Background: Tuberculosis (TB), caused by Mycobacterium tuberculosis (MTB), is one of the most common infectious diseases, especially in countries with limited healthcare resources. Early and accurate diagnosis is essential to curb its spread, and loop-mediated isothermal amplification (LAMP) is a rapid, cost-effective, and reliable molecular diagnostic method. Objective: The objective of this study was to evaluate the performance of TB-LAMP as a rapid and reliable diagnostic tool for pulmonary TB and compare it with direct smears and Gene Xpert, using culture as a reference. Materials: Between February and July 2025, a total of 397 patients (227 men and 170 women) were enrolled in the study. Samples were tested by smear microscopy, culture, Xpert MTB/RIF, and TB-LAMP. Results: Of the 397 patients, 84 (21.15%) were culture-positive. Among culture-positive patients, 81 (96.4%) were positive by Gene Xpert, 69 (82.1%) by TB-LAMP, and 49 (58.3%) by direct smear microscopy. Using culture as the reference standard, the specificity, positive predictive value (PPV), and negative predictive value (NPV) of the TB-LAMP assay were 82.1% (73.9%–90.3%), 99.0% (97.9%–100%), 95.8% (91.2%–100%), and 95.4% (93.1%–97.7%), respectively. Conclusions: The TB-LAMP assay exhibits high diagnostic accuracy for the detection of Mycobacterium tuberculosis, making it a rapid, cost-effective, and reliable alternative to conventional methods, especially in resource-poor settings.
| Published in | Medicine and Health Sciences (Volume 2, Issue 3) |
| DOI | 10.11648/j.mhs.20260203.12 |
| Page(s) | 115-120 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Tuberculosis (TB), Mycobacterium Tuberculosis (MTB), Gene Xpert, TB-LAMP
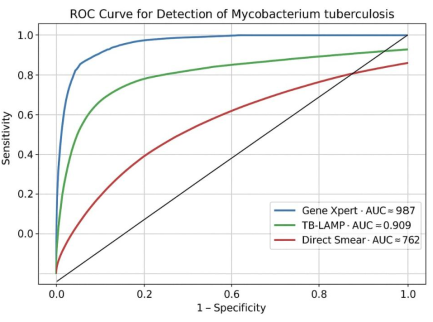
Test | Sensitivity% [95% Cl] | Specificity% [95% Cl] | PPV% [95% Cl] | NPV% [95% Cl] |
|---|---|---|---|---|
Gene xpert | (92.4–100%) 96.4 | (99.1–100%) 99.7 | (96.4–100%) 98.8 | (97.9–100%) 99.0 |
TB-LAMP | (73.9–90.3%) 82.1 | (97.9–100%) 99.0 | (91.2–100%) 95.8 | (93.1–97.7%) 95.4 |
Direct smear | (47.8–68.8%) 58.3 | (91.6–96.8%) 94.2 | (62.5–83.7%) 73.1 | (86.1–92.7%) 89.4 |
AUC | Area Under Curve |
CI | Confidence Intervals |
LPA | Line Probe Assay |
TB-LAMP | Loop-mediated Isothermal Amplification |
L-J | Lowenstein-Janssen Medium |
MDR-MTB | Multidrug-Resistant M. Tuberculosis |
MTB | Mycobacterium Tuberculosis |
NPV | Negative Predictive Value |
NTM | Nontuberculous Mycobacteria |
PPV | Positive Predictive Value |
ROC | Receiver Operating Characteristic |
TB | Tuberculosis |
WHO | World Health Organization |
| [1] | I. Khalil, "Challenges in diagnosing primary tubercular chorioretinitis and ocular tuberculosis in resource-limited settings of Bangladesh," Indian Journal of Tuberculosis, vol. 72, pp. S80–S84, 2025. |
| [2] | V. Mittal, M. Kumar, and A. K. Singh, "TB LAMP assay, a beneficial tool for the diagnosis of Tubercular meningitis in resource-limited settings," The Journal of Infection in Developing Countries, vol. 18, no. 03, pp. 435–440, 2024. |
| [3] | I. K. Matar, Z. Dong, and C. F. Matta, "Exploring the chemical space of mycobacterial oxidative phosphorylation inhibitors using molecular modeling," ChemMedChem, vol. 19, no. 22, e202400303, 2024. |
