Background: Immunization is known to be a cost-effective intervention; addressing more than (20) diseases. The Expanded Program on Immunization (EPI) was established to ensure target population, especially children, benefit from life-saving immunization services. Securing resources, establishing systems, and demand generation are crucial for successful immunization programs. The ongoing conflict in Sudan, resulting in displacement of over 10 million people, had severely affected country’s immunization services. This study explores the impact of the conflict on Sudan’s EPI and examines the strategies employed to mitigate these challenges. Methods: A qualitative synthesis and desk review were conducted to explore the best practices, innovations, challenges, and lessons learned from June 2023- to December 2024. Five of the authors collaborated to identify sources and extracted data from the EPI reports and records. Two other authors verified the outcomes and complemented it using meeting memos. Compiled findings were shared with other authors for review and feedback. Data was manually organized and analyzed using a thematic analysis. Key themes reflected the situation of EPI program before the conflict, the impact of war on the program, and the response of EPI program. Thematic areas encompassed human resources, cold chain, routine immunization, supplementary immunization activities, surveillance and outbreak investigation. Results: By the end of 2024, the EPI in Sudan started to reverse the decline in immunization services’ coverage and accessibility resulting from war. Modification of service delivery strategies; contemplating the security status district by district was key success factor. Furthermore, program’s resilience was supported by a dedicated, committed, and responsive EPI teams at national and sub-national levels, operating in collaboration and coordination with partners, motivated by a unified vision encapsulated in the slogan “Despite what is happening, vaccination must continue”. Conclusions: To sustain the immunization services in Sudan, the EPI prioritized the cohesion and solidarity of the team, adopting a collaborative approach. This durable essence of unity was especially evident is expanding partnership in security compromised states.
| Published in | Science Journal of Public Health (Volume 13, Issue 5) |
| DOI | 10.11648/j.sjph.20251305.14 |
| Page(s) | 283-295 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Immunization, Sudan, Conflict, Acheivement, Lesson Leant
States | 2022 | 2023 | 2024 | |||
|---|---|---|---|---|---|---|
Penta 1 | Penta 3 | Penta 1 | Penta 1 | Penta 1 | Penta 3 | |
