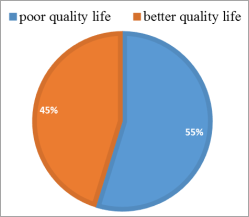
Background: Psoriasis is a skin disorder that inflames the skin and joints, increasing susceptibility to obesity, heart disease, and diabetes. It is more common in higher-altitude areas and affects 100 million people worldwide. Understanding the subtypes and treatments is crucial for the management of the condition. Method: The study used a cross-sectional design to assess quality of life and identify factors associated with poor quality of life among patients with psoriasis in the region. The study involved 219 patients. Data collection was carried out through structured interviews with patients with psoriasis attending public hospitals in Harar, eastern Ethiopia. Bivariate and multivariate logistic regression analyzes were performed to identify factors associated with poor quality of life among patients with psoriasis. Variables demonstrating a p-value > 0.20 in bivariate analyzes were included in the multivariate logistic regression model. Statistical significance was determined with a p-value < 0.05. Results: the proportion of poor quality of life was 54.8%. Factors associated with poor quality of life could not read and write (AOR = 14, 95% CI 2.08, 94.2), Duration of more than 5 years (AOR = 3.1, 95% CI 1.49, 6.41), New body site and in disease patients at both sites (AOR = 9.2, 95% CI 2.96, 28.56) and (AOR = 7.2, 95% CI 2.37, 21.95), respectively. Moderate affected body surface area (AOR= 2.98, 95% CI 1.15, 6.41)). And have a comorbidity (AOR= 2.69, 95%CI: 1.01, 7.20). Conclusions: The study revealed that 54.8% of the patients experienced severe quality of life impairment, with factors such as illiteracy, duration of the disease over five years, psoriasis at new sites of the body, moderate body surface area affected, and comorbidities significantly associated with poor quality of life. The study shed light on the challenges faced by patients with psoriasis in Harar, highlighting the need for comprehensive care strategies to improve their quality of life and well-being.
| Published in | Reports (Volume 4, Issue 3) |
| DOI | 10.11648/j.reports.20240403.11 |
| Page(s) | 27-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Quality of Life, Psoriasis, Harar, Ethiopia
Variables | Frequency | Percent |
|---|---|---|
Sex | ||
Female | 100 | 45.66 |
Male | 119 | 54.34 |
Age | ||
16-35 | 80 | 36.53 |
36-65 | 126 | 57.53 |
Above 65 | 13 | 5.94 |
Monthly Income | ||
Low income (<2000) | 83 | 38.81 |
Average income (2001-3000) | 47 | 21.46 |
Above average income (3001-6000) | 47 | 21.46 |
High income (>6000) | 40 | 18.26 |
Marital status | ||
Single | 70 | 31.96 |
Married | 126 | 57.53 |
Widowed | 15 | 6.85 |
Divorced | 8 | 3.65 |
Educational status | ||
Can't read and write | 22 | 10.05 |
Primary | 38 | 17.35 |
Secondary | 68 | 31.05 |
Technical/Vocational | 33 | 15.07 |
College or University | 58 | 26.48 |
Occupational status | ||
House wife | 41 | 18.72 |
Government employee | 86 | 39.72 |
Non-government employee | 92 | 42.01 |
Religion | ||
Orthodox | 143 | 65.30 |
Muslim | 46 | 21 |
Protestant | 30 | 13.70 |
Alcohol use | ||
No | 185 | 84.47 |
Yes | 34 | 15.53 |
Smoking cigarette | ||
No | 205 | 93.61 |
Yes | 14 | 6.39 |
Khat chewing | ||
No | 204 | 93.15 |
Yes | 15 | 6.85 |
Variables | Frequency | Percent |
|---|---|---|
Age at initial diagnosis | ||
Age at onset <40 | 147 | 67.12 |
Age at onset >=40 | 72 | 38.88 |
Duration of the illness | ||
Duration <5 years | 119 | 54.34 |
Duration>=5 years | 100 | 45.66 |
New body site | ||
Unexposed | 40 | 18.26 |
Exposed | 70 | 31.96 |
Both site | 109 | 49.77 |
Body surface area affected | ||
Mild | 90 | 41.10 |
Moderate | 69 | 31.51 |
