
And from the CDC (Center for Disease Control) newsroom from Tuesday, April 9, 2024, we have these reasons why women are avoiding mammography. Additionally, multiple factors are intervening in women’s decisions to avoid mammography altogether and this number is increasing.
They are not limited to feeling socially isolated, loss of work, dissatisfaction with life, cost of access to care, lack of transportation, receiving food stamps, and from our own experience, fear of radiation, fear of pain, fear of ending up like their mother or grandmother and lastly, fear that something bad will happen if they find something. In another publication, medstarhealth.org, ‘A new MedStar health national survey finds that 60%-plus of women aged 40 and over are not following the recommendation from the American College of Radiology to have a yearly mammogram. About 21 percent of those surveyed in the same age group say they have never had a mammogram.’
The PubMed database, which accounts for just 12% of scientific papers published on cancer, finds over 3 million papers published on this topic. The NCI (National Cancer Institute) wrote a memorandum saying that breast cancer cases were about 283,000 cases in 2011 and will show a 50% increase by 2030.
As heard at a conference, the former Director of the National Reconnaissance Office, Bruce Carlson, presented an axiom. “If you do things the same way the results will always be the same.” All this reminds the authors of the folk song group called Peter, Paul and Mary back in the 60s who sang, “How many deaths will it take ‘till he knows that too many people have died. The answer my friend is blownin’ in the wind, the answer is blownin’ in the wind.”
The vast majority of people (usually women) never see the horrendous results of breast surgery that made grandma or mother never want to leave the house. Lumpectomy sounds really good vs. mastectomy, as in, “Good I’m not going to lose my breast.” Below are some typical results we see day after day. While treatment at a so-called comprehensive breast center sounds like your breast will come out with nary a scratch, it should be remembered that very few centers have dedicated breast surgeons that have honed their skills so as to do as cosmetically acceptable surgery as possible. The vast majority of breast surgeries are performed by a general surgeon that also does gallbladders, hernias and hemorrhoids, and the breast case gets sandwiched in somehow.
Then too, most surgeons never see that breast cancer patient again after they are healed. At our Lavender Breast Center, patients see the same doctor for decades and is the one who can do surgery or cryoablation. This responsibility placed on the doctors at Lavender dramatically changes the dynamic of patient outcomes if they don’t do well. When we have the capability of omitting surgery, chemotherapy, and radiation and have a successful outcome, if that doesn’t happen and ostensibly the patient’s soul is on your shoulders, you can’t blame anyone but yourself. That is what drives our doctors to hone their skills, so an untoward outcome doesn’t happen. It’s a different mindset than just whacking off a breast that any sloppy surgeon can do. A search to find anyone who killed themselves because of an inguinal hernia incision didn’t reveal anything. That means to us that breast surgery is a very serious undertaking with at times untenable life outcome. Breast surgery is different. Below are some typical examples of so-called state-of-the art surgeries.
Figure 1. Bilateral mastectomies, radial on the right. The surgeon sutured her up like a football.
Figure 2. Two minutes after The Lavender Procedure.
Figure 3. The reason Grandma doesn’t want to leave the house.
Figure 4. One of a number of patients we see now who refuse standard-of care including diagnostic testing because they are afraid of radiation. This tumor took seven years to erode through the skin. Another Black lady was just lost because of the same thing, no mammos because of radiation fear. She was a TV personality. When will people wake up that the system isn’t working?
Figure 5. If encountering a patient with a tumor growing through the skin while rejecting the medical-industrial complex’s answer to surgery, chemotherapy, and radiation was so rare, how is it that we have so many?
Figure 6. We only see a minute fraction of all the women out there. It makes one ask, how many are there that are rejecting help from big cancer centers? We surmise that having comprehensive breast centers on every corner wasn’t the answer after all.
Don’t worry, they say we’ll just reconstruct your breasts.
Figure 7. Which breast is natural and which manmade? And you say this patient should be happy with a little asymmetry as opposed to a flat chest.
Figure 8. This patient was talked into bilateral subcutaneous mastectomies (at a major west coast hospital), with immediate reconstruction for DCIS (ductal carcinoma in situ) in one breast. She is on her third surgery to correct the obvious problem that may never get fixed. It’s our opinion we could have Lavendered that DCIS, and she would have had her breasts intact.
