Pseudomonas aeruginosa is an opportunistic pathogen responsible for severe hospital-acquired infections, including ventilator-associated pneumonia. Due to its biofilm-forming ability and antimicrobial resistance, it presents a significant public health challenge. This study assessed the efficacy of selected antibiotics against P. aeruginosa isolates associated with respiratory devices from regional referral hospitals in mainland Tanzania. A cross-sectional study was conducted in 2024, in which samples were collected from January to March in Emergency wards, Intensive care units, and Medical wards. Samples collected included water from the Oxygen humidification container, swab samples from reusable masks and the connectors. Laboratory analysis using standard microbiological techniques and PCR were employed for isolation and confirmation of P. aeruginosa. Antimicrobial susceptibility testing was performed using the Kirby-Bauer disc diffusion method. Out of the collected samples (N=231), P. aeruginosa was detected at an overall prevalence of 14.7% (n=34). The analysis of prevalence by sample type revealed that water for humidification had the highest prevalence of 30.6%, followed by respirators at 8.2% and the least in connectors at 3.5%. P. aeruginosa showed a notable resistance towards gentamycin, followed by meropenem, and the least resistance was shown in ceftazidime. On the other hand, P. aeruginosa were fully susceptible to piperacillin-tazobactam combination. A very small proportion of isolates demonstrated multidrug resistance (MDR). Despite the noted resistance majority of the antibiotics used to treat respiratory tract infection (RTIs) in this study showed significant efficacy.
| Published in | Medicine and Health Sciences (Volume 2, Issue 2) |
| DOI | 10.11648/j.mhs.20260202.13 |
| Page(s) | 86-96 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Pseudomonas aeruginosa Detection, Respiratory Tract Infection, Antibiotic Resistance, Oxygen Therapy Devices
Condition | Temperature (℃) | Time (minutes) | No. of cycles |
|---|---|---|---|
Initial denaturation | 96 | 5 | 1 |
Denaturation | 96 | 1 | 40 |
Annealing | 55 | 1 | 40 |
Extension | 72 | 1 | 40 |
Final extension | 72 | 10 | 1 |
Hospital codes | P. aeruginosa | χ2 | p-value | |
|---|---|---|---|---|
Absent | Present | |||
n (%) | n (%) | |||
RRH001 | 6 (85.7) | 1 (14.3) | 25.637 | 0.375 |
RRH002 | 8 (88.9) | 1 (11.1) | ||
RRH003 | 7 (100) | 0 (0) | ||
RRH004 | 5 (62.5) | 3 (37.5) | ||
RRH005 | 6 (100) | 0 (0) | ||
RRH006 | 6 (75) | 2 (25) | ||
RRH007 | 9 (100) | 0 (0) | ||
RRH008 | 6 (75) | 2 (25) | ||
RRH009 | 8 (88.9) | 1 (11.1) | ||
RRH010 | 5 (62.5) | 3 (37.5) | ||
RRH011 | 4 (66.7) | 2 (33.3) | ||
RRH012 | 7 (87.5) | 1 (12.5) | ||
RRH013 | 9 (100) | 0 (0) | ||
RRH014 | 9 (100) | 0 (0) | ||
RRH015 | 6 (85.7) | 1 (14.3) | ||
RRH016 | 9 (100) | 0 (0) | ||
RRH017 | 6 (75) | 2 (25) | ||
RRH018 | 7 (77.8) | 2 (22.2) | ||
RRH019 | 8 (88.9) | 1 (11.1) | ||
RRH020 | 8 (88.9) | 1 (11.1) | ||
RRH021 | 7 (87.5) | 1 (12.5) | ||
RRH022 | 7 (87.5) | 1 (12.5) | ||
RRH023 | 7 (77.8) | 2 (22.2) | ||
RRH024 | 6 (85.7) | 1 (14.3) | ||
RRH025 | 5 (55.6) | 4 (44.4) | ||
RRH026 | 5 (100.0) | 0 (0) | ||
RRH027 | 7 (77.8) | 2 (22.2) | ||
RRH028 | 6 (100) | 0 (0) | ||
RRH029 | 8 (100) | 0 (0) | ||