| [4] | A. Allué-Guardia, J. I. García, and J. B. Torrelles, "Evolution of drug-resistant Mycobacterium tuberculosis strains and their adaptation to the human lung environment," Frontiers in Microbiology, vol. 12, 612675, 2021 |
| [5] | D. Kaushal, D. K. Singh, and S. Mehra, "Immune responses in lung granulomas during MTB/HIV co-infection: implications for pathogenesis and therapy," Pathogens, vol. 12, no. 9, 1120, 2023 |
| [6] | M. K. Sharma, Q. Wonitowy, and H. Soualhine, "Conventional and modern approaches for clinical and laboratory diagnosis of tuberculosis," in Biomedical Translational Research: From Disease Diagnosis to Treatment, Singapore: Springer Nature Singapore, pp. 209–236, 2022. |
| [7] | R. Gopalaswamy, G. Saminathan, V. Manoharan, and S. K. Shanmugam, "Challenges in the diagnosis of tuberculosis and non-tuberculosis mycobacteria," in Diagnosis and Treatment of Mycobacterial Infections, IntechOpen, 2025. |
| [8] | R. Rodrigues da Costa, M. R. Silva, C. J. Augusto, and I. C. Gonçalves Leite, "Fast, simple and cheap: method modified from conventional cultivation for tuberculosis diagnosis allows seeding on Löwenstein–Jensen of any swab-embedded pulmonary samples decontaminated with sodium hydroxide," Transactions of The Royal Society of Tropical Medicine and Hygiene, vol. 116, no. 6, pp. 523–530, 2022. |
| [9] | World Health Organization, WHO consolidated guidelines on tuberculosis. Module 3: diagnosis – rapid diagnostics for tuberculosis detection, World Health Organization, 2024. |
| [10] | Y. P. Wong, S. Othman, Y. L. Lau, S. Radu, and H. Y. Chee, "Loop-mediated isothermal amplification (LAMP): a versatile technique for detection of micro-organisms," Journal of Applied Microbiology, vol. 124, no. 3, pp. 626–643, 2018, |
| [11] | S. Reddy, S. Ntoyanto, Y. Sakadavan, T. Reddy, S. Mahomed, M. Dlamini, … and P. Kiepiela, "Detecting Mycobacterium tuberculosis using the loop-mediated isothermal amplification test in South Africa," The International Journal of Tuberculosis and Lung Disease, vol. 21, no. 10, pp. 1154–1160, 2017. |
| [12] | R. Yadav, N. Sharma, R. Khaneja, P. Agarwal, A. Kanga, D. Behera, and S. Sethi, "Evaluation of the TB-LAMP assay for the rapid diagnosis of pulmonary tuberculosis in Northern India," The International Journal of Tuberculosis and Lung Disease, vol. 21, no. 10, pp. 1150–1153, 2017. |
| [13] | M. H. Wahid, A. Sjahrurachman, A. H. Sitorus, and E. Burhan, "The role of TB-LAMP method in detecting Mycobacterium tuberculosis from sputum of patients suspected of having pulmonary tuberculosis," Acta Medica Indonesiana, vol. 52, no. 4, pp. 352–359, 2020. |
| [14] | M. Zaber, F. Hoque, I. M. Paean, and S. Tarafder, "Evaluation of multiplex loop-mediated isothermal amplification assay for the detection of Mycobacterium tuberculosis complex from clinically suspected cases of pulmonary tuberculosis," Heliyon, vol. 10, 21, 2024. |
| [15] | J. Jain, P. Jadhao, S. Banait, and P. Salunkhe, "Diagnostic accuracy of GeneXpert MTB/RIF assay for detection of tubercular pleural effusion," PLoS One, vol. 16, no. 6, e0251618, 2021. |
| [16] | E. N. Edem, A. N. Umo, O. J. Akinjogunla, A. A. Elahmar, and D. Arome, "Detection rate of pulmonary tuberculosis by direct and concentrated microscopy techniques with Lowenstein–Jensen culture as standard: South-South Nigeria scenario," Open J Bac, vol. 6, no. 1, pp. 001–005, 2022. |