Severe | 60 | 27.40 |
Treatment types | ||
Tropical | 171 | 78.08 |
Systematic | 48 | 21.92 |
Comorbid illness | ||
No | 171 | 78.08 |
Yes | 48 | 21.92 |
Variables | Psoriasis QOL | COR (95%CI) | AOR (95%CI) | |
|---|---|---|---|---|
Poor | Better | |||
Sex | ||||
Female | 51 | 49 | 1 | 1 |
Male | 69 | 50 | 1.33 (0.78, 2.26) | 1.71 (0.74, 3.99) |
Monthly Income | ||||
Low income (<2000) | 47 | 38 | 1 | 1 |
Average income (2001-3000) | 25 | 22 | 0.92 (0.45, 1.88) | 0.75 (0.28, 2.01) |
Above average income (3001-6000) | 27 | 20 | 1.01 (0.53, 2.24) | 0.77 (0.28, 2.16) |
High income (>6000) | 21 | 19 | 0.89 (0.42, 1.90) | 0.67 (0.21, 2.16) |
Educational status | ||||
Can't read and write | 9 | 13 | 2.78 (0.94, 8.20) | 14.0 (2.08, 94.2)* |
Primary | 25 | 13 | 1.63 (0.61, 4.30) | 4.66 (0.85, 25.73) |
Secondary | 36 | 32 | 1.73 (0.58, 5.16) | 3.93 (0.63, 24.33) |
Technical/Vocational | 18 | 15 | 1.78 (0.66, 4.81) | 5.54 (0.88, 34.66) |
College or University | 32 | 26 | 1 | 1 |
Alcohol use | ||||
No | 102 | 83 | 1 | 1 |
Yes | 18 | 16 | 0.92 (0.44, 1.91) | 1.15 (0.39, 3.40) |
Smoking cigarette | ||||
No | 112 | 93 | 1 | 1 |
Yes | 8 | 6 | 1.11 (0.37, 3.30) | 1.97 (0.12, 7.75) |
Khat chewing | ||||
No | 111 | 93 | 1 | 1 |
Yes | 9 | 6 | 1.26 (0.43, 3.66) | 1.18 (0.15, 9.07) |
Duration of the illness | ||||
Duration <5 years | 52 | 67 | 1 | 1 |
Duration>=5 years | 68 | 32 | 2.74 (1.57, 4.77)* | 3.1 (1.49, 6.41)* |
New body site | ||||
Unexposed | 9 | 31 | 1 | 1 |
Exposed | 39 | 31 | 4.33 (1.79, 10.44)* | 9.2 (2.96, 28.56)* |
Both site | 72 | 37 | 6.7 (2.89, 15.55)* | 7.2 (2.37, 21.95)* |
Body surface area affected | ||||
Mild | 36 | 54 | 1 | 1 |
Moderate | 45 | 24 | 2.81 (1.47, 5.39)* | 2.98 (1.15, 6.41)* |
Severe | 39 | 21 | 2.79 (1.41, 5.49)* | 1.89 (0.56, 6.21) |
Treatment types | ||||
Tropical | 90 | 81 | 1 | 1 |
Systematic | 30 | 18 | 1.5 (0.78, 2.89) | 0.69 (0.24, 1.94) |
Presence of Comorbid | ||||
No | 88 | 83 | 1 | 1 |
Yes | 32 | 16 | 1.89 (0.96, 3.69) | 2.69 (1.01, 7.20)* |
DLOI | Dermatology Quality of Life Index |
HRQOL | Health-Related Quality of Life |
QOL | Quality of Life |
WHO | World Health Organization |
| [1] | Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ (Clinical research ed). 2020; 369: m1590. |
| [2] | Belinchón I, Rivera R, Blanch C, Comellas M, Lizán L. Adherence, satisfaction and preferences for treatment in patients with psoriasis in the European Union: a systematic review of the literature. Patient preference and adherence. 2016; 10: 2357-67. |
| [3] | Tejada Cdos S, Mendoza-Sassi RA, Almeida HL, Jr., Figueiredo PN, Tejada VF. Impact on the quality of life of dermatological patients in southern Brazil. Anais brasileiros de dermatologia. 2011; 86(6): 1113-21. |
| [4] | Goyal S, Pisharody RR, Nath S. Psychiatric morbidity in psoriasis: A case-control study. Journal of Marine Medical Society. 2017; 19: 18. |
| [5] | Meneguin S, de Godoy NA, Pollo CF, Miot HA, de Oliveira C. Quality of life of patients living with psoriasis: a qualitative study. BMC dermatology. 2020; 20(1): 22. |
| [6] | Lebwohl M. Psoriasis. Annals of internal medicine. 2018; 168(7): Itc49-itc64. |
| [7] | García-Sánchez L, Montiel-Jarquín Á J, Vázquez-Cruz E, May-Salazar A, Gutiérrez-Gabriel I, Loría-Castellanoso J. [Quality of life in patients with psoriasis]. Gaceta medica de Mexico. 2017; 153(2): 185-9. |
| [8] | Seefu Megarsa Kumsa TAT, Minyahil Alebachew Woldu. Management practice, quality of life and associated factors in psoriasis patients attending a dermatological center in Ethiopia. 2020. |
| [9] | Schadler ED, Ortel B, Mehlis SL. Biologics for the primary care physician: Review and treatment of psoriasis. Disease-a-month: DM. 2019; 65(3): 51-90. |