Total | 197 (85.3) | 34 (14.7) | ||
Unit name | P. aeruginosa isolation [n (%)] | |||
|---|---|---|---|---|
Positive | Negative | χ2 | p-value | |
EMD | 11 (13.9) | 68 (86.1) | 1.371 | 0.523 |
ICU | 14 (18.4) | 62 (81.6) | ||
WARD | 9 (11.8) | 67 (88.2) | ||
TOTAL | 34 (14.7) | 197 (85.3) | ||
Unit name | P. aeruginosa isolates | |||
|---|---|---|---|---|
n | % | χ2 | P-value | |
EMD | 11 | 32.3 | 1.371 | 0.523 |
ICU | 14 | 41.2 | ||
WARD | 9 | 26.5 | ||
TOTAL (N) | 34 | 100 | ||
Sample type | P. aeruginosa | |||
|---|---|---|---|---|
Absent n (%) | Present n (%) | X2 | p= value | |
Connector (CS) | 82 (96.5) | 3 (3.5) | 27.599 | <0.0001 |
Water for humidification (WS) | 59 (69.4) | 26 (30.6) | ||
Respirator/reusable Masks (RS) | 56 (91.8) | 5 (8.2) | ||
Hospital code | Susceptible (S) (n) | Intermediate (I) (n) | Resistance (R) (n) | MDR status |
|---|---|---|---|---|
RRH001 | 5 | 0 | 1 | Not MDR |
RRH002 | 5 | 1 | 0 | Not MDR |
RRH003 | 2 | 0 | 4 | MDR |
RRH006 | 11 | 0 | 1 | Not MDR |
RRH008 | 5 | 1 | 0 | Not MDR |
RRH009 | 6 | 0 | 0 | Not MDR |
RRH010 | 24 | 0 | 0 | Not MDR |
RRH011 | 10 | 0 | 2 | Not MDR |
RRH012 | 6 | 0 | 0 | Not MDR |
RRH015 | 6 | 0 | 0 | Not MDR |
RRH018 | 12 | 0 | 0 | Not MDR |
RRH017 | 11 | 1 | 0 | Not MDR |
RRH020 | 6 | 0 | 0 | Not MDR |
RRH021 | 6 | 0 | 0 | Not MDR |
RRH022 | 4 | 0 | 2 | Not MDR |
RRH023 | 6 | 0 | 0 | Not MDR |
RRH024 | 5 | 1 | 0 | Not MDR |
RRH025 | 23 | 1 | 0 | Not MDR |
RRH027 | 5 | 1 | 0 | Not MDR |
AMR | Antimicrobial Resistance |
ATCC | American Type Culture Collection |
CA | Cetrimide Agar |
CDC | Center for Disease Control |
CLSI | Clinical and Laboratory Standards Institute |
EMD | Emergence Department |
ESKAPE | Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa and Enterobacter Spp. |
HAI | Hospital Acquired Infections |
ICU | Intensive Care Unit |
MDR | Multi Drug Resistance |
MHA | Mueller Hinton Agar |
PCR | Polymerase Chain Reaction |
RRH | Regional Referral Hospital |
NA | Nutrient Agar |
RTI | Respiratory Tract Infection |
SPP | Species |
SPSS | Statistical Product and Service Solutions |
TAE | Tris-acetate-EDTA |
TMDA | Tanzania Medicines and Medical Devices Authority |
TSB | Tryptose Soy Broth |
USP | United State Pharmacopoeia |
USPNF | United States Pharmacopoeia-National Formulary |
| [1] | Gellatly SL, Hancock REW. Pseudomonas aeruginosa: New insights into pathogenesis and host defenses. Pathog Dis. 2013; 67(3): 159–73. |
| [2] | Stover CK, Pham XQ, Erwin AL, Mizoguchi SD, Warrener P, Hickey MJ, et al. Complete genome sequence of Pseudomonas aeruginosa PAO1, an opportunistic pathogen. Nature. 2000; 406(6799): 959–64. |
| [3] | Denissen J, Reyneke B, Waso-Reyneke M, Havenga B, Barnard T, Khan S, et al. Prevalence of ESKAPE pathogens in the environment: Antibiotic resistance status, community-acquired infection and risk to human health. Int J Hyg Environ Health. 2022; 244(July): 114006. |
| [4] | Abushaheen MA, Muzaheed, Fatani AJ, Alosaimi M, Mansy W, George M, et al. Antimicrobial resistance, mechanisms and its clinical significance. Disease-a-Month. 2020; 66(6): 1–21. |
| [5] | Augustine FF, Mgaya XM, Yahya SA, Niccodem EM, Matee MI. An alarming prevalence of multidrug-resistant (MDR) ESKAPE pathogens and other drug-resistant bacteria isolated from patients with bloodstream infections hospitalized at Muhimbili National Hospital in Dar es Salaam, Tanzania. Ger J Microbiol. 2023; 3(3): 7–15. |