Having seen this admittedly small group of unfortunate women, one must be forced to ask why do they look like this after billions of dollars have been spent trying to optimize care? We think we know the answer, but we can’t say it.
Why the heck not. They ended up like this because they either submitted to standard-of-care that left them disfigured and monumentally disappointed or they ended up like this because they were fed up with all the promises decade after decade with the ‘system’s’ answer of surgery, chemotherapy, and radiation that leaves a tsunami of grief in its wake. Time for change?
Figure 9. If a surgeon says he/she can do a breast conserving procedure, sometimes this is what they mean. This patient must live with this divot in her breast the rest of her life, that is, no low-cut dresses. The surgeon just carved around the tumor leaving this big dent.
Figure 10. This is a self-taught ‘cosmetic lumpectomy’ by our senior surgeon. One of the tenets at Lavender is, if we have to operate, that the patient will not know we were there ten days after or in ten years. If you have a hard time seeing the incision, it’s in the right breast around the nipple (a circumareolar incision).
Figure 11. This kind of surgery needs to be in history books. It’s no wonder women are afraid.
Figure 12. This patient with breast implants had her Lavender Procedure a few days ago. Cryoablation and breast implants poses no problem.
Figure 13. When we talk about humanizing the treatment of breast cancer at Lavender Breast Center, the above photo is integral to what we mean. This is the patient’s husband videotaping the entire procedure. You can just make out the smile on his face as he talks to his wife as well. Prior to the procedure, he was invited and did run his finger through the liquid nitrogen. At other times, he held his wife’s hand. His wife is also the one who dressed in lavender, including painting her nails and lavender ring. She was the one who entered the procedure room and said, “I’m ready for the party”.
With this kind of involvement and also the years long trusting our motto to preserve mind, body, and spirit, everything we had envisioned came to fruition in this patient. This is the kind of outcome we would envision for ALL women who would come to a Lavender Breast Center, another successful Lavender Procedure enabling the patient to avoid surgery, chemotherapy, and radiation. We can accomplish this patient after patient because of a completely different mindset and utilization of a genetics risk test that not only tells a woman’s lifetime risk but when that risk will likely manifest within ten years during her life. Then as the time approaches to appearance of the cancer, we can image the patient as often as necessary to find nascent tumors (5-8mm) because we depend on all FDA approved non-radiation diagnostic modalities that are dismissed by the medical establishment.
This quote and the story were published in LIVESCIENCE, online June 26
th 2024
| [7] | LIVESCIENCE online June 26th, 2024. |
[7]
.
“That particular moment where I saw the kidney in Dr. Nadig's hands — like [it was] extremely powerful to see that," Nicholas said at a press conference Monday (June 24). Within 24 hours of the procedure, Nicholas walked out of the hospital.”
What is this about and does it relate in any way to treat breast cancer? Further, on June 25th while watching the TV game show Wheel of Fortune, one contestant was an African American woman who developed breast cancer at age 26. So what?
Our surgeon, having served on the transplant team (at Loyola in Chicago -1970s), and who directs our Lavender Breast Center, was quick to recognize the correlation between this apparent unheard ‘feat’ of a kidney transplant patient being awake during the procedure, and our Lavender Procedure for killing breast cancer. Whether he knows it or not, that kidney transplant patient will never forget that moment of seeing his ‘new’ kidney and I doubt Dr. Nadig will never forget showing it to him. This kidney transplant was performed at Northwestern University in Chicago. Doing surgical procedures now under local anesthesia and IV sedation is nothing new. In fact, it took our surgeon back to performing a cholecystectomy under local and IV sedation for a patient with COPD. The pulmonary doctor wasn’t afraid of the patient not surviving general anesthesia, but he was very concerned about the possibility of a prolonged weaning from the ventilator, and then the possible need for a tracheostomy. Had our surgeon ever performed a cholecystectomy under local anesthesia? No. Was there any ‘evidence-based medicine’ our current unimpeachable standard that everyone must abide by - no. He just did what he was trained as a surgeon to do, that is, reduce suffering when others couldn’t help. To do what Dr. Nadig and our surgeon did was what some might call, flying by the seat of your pants.’ That’s what surgeons are trained to do, expect the unexpected and be able to surmount any difficulty. We would do that better without meddling functionaries foisting more and more regulations on us.