| [10] | Mehrmal S, Uppal P, Nedley N, Giesey RL, Delost GR. The global, regional, and national burden of psoriasis in 195 countries and territories, 1990 to 2017: A systematic analysis from the Global Burden of Disease Study 2017. Journal of the American Academy of Dermatology. 2021; 84(1): 46-52. |
| [11] | Aynalem S. Psoriasis at Ayder Referral Hospital among Patients Attending Dermatology Clinic, Mekelle, North Ethiopia. Science Journal of Clinical Medicine. 2014; 3: 106. |
| [12] | Abdulghani M, Al Sheik A, Alkhawajah M, Ammoury A, Behrens F, Benchikhi H, et al. Management of psoriasis in Africa and the Middle East: a review of current opinion, practice and opportunities for improvement. The Journal of international medical research. 2011; 39(5): 1573-88. |
| [13] | Lane H, Walker M. The Impact of Temperature, Humidity, and Sunshine on Internet Search Volumes Related to Psoriasis. 2023; 6: e49901. |
| [14] | The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization. Social science & medicine (1982). 1995; 41(10): 1403-9. |
| [15] | Ferrans CE, Zerwic JJ, Wilbur JE, Larson JL. Conceptual model of health-related quality of life. Journal of nursing scholarship: an official publication of Sigma Theta Tau International Honor Society of Nursing. 2005; 37(4): 336-42. |
| [16] | Kumsa SM, Tadesse TA. Management practice, quality of life and associated factors in psoriasis patients attending a dermatological center in Ethiopia. 2021; 16(11): e0260243. |
| [17] | Belachew EA, Sendekie AK. Health-related quality of life and its determinants in patients with different dermatological disorders at the University of Gondar Comprehensive Specialized Hospital. BMC Research Notes. 2023; 16(1): 191. |
| [18] | Kamio Y, Inada N, Koyama T. A nationwide survey on quality of life and associated factors of adults with high-functioning autism spectrum disorders. Autism. 2013; 17(1): 15-26. |
| [19] | Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clinical and experimental dermatology. 1994; 19(3): 210-6. |
| [20] | Mohd Shahriman Ahmad Fuat, Zainab Mat Yudin, Juliawati Muhammad andFaridah Mohd Zin. Quality of Life and Its Associated Factors among Patients with Psoriasis in a Semi-Urban Northeast Malaysia. 2022. |
| [21] | Yang H-J, Yang K-C. Impact of psoriasis on quality of life in Taiwan. Dermatologica Sinica. 2015; 33. |
| [22] | Tang MM, Chang CC, Chan LC, Heng A. Quality of life and cost of illness in patients with psoriasis in Malaysia: a multicenter study. International journal of dermatology. 2013; 52(3): 314-22. |
| [23] | Chen C-Y. Quality of life and its associated factors for psoriasis patients in China: a cross-sectional study from hospital-based data. 2016. |
| [24] | Youn SW, Lee JH, Yu DY, Kim Y, Kim BS, Seo SJ, et al. The relationship between clinical characteristics including presence of exposed lesions and health-related quality of life (HRQoL) in patients with psoriasis: analysis from the nationwide epidemiologic study for psoriasis in Korea (EPI-PSODE study). Journal of the European Academy of Dermatology and Venereology: JEADV. 2018; 32(9): 1499-506. |
| [25] | Ahmad Fuat MS, Mat Yudin Z. Quality of Life and Its Associated Factors among Patients with Psoriasis in a Semi-Urban Northeast Malaysia. 2022; 19(18). |
| [26] | Gelfand JM, Feldman SR, Stern RS, Thomas J, Rolstad T, Margolis DJ. Determinants of quality of life in patients with psoriasis: A study from the US population. Journal of the American Academy of Dermatology. 2004; 51(5): 704-8. |
| [27] | Armstrong AW, Schupp C, Wu J, Bebo B. Quality of life and work productivity impairment among psoriasis patients: findings from the National Psoriasis Foundation survey data 2003-2011. PLoS One. 2012; 7(12): e52935. |