| [6] | Cole SJ, Records AR, Orr MW, Linden SB, Lee VT. Catheter-associated urinary tract infection by Pseudomonas aeruginosa is mediated by exopolysaccharide-independent biofilms. Infect Immun. 2014; 82(5): 2048–58. |
| [7] | Kollef MH, Chastre J, Fagon JY, François B, Niederman MS, Rello J, et al. Global prospective epidemiologic and surveillance study of ventilator-associated pneumonia due to pseudomonas aeruginosa. Crit Care Med. 2014; 42(10): 2178–87. |
| [8] | Alem K. Prevalence of bacterial pneumonia among HIV- Seropositive patients in East Africa : Review Prevalence of bacterial pneumonia among HIV-Seropositive patients in East Africa : Review. Cogent Med. 2021; 8(1). |
| [9] | Josephs-Spaulding J, Singh O V. Medical Device Sterilization and Reprocessing in the Era of Multidrug-Resistant (MDR) Bacteria: Issues and Regulatory Concepts. Front Med Technol. 2020; 2(February): 1–15. |
| [10] | Moradali MF, Ghods S, Rehm BHA. Pseudomonas aeruginosa lifestyle: A paradigm for adaptation, survival, and persistence. Front Cell Infect Microbiol. 2017; 7(FEB). |
| [11] | Jasim AK, Hussein AA. Detection Genotyping Virulence Factor among Pseudomonas aeruginosa Isolated from Burns Patients. Int J Adv Multidiscip Res Stud. 2023; 3(4): 1209–14. |
| [12] | Vos DDE, Lim A, Pirnay J, Struelens M, Vandenvelde C, Duinslaeger LUC, et al. Direct Detection and Identification of Pseudomonas aeruginosa in Clinical Samples Such as Skin Biopsy Specimens and Expectorations by Multiplex PCR Based on Two Outer Membrane Lipoprotein Genes, oprI and oprL. 1997; 35(6): 1295–9. |
| [13] | Limbago JSLIib and ALB et al. CLSI, performance standards for antimicrobial susceptibility testing 33rd Edition. Clinical and Laboratory Standards Institute,. 2024. 1–416 p. |
| [14] | Interim S, Announcement R, Tests S. 71 sterility tests. 2016; 34(6): 1–12. |
| [15] | Abdullahi R, Lihan S, Carlos BS, Bilung ML, Mikal MK, Collick F. Detection of opr L gene and antibiotic resistance of Pseudomonas aeruginosa from aquaculture environment. 2013; 3(6): 148–52. |
| [16] | Vidal-Cortés P, Campos-Fernández S, Cuenca-Fito E, del Río-Carbajo L, Fernández-Ugidos P, López-Ciudad VJ, et al. Difficult-to-Treat Pseudomonas aeruginosa Infections in Critically Ill Patients: A Comprehensive Review and Treatment Proposal. Antibiot (Basel, Switzerland). 2025 Feb; 14(2). |
| [17] | Litwin A, Rojek S, Gozdzik W, Duszynska W. Pseudomonas aeruginosa device associated – healthcare associated infections and its multidrug resistance at intensive care unit of University Hospital: polish, 8.5-year, prospective, single-centre study. BMC Infect Dis. 2021; 21(1): 4–11. |
| [18] | Shane AL, Gonzalez MD, Roy AM, Preidis GA, Woodworth MH. State-of-the-Art Review: Infectious Diarrhea. Clin Infect Dis. 2025 Nov; 81(5): e250–62. |
| [19] | La Fauci V, Costa GB, Facciolà A, Conti A, Riso R, Squeri R. Humidifiers for oxygen therapy: what risk for reusable and disposable devices J Prev Med Hyg. 2017; 58(2): E161 |
| [20] | Serrano-Mayorga CC, Degree M, Olivella-Gomez J, Torres A, Martin-Loeches I, Luis, et al. P-286. Prevalence of Pseudomonas aeruginosa in patients with ICU-related respiratory Infections: A secondary analysis of the European Network for ICU-Related Respiratory Infections (ENIRRIs). Open Forum Infect Dis. 2025 Jan; 12(Supplement_1). |