The contestant on Wheel of Fortune, being African American and having breast cancer at age 26, confirms what we already know about African American women and breast cancer. But the big deal here is nothing revolutionary has been done for them, or for that matter, all women who develop breast cancer. As far as breast cancer is concerned, we still cling to the “assumed righteousness in the way things are done.”
| [8] | Raza Azra, ‘The First Cell,’ 2019; 6-35, Basic Books publishing. |
[8]
This quote is from Dr. Azra Raza’s book, ‘The First Cell.’ That is, the medical-industrial complex embraces the unchanging paradigm of the notion of how to treat cancer, via the slash-poison-burn approach, remains written in stone.
More to the point, there was a paper published by the American College of Surgeons Oncology Group in 2009
| [9] | Garneski SaLly, African American women still have poorer breast cancer outcomes, JACS, 2009. |
[9]
that specifically looked at breast cancer in African American women and found a startling revelation. That is, breast cancer in African American women presented at a much earlier age (in their thirties) and was significantly more aggressive, being so-called triple negative. So what? The so what is, how unconscionable is it for some edict to come out by some appointed overseeing ‘central planning’ committee that mammography shouldn’t be initiated until age 50? This lasted for years and only recently has the edict been modified to begin mammography at 40. The ACSOG recommended beginning screening for this group at around 30 years of age. This is something the ‘system’ can’t and won’t do. Why? Because radiation is cumulative and for how long do we do mammograms every six months on a high-risk woman? The ‘system’ won’t pay for all those mammograms or MRI’s. Of course, we will never know how many African American women in particular succumbed to this nonsense of their mammograms being delayed until age 50. Going back to the Hippocratic oath all physicians took or should have taken to practice the ART OF MEDICINE:
“I swear by Apollo the physician, and Aesculapius the surgeon, likewise Hygeia and Panacea, and call all the gods and goddesses to witness, that I will observe and keep this underwritten oath, to the utmost of my power and judgment. I will reverence my master who taught me the art.”
It also has something to specifically say ‘do no harm.’ When a ’central planner’ lays down a law (of course, they say it’s not a law), but Medicare and insurance companies use it to justify not paying for mammograms other than what is ‘allowed by the central planner,’ and some women may have died because of it, then that is cause for real concern and policy change.
That some entity can interfere with the sacred bond between a doctor and his/her patient and how the doctor practices his/her art, is a travesty. It raises the question of what kind of doctors are we creating that allow a central planner to authoritatively direct their care without raising a whimper? Has the ‘art’ of medicine vanished in lieu of the edicts of the ‘central planner? Of course, the ‘central planner’ has just about interfered with every aspect of medical care with one objective, to delay and deny proper care and reap profits. Now when about 80% of physicians are employed by either a hospital, HMO or private equity firm that dictates how many patients a doctor will see, and how much time is allotted, and worse, what care can be prescribed, that’s a real problem.
Getting back to the transplant patient. After the procedure, with the patient still on the operating table, the surgical team gathered around for a photo. Now clearly this is not standard-of-care for a photo to be taken, and then in addition to making it public.
Should Dr. Nadig and his assistants be brought before some disciplinary committee or better yet be investigated by the Illinois Board of Medicine? Did they overstep their bounds? I think we can safely say they pushed the envelope in not only performing the kidney transplant under local anesthesia and IV sedation, but then the photo, and then going public. Why did they do this? We feel they did it to light the way that a procedure of this type can be performed as they did it with its attendant benefits, and the patient left the hospital within 24 hours (also unheard of). What’s the lesson here we and all Medical Boards should be learning? That medicine is an art. Those people who become doctors (especially surgeons), have spent the majority of their lives honing their skills that permit something as groundbreaking (totally outside standard-of-care) as what Dr. Nadig and his team accomplished. For that they should be lauded. Aren’t the results what matters?