| [28] | Jankovic S, Raznatovic M, Marinkovic J, Jankovic J, Kocev N, Tomic-Spiric V, et al. Health-Related Quality of Life in Patients with Psoriasis. Journal of Cutaneous Medicine and Surgery. 2011; 15(1): 29-36. |
APA Style
Bayisa, F. S., Nimani, T. D., Darcho, S. D. (2024). Quality of Life and Its Associated Factors Among Patients with Psoriasis Attending the Dermatology Department at Public Hospitals in Harar Town, Eastern Ethiopia. Reports, 4(3), 27-36. https://doi.org/10.11648/j.reports.20240403.11
ACS Style
Bayisa, F. S.; Nimani, T. D.; Darcho, S. D. Quality of Life and Its Associated Factors Among Patients with Psoriasis Attending the Dermatology Department at Public Hospitals in Harar Town, Eastern Ethiopia. Reports. 2024, 4(3), 27-36. doi: 10.11648/j.reports.20240403.11
AMA Style
Bayisa FS, Nimani TD, Darcho SD. Quality of Life and Its Associated Factors Among Patients with Psoriasis Attending the Dermatology Department at Public Hospitals in Harar Town, Eastern Ethiopia. Reports. 2024;4(3):27-36. doi: 10.11648/j.reports.20240403.11
@article{10.11648/j.reports.20240403.11,
author = {Feyisa Shasho Bayisa and Teshome Demis Nimani and Samuel Demissie Darcho},
title = {Quality of Life and Its Associated Factors Among Patients with Psoriasis Attending the Dermatology Department at Public Hospitals in Harar Town, Eastern Ethiopia
},
journal = {Reports},
volume = {4},
number = {3},
pages = {27-36},
doi = {10.11648/j.reports.20240403.11},
url = {https://doi.org/10.11648/j.reports.20240403.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.reports.20240403.11},
abstract = {Background: Psoriasis is a skin disorder that inflames the skin and joints, increasing susceptibility to obesity, heart disease, and diabetes. It is more common in higher-altitude areas and affects 100 million people worldwide. Understanding the subtypes and treatments is crucial for the management of the condition. Method: The study used a cross-sectional design to assess quality of life and identify factors associated with poor quality of life among patients with psoriasis in the region. The study involved 219 patients. Data collection was carried out through structured interviews with patients with psoriasis attending public hospitals in Harar, eastern Ethiopia. Bivariate and multivariate logistic regression analyzes were performed to identify factors associated with poor quality of life among patients with psoriasis. Variables demonstrating a p-value > 0.20 in bivariate analyzes were included in the multivariate logistic regression model. Statistical significance was determined with a p-value Results: the proportion of poor quality of life was 54.8%. Factors associated with poor quality of life could not read and write (AOR = 14, 95% CI 2.08, 94.2), Duration of more than 5 years (AOR = 3.1, 95% CI 1.49, 6.41), New body site and in disease patients at both sites (AOR = 9.2, 95% CI 2.96, 28.56) and (AOR = 7.2, 95% CI 2.37, 21.95), respectively. Moderate affected body surface area (AOR= 2.98, 95% CI 1.15, 6.41)). And have a comorbidity (AOR= 2.69, 95%CI: 1.01, 7.20). Conclusions: The study revealed that 54.8% of the patients experienced severe quality of life impairment, with factors such as illiteracy, duration of the disease over five years, psoriasis at new sites of the body, moderate body surface area affected, and comorbidities significantly associated with poor quality of life. The study shed light on the challenges faced by patients with psoriasis in Harar, highlighting the need for comprehensive care strategies to improve their quality of life and well-being.