| [21] | Thaden JT, Park LP, Maskarinec SA, Ruffin F, Fowler VG, Van Duin D. Results from a 13-year prospective cohort study show increased mortality associated with bloodstream infections caused by pseudomonas aeruginosa compared to other bacteria. Antimicrob Agents Chemother. 2017; 61(6). |
APA Style
Mtenga, A. B., Kasekwa, E. E., Fimbo, A. M., Mwambene, S. J., Makonope, R. E., et al. (2026). Efficacy of Antibiotics Against Pseudomonas aeruginosa Isolated from Respiratory Devices in Tanzania. Medicine and Health Sciences, 2(2), 86-96. https://doi.org/10.11648/j.mhs.20260202.13
ACS Style
Mtenga, A. B.; Kasekwa, E. E.; Fimbo, A. M.; Mwambene, S. J.; Makonope, R. E., et al. Efficacy of Antibiotics Against Pseudomonas aeruginosa Isolated from Respiratory Devices in Tanzania. Med. Health Sci. 2026, 2(2), 86-96. doi: 10.11648/j.mhs.20260202.13
@article{10.11648/j.mhs.20260202.13,
author = {Adelard Bartholomew Mtenga and Elizabeth Erasto Kasekwa and Adam Mitangu Fimbo and Saxon Joseph Mwambene and Revocatus Evarist Makonope and Kissa Watson Mwamwitwa and Raphael Zozimus Sangeda and Danstan Hipolite Shewiyo},
title = {Efficacy of Antibiotics Against Pseudomonas aeruginosa Isolated from Respiratory Devices in Tanzania},
journal = {Medicine and Health Sciences},
volume = {2},
number = {2},
pages = {86-96},
doi = {10.11648/j.mhs.20260202.13},
url = {https://doi.org/10.11648/j.mhs.20260202.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.mhs.20260202.13},
abstract = {Pseudomonas aeruginosa is an opportunistic pathogen responsible for severe hospital-acquired infections, including ventilator-associated pneumonia. Due to its biofilm-forming ability and antimicrobial resistance, it presents a significant public health challenge. This study assessed the efficacy of selected antibiotics against P. aeruginosa isolates associated with respiratory devices from regional referral hospitals in mainland Tanzania. A cross-sectional study was conducted in 2024, in which samples were collected from January to March in Emergency wards, Intensive care units, and Medical wards. Samples collected included water from the Oxygen humidification container, swab samples from reusable masks and the connectors. Laboratory analysis using standard microbiological techniques and PCR were employed for isolation and confirmation of P. aeruginosa. Antimicrobial susceptibility testing was performed using the Kirby-Bauer disc diffusion method. Out of the collected samples (N=231), P. aeruginosa was detected at an overall prevalence of 14.7% (n=34). The analysis of prevalence by sample type revealed that water for humidification had the highest prevalence of 30.6%, followed by respirators at 8.2% and the least in connectors at 3.5%. P. aeruginosa showed a notable resistance towards gentamycin, followed by meropenem, and the least resistance was shown in ceftazidime. On the other hand, P. aeruginosa were fully susceptible to piperacillin-tazobactam combination. A very small proportion of isolates demonstrated multidrug resistance (MDR). Despite the noted resistance majority of the antibiotics used to treat respiratory tract infection (RTIs) in this study showed significant efficacy.},