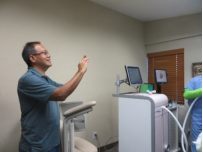
The kidney transplant patient’s recognition of the “extremely powerful moment” of Dr. Nadig showing him his new kidney that we are sure he will never forget, relates directly to a phenomenon we encountered with patients seeing their breast cancer killed via cryoablation (aka Lavender Procedure), under real time ultrasound, as the patients are fully awake. Does the fact that the patient is fully awake with her significant other by her side seeing her cancer being killed in real time have lasting meaning? We as physicians are fully aware of all the consequences that breast cancer portends. Those include, fear of death, fear that they won’t see their children grow up, fear that their husband might leave, anxiety of being disfigured (some say mutilated), fear that the cancer might return, loss of self-image (losing their hair), and bankruptcy just to name a few.
In 2014 the team at then Visionary Breast Center performed their first killing of an invasive breast cancer with the patient fully awake under only local anesthesia using liquid nitrogen, aka The Lavender Procedure. Not only that, but to humanize the procedure as much as possible, the patient’s significant other was allowed in the procedure room able to hold the patient’s hand.
They could ask questions and actually see the cancer being killed on real-time ultrasound. This instead of the relative or friend sitting in a cold hospital waiting room with other anxious people wanting to know what’s happening to their loved one. And before the procedure started, they saw the liquid nitrogen with the cloud of nitrogen it creates being transferred from the large dewar to the smaller cannister that is housed in the cryo machine. They could (if desired) actually run their fingers through the liquid nitrogen. It actually has an unanticipated warm and almost gritty feeling. The entire process, to use a term from back in the 1960s, was almost a ‘happening.’ In fact, one patient entered the procedure room dressed in lavender including painted nails and said, “I’m ready for the party.” How many patients do you know that enter a facility for definitive treatment of breast cancer and spontaneously say that? None. Instances like that should have alerted us that something different and profound was going on.
That something different that we didn’t realize until years had passed in follow-up was a total discharging of any hint of anxiety about anything related to their breast cancer outcome, that we typically see in standard-of-care patients as stated above.
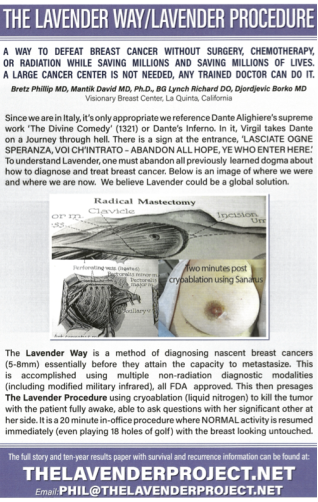
Before we continue, let’s look at an image of radical breast surgery. This was typically carried out for a hundred years up until 1979 when Umberto Veronesi, MD, (R. I. P.) founder of Istituto Europeo di Oncologia in Milan, Italy, published his seminal paper on lumpectomy vs mastectomy that showed no difference in outcomes. Our poster was invited and exhibited at the EBCC (European Breast Cancer Conference) in Milan, Italy March 2024. You will see no incision on the breast. All that is left is the minute hole at the entrance site of the cryo probe (3mm). That is covered with a little dab of antibiotic ointment, no sutures. The image toward the left is the radical surgery (which continues to alienate women to this day), and the image on the right is about 2 minutes after The Lavender Procedure with the breast looking untouched.
We called it The Lavender Procedure because one of our first patients remarked that she was hungry right after. She wanted to walk across the street to Lavender Bistro in La Quinta, CA. Within fifteen minutes she was dining on lobster salad and toasting with a glass of chardonnay with her significant other as NONE of the evils of breast cancer had reached her. She is now over ten years out and cancer-free. The poster follows. The reader can decide what happened at this conference to our poster. Look at the poster, then come back to realize what happened. Redacted?
Figure 14. Check our poster below and you will see they redacted all the writing. Why would they do that?
Figure 15. Poster from the medical conference in Milan, Italy 2024.
This phenomenon of reversing or eliminating the horrific things that breast cancer portends (fear, anxiety, dread, etc.) is one of the many benefits of cryoablation (Lavender). In our 10 years of follow up, here are the things we have learned that cryoablation can offer. These are in no particular order.
1. Prolonged disease-free interval. We intentionally never say ‘cure’ because breast cancer does what it does despite our best efforts. We have seen local recurrences 20 years out. However, having cancer-free patients ten years out from Lavender with the breast looking untouched we believe is noteworthy.
2. Lavender can be used to kill local recurrences to save the breast when standard-of-care says mastectomy after lumpectomy and external beam radiation.
3. The procedure is performed with the patient fully awake with their significant other by their side. Both are able to ask questions, and both can see the cancer being killed. This scenario is instead of an impersonal hospital waiting room with prolonged waiting as to what is happening to their loved one.
4. Lavender is ideal for very frail or elderly patients, for instance those who use a cane for walking. It eliminates the risk of nerve injury from axillary lymph node dissection.
5. While Lavender can be performed on larger tumors (just to save the breast), chemotherapy can still be done. Cryoablation doesn’t eliminate chemotherapy or, for that matter, radiation.
6. While it is possible to tackle larger tumors (3cm), ideally it should be performed on nascent tumors (5-8 mm) before many have the capacity to metastasize. Even with metastasis, the breast can be saved.
7. In planning a Lavender Procedure many things are taken into consideration. Tumor analysis to disclose the true aggressiveness of the tumor or not, family history, tumor size, is the patient fully ambulatory or restricted somehow, are all important.
8. Multiple tumors can be killed in one treatment session.
9. Cost savings to a country, not to mention the better result for its women, would be in the hundreds of millions to billons yearly.
10. Finding nascent tumors before they attain the capacity to metastasize is left up to the Lavender Way which then presages or enables the Lavender Procedure. That is first identifying the patient’s true lifetime risk for breast cancer, and the genetics test also shows within ten years of the patient’s life when that risk will likely manifest. It looks at age related SNPs (Single Nucleotide Polymorphisms) in the DNA molecule (3). Depending on this result, that risk test determines when and what non-radiation diagnostic modalities are used. Non-radiation diagnostic modalities used include modified military infrared, a pressure sensing device that can identify hard vs soft masses at 5mm, ultrasound with elastography and a device that can perform liquid biopsy by sucking out atypical cells or dissociated malignant cells lying in the ducts. For instance, a true case was a patient whose mother died of breast cancer at age 57 and she was now 50. She was imaged twice yearly starting at age 50 and a 4 mm invasive cancer was found three years before mammography or MRI identified it. The infrared image could not pinpoint the location. We had to wait for mammography to catch up. But the infrared image found it first.
11. Mammography is used as required and to specifically identify the location of the tumor, likewise MRI. But they are not the main modalities used to survey the patient. In the future, the use of the genetics test, physical exam, IR, and ultrasound would be used instead of yearly mammography.
12. Cost is something many people have been trying to reduce while at the same time providing outstanding care. Lavender has been performed for $2,500.00 USD vs. over 200K for standard-of-care requiring 30-40% of the time a second or third surgery for ‘tumor at the margins,’ prolonged chemotherapy and radiation.
13. Importantly, Lavender (if done correctly) eliminates surgery, chemotherapy and radiation all in the 20 minute in-office procedure (outside the hospital) with all patients, including a 91-year-old resuming normal activity immediately with the breasts looking untouched.
14. We believe that Lavender can be used globally (any trained doctor can do it), therefore, a huge cancer center is NOT needed. Lavender is an ideal tool in developing countries where perhaps resources are at a premium.
15. The entire process is accomplished totally outside any insurance company or central planner directive. Lavender restores the sacred relationship between the doctor and patient. Ideally, the patient sees the same doctor for decades, not a different one at every visit and no NPs (Nurse Practitioners) or PAs (Physician Assistants).
Lavender is VERY DISRUPTIVE (to the medical establishment-- not the patient) and generally those in place universally don’t want to be displaced, so it becomes very difficult for Lavender and what it offers to see the light of day when the medical-industrial complex rules the roost. Preventing women from realizing the benefits of Lavender by its simple dismissal is unconscionable. A couple more quotes from Dr. Raza’s book are in order.