},
year = {2024}
}
TY - JOUR T1 - Quality of Life and Its Associated Factors Among Patients with Psoriasis Attending the Dermatology Department at Public Hospitals in Harar Town, Eastern Ethiopia AU - Feyisa Shasho Bayisa AU - Teshome Demis Nimani AU - Samuel Demissie Darcho Y1 - 2024/08/15 PY - 2024 N1 - https://doi.org/10.11648/j.reports.20240403.11 DO - 10.11648/j.reports.20240403.11 T2 - Reports JF - Reports JO - Reports SP - 27 EP - 36 PB - Science Publishing Group SN - 2994-7146 UR - https://doi.org/10.11648/j.reports.20240403.11 AB - Background: Psoriasis is a skin disorder that inflames the skin and joints, increasing susceptibility to obesity, heart disease, and diabetes. It is more common in higher-altitude areas and affects 100 million people worldwide. Understanding the subtypes and treatments is crucial for the management of the condition. Method: The study used a cross-sectional design to assess quality of life and identify factors associated with poor quality of life among patients with psoriasis in the region. The study involved 219 patients. Data collection was carried out through structured interviews with patients with psoriasis attending public hospitals in Harar, eastern Ethiopia. Bivariate and multivariate logistic regression analyzes were performed to identify factors associated with poor quality of life among patients with psoriasis. Variables demonstrating a p-value > 0.20 in bivariate analyzes were included in the multivariate logistic regression model. Statistical significance was determined with a p-value Results: the proportion of poor quality of life was 54.8%. Factors associated with poor quality of life could not read and write (AOR = 14, 95% CI 2.08, 94.2), Duration of more than 5 years (AOR = 3.1, 95% CI 1.49, 6.41), New body site and in disease patients at both sites (AOR = 9.2, 95% CI 2.96, 28.56) and (AOR = 7.2, 95% CI 2.37, 21.95), respectively. Moderate affected body surface area (AOR= 2.98, 95% CI 1.15, 6.41)). And have a comorbidity (AOR= 2.69, 95%CI: 1.01, 7.20). Conclusions: The study revealed that 54.8% of the patients experienced severe quality of life impairment, with factors such as illiteracy, duration of the disease over five years, psoriasis at new sites of the body, moderate body surface area affected, and comorbidities significantly associated with poor quality of life. The study shed light on the challenges faced by patients with psoriasis in Harar, highlighting the need for comprehensive care strategies to improve their quality of life and well-being. VL - 4 IS - 3 ER -
Department of Epidemiology and Biostatistics, School of Public Health College of Medicine and Health Science, Haramaya University, Harar, Ethiopia
Department of Epidemiology and Biostatistics, School of Public Health College of Medicine and Health Science, Haramaya University, Harar, Ethiopia
Department of Health Service and Policy Management, School of Public Health, College of Medicine and Health Science, Haramaya University, Harar, Ethiopia
Information