year = {2026}
}
TY - JOUR T1 - Efficacy of Antibiotics Against Pseudomonas aeruginosa Isolated from Respiratory Devices in Tanzania AU - Adelard Bartholomew Mtenga AU - Elizabeth Erasto Kasekwa AU - Adam Mitangu Fimbo AU - Saxon Joseph Mwambene AU - Revocatus Evarist Makonope AU - Kissa Watson Mwamwitwa AU - Raphael Zozimus Sangeda AU - Danstan Hipolite Shewiyo Y1 - 2026/03/26 PY - 2026 N1 - https://doi.org/10.11648/j.mhs.20260202.13 DO - 10.11648/j.mhs.20260202.13 T2 - Medicine and Health Sciences JF - Medicine and Health Sciences JO - Medicine and Health Sciences SP - 86 EP - 96 PB - Science Publishing Group SN - 3070-6300 UR - https://doi.org/10.11648/j.mhs.20260202.13 AB - Pseudomonas aeruginosa is an opportunistic pathogen responsible for severe hospital-acquired infections, including ventilator-associated pneumonia. Due to its biofilm-forming ability and antimicrobial resistance, it presents a significant public health challenge. This study assessed the efficacy of selected antibiotics against P. aeruginosa isolates associated with respiratory devices from regional referral hospitals in mainland Tanzania. A cross-sectional study was conducted in 2024, in which samples were collected from January to March in Emergency wards, Intensive care units, and Medical wards. Samples collected included water from the Oxygen humidification container, swab samples from reusable masks and the connectors. Laboratory analysis using standard microbiological techniques and PCR were employed for isolation and confirmation of P. aeruginosa. Antimicrobial susceptibility testing was performed using the Kirby-Bauer disc diffusion method. Out of the collected samples (N=231), P. aeruginosa was detected at an overall prevalence of 14.7% (n=34). The analysis of prevalence by sample type revealed that water for humidification had the highest prevalence of 30.6%, followed by respirators at 8.2% and the least in connectors at 3.5%. P. aeruginosa showed a notable resistance towards gentamycin, followed by meropenem, and the least resistance was shown in ceftazidime. On the other hand, P. aeruginosa were fully susceptible to piperacillin-tazobactam combination. A very small proportion of isolates demonstrated multidrug resistance (MDR). Despite the noted resistance majority of the antibiotics used to treat respiratory tract infection (RTIs) in this study showed significant efficacy. VL - 2 IS - 2 ER -
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania;Department of Pharmaceutical Microbiology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Department of Pharmaceutical Microbiology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
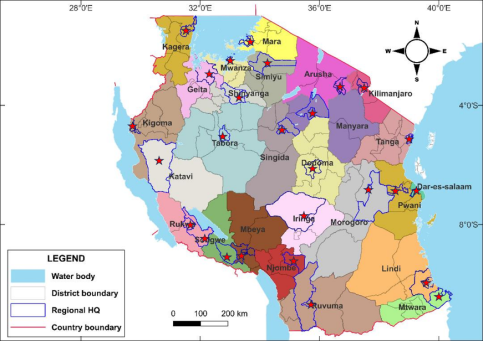
Figure 1. A map of Tanzania showing the locations of all RRH where samples were collected.
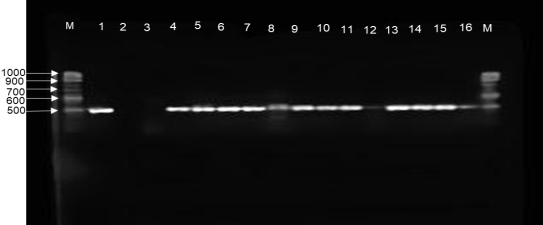
Figure 2. Agarose gel electrophoresis of PCR-amplified Oprl gene from P. aeruginosa isolates, lane M; markers, lane 1; positive control, lane 2; negative control and lane 3-16; isolate samples.
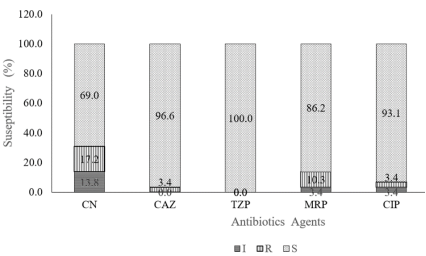
Figure 3. The Antimicrobial susceptibility profile of P. aeruginosa against six different antibiotics for treatment of RTIs in Tanzania.
Information