| [17] | A. W. Kaso and A. Hailu, "Costs and cost-effectiveness of GeneXpert compared to smear microscopy for the diagnosis of pulmonary tuberculosis using real-world data from Arsi zone, Ethiopia," PLoS One, vol. 16, no. 10, e0259056, 2021. |
| [18] | R. Yadav, P. Daroch, P. Gupta, P. Vaidya, J. L. Mathew, M. Singh, and S. Sethi, "Evaluation of TB-LAMP assay for detection of Mycobacterium tuberculosis in children," Infectious Diseases (London, England), vol. 53, no. 12, pp. 942–946, 2021. |
| [19] | B. Gelaw, Y. Shiferaw, M. Alemayehu, and A. A. Bashaw, "Comparison of loop-mediated isothermal amplification assay and smear microscopy with culture for the diagnostic accuracy of tuberculosis," BMC Infectious Diseases, vol. 17, no. 1, 79, 2017. |
| [20] | D. Arora and B. Dhanashree, "Utility of smear microscopy and GeneXpert for the detection of Mycobacterium tuberculosis in clinical samples," Germs, vol. 10, no. 2, pp. 81–87, 2020. |
| [21] | R. Rimal, D. Shrestha, S. Pyakurel, R. Poudel, P. Shrestha, K. R. Rai, G. R. Ghimire, G. Rai, and S. K. Rai, "Diagnostic performance of GeneXpert MTB/RIF in detecting MTB in smear-negative presumptive TB patients," BMC Infectious Diseases, vol. 22, no. 1, 321, 2022. |
| [22] | L. Weldemhret, A. Hailu, G. Gebremedhn, H. Bekuretsion, G. Alemseged, G. Gebreegziabher, … and K. Mehari, "Blinded rechecking of sputum smear microscopy performance in public health facilities in Tigray region, Northern Ethiopia: Retrospective cross-sectional study," PLoS One, vol. 15, no. 10, e0239342, 2020. |
| [23] | S. Mitarai, M. Okumura, E. Toyota, T. Yoshiyama, A. Aono, A. Sejimo, … and T. Mori, "Evaluation of a simple loop-mediated isothermal amplification test kit for the diagnosis of tuberculosis," International Journal of Tuberculosis and Lung Disease, vol. 15, no. 9, pp. 1211–1217, 2011. |
| [24] | C. C. Boehme, P. Nabeta, D. Hillemann, M. P. Nicol, S. Shenai, F. Krapp, … and M. D. Perkins, "Rapid molecular detection of tuberculosis and rifampin resistance," New England Journal of Medicine, vol. 363, no. 11, pp. 1005–1015, 2010 |
APA Style
Hussein, T. A., Ali, A. M., Rahem, H. H. (2026). Performance Evaluation of TB-LAMP in the Diagnosis of Pulmonary Tuberculosis. Medicine and Health Sciences, 2(3), 115-120. https://doi.org/10.11648/j.mhs.20260203.12
ACS Style
Hussein, T. A.; Ali, A. M.; Rahem, H. H. Performance Evaluation of TB-LAMP in the Diagnosis of Pulmonary Tuberculosis. Med. Health Sci. 2026, 2(3), 115-120. doi: 10.11648/j.mhs.20260203.12
@article{10.11648/j.mhs.20260203.12,
author = {Teeba Alaa Hussein and Ali Muhsin Ali and Hussein Hameed Rahem},
title = {Performance Evaluation of TB-LAMP in the Diagnosis of Pulmonary Tuberculosis},
journal = {Medicine and Health Sciences},
volume = {2},
number = {3},
pages = {115-120},
doi = {10.11648/j.mhs.20260203.12},
url = {https://doi.org/10.11648/j.mhs.20260203.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.mhs.20260203.12},