From page 17, “Too many lives are being lost because of our own unshakable hubris, convinced as we are that we possess the power to untangle the intricacies of as complex disease as cancer.”
“Liberate us from the confident complacency of assumed righteousness in the way things are done, liberate us from the mental cages we have inadvertently imprisoned ourselves in, our lives are at stake.” And, from page 10, “The disease is fantastically complex. More fantastic is the reductionist conceit that targeting a single genetic abnormality with a single drug will be curative.” And, from page 6, “With minor exceptions, a protocol of surgery, chemotherapy, and radiation – the slash-poison-burn approach to treating cancer – remains unchanged. It is an embarrassment. Equally embarrassing is the arrogant denial of that embarrassment.”
It's apropos to revisit some writings of Dr. Vincent T. DeVita Jr., whose son died of cancer which led him on a quest to make things better. His experience should open our eyes to just how innovation takes place and what hinders it, especially in a disease like cancer. Taken from an article published in the New Yorker on December 7th, 2015, “The breakthroughs made at the N.C.I. in the nineteen-sixties and seventies were the product of a freewheeling intellectual climate.
The social conditions that birthed a new idea in one place, impeded the spread of that same idea in another.
When the Cancer researcher Bernard Fisher (R.I.P.) did a study showing that there was no difference in outcome between radical mastectomies and the far less invasive lumpectomies, he called DeVita in distress. He couldn’t get the study published.” This is a sterling example of people’s uptight and arrogant exclusionary nature with their reluctance to change even when positive results are staring them in the face.
This example of Fisher’s problem getting his study published points to another problem of American cancer researchers. What isn’t mentioned in De Vita’s article or in the publication by Fisher is that Fisher’s trial was based totally on Umberto Veronese’s landmark article published in 1979. Simply by our American researchers embracing a well-done study by the Italians and getting this new, less disfiguring treatment out there immediately, we had to do yet another six-year long re-do. Even when the results verified Umberto’s, it took about twenty years for lumpectomy to be accepted. Now with functionaries leading the way with ever mounting regulations and insistence on ‘evidence-based medicine’ as the only way, no wonder women are continually sacrificed.
DeVita further states, “Clinical progress against a disease as wily and dimly understood as cancer, DeVita argues, happens when doctors have the freedom to try unorthodox things - and he worries we have lost sight on that fact.” Another sterling example is his association with Dr. Freireich at the N.C.I. (National Cancer Institute). This is how intrathecal injections of an antibiotic came to save the lives of people with leukemia and pseudomonas meningitis. “The first time Freireich told me to do it, I held up the vial and showed him the label, thinking that he’d possibly missed something. It said right there, Do Not Use Intrathecally. I said. Freireich glowed at me and pointed a long bony finger in my face “DO IT.” “He barked. I did it, though I was terrified, but it worked every time,” No evidence-based medicine here.
Concerning breast cancer specifically, DeVita writes, “Years ago, women with all stages of breast cancer had radical mastectomies, leaving just tissue over bone and a painful swollen arm. Then they died. Look how far we’ve come.”
The question now is, have we come far enough to see the light, or are we reverting to ‘getting it all’ with oncoplastic surgery, with the simultaneous incrimination of cryoablation and advanced non-radiation diagnostic modalities?
In more recent times, Robert F Kennedy Jr. (now Secretary of HHS) refers in his book ‘The Real Anthony Fauci,’ one man’s authority to do what Kennedy calls “agency capture.” That is, one man who has the authority to appoint members of the FDA (Food and Drug Administration) and CDC (Center for Disease Control) to entrusted positions and at the same time tell them what to do and what not to do. Kennedy spells this out very clearly in his speech before members of Hillsdale College (available online). This authority is a monumental example of misuse of public trust in our most sacred institutions.
Secretary Kennedy also makes reference in his speech at Hillsdale College to the drug companies that gave us the opioid epidemic that killed 68,000 people per year. That’s more than the 58,000 killed during the twenty-year war with Vietnam. And the drug companies knew it. He says that these are bad people that have paid over 35 billion dollars in criminal fees during the past ten years, and if you think they found Jesus when it comes to vaccines, you are mistaken. THE SAME CAN BE SAID ABOUT BREAST CANCER.