abstract = {Background: Tuberculosis (TB), caused by Mycobacterium tuberculosis (MTB), is one of the most common infectious diseases, especially in countries with limited healthcare resources. Early and accurate diagnosis is essential to curb its spread, and loop-mediated isothermal amplification (LAMP) is a rapid, cost-effective, and reliable molecular diagnostic method. Objective: The objective of this study was to evaluate the performance of TB-LAMP as a rapid and reliable diagnostic tool for pulmonary TB and compare it with direct smears and Gene Xpert, using culture as a reference. Materials: Between February and July 2025, a total of 397 patients (227 men and 170 women) were enrolled in the study. Samples were tested by smear microscopy, culture, Xpert MTB/RIF, and TB-LAMP. Results: Of the 397 patients, 84 (21.15%) were culture-positive. Among culture-positive patients, 81 (96.4%) were positive by Gene Xpert, 69 (82.1%) by TB-LAMP, and 49 (58.3%) by direct smear microscopy. Using culture as the reference standard, the specificity, positive predictive value (PPV), and negative predictive value (NPV) of the TB-LAMP assay were 82.1% (73.9%–90.3%), 99.0% (97.9%–100%), 95.8% (91.2%–100%), and 95.4% (93.1%–97.7%), respectively. Conclusions: The TB-LAMP assay exhibits high diagnostic accuracy for the detection of Mycobacterium tuberculosis, making it a rapid, cost-effective, and reliable alternative to conventional methods, especially in resource-poor settings.},
year = {2026}
}
TY - JOUR T1 - Performance Evaluation of TB-LAMP in the Diagnosis of Pulmonary Tuberculosis AU - Teeba Alaa Hussein AU - Ali Muhsin Ali AU - Hussein Hameed Rahem Y1 - 2026/06/02 PY - 2026 N1 - https://doi.org/10.11648/j.mhs.20260203.12 DO - 10.11648/j.mhs.20260203.12 T2 - Medicine and Health Sciences JF - Medicine and Health Sciences JO - Medicine and Health Sciences SP - 115 EP - 120 PB - Science Publishing Group SN - 3070-6300 UR - https://doi.org/10.11648/j.mhs.20260203.12 AB - Background: Tuberculosis (TB), caused by Mycobacterium tuberculosis (MTB), is one of the most common infectious diseases, especially in countries with limited healthcare resources. Early and accurate diagnosis is essential to curb its spread, and loop-mediated isothermal amplification (LAMP) is a rapid, cost-effective, and reliable molecular diagnostic method. Objective: The objective of this study was to evaluate the performance of TB-LAMP as a rapid and reliable diagnostic tool for pulmonary TB and compare it with direct smears and Gene Xpert, using culture as a reference. Materials: Between February and July 2025, a total of 397 patients (227 men and 170 women) were enrolled in the study. Samples were tested by smear microscopy, culture, Xpert MTB/RIF, and TB-LAMP. Results: Of the 397 patients, 84 (21.15%) were culture-positive. Among culture-positive patients, 81 (96.4%) were positive by Gene Xpert, 69 (82.1%) by TB-LAMP, and 49 (58.3%) by direct smear microscopy. Using culture as the reference standard, the specificity, positive predictive value (PPV), and negative predictive value (NPV) of the TB-LAMP assay were 82.1% (73.9%–90.3%), 99.0% (97.9%–100%), 95.8% (91.2%–100%), and 95.4% (93.1%–97.7%), respectively. Conclusions: The TB-LAMP assay exhibits high diagnostic accuracy for the detection of Mycobacterium tuberculosis, making it a rapid, cost-effective, and reliable alternative to conventional methods, especially in resource-poor settings. VL - 2 IS - 3 ER -
Department of Biology, Mustansiriyah University, Baghdad, Iraq
Department of Biology, Baghdad University, Baghdad, Iraq
National TB Institute, Ministry of Health, Baghdad, Iraq
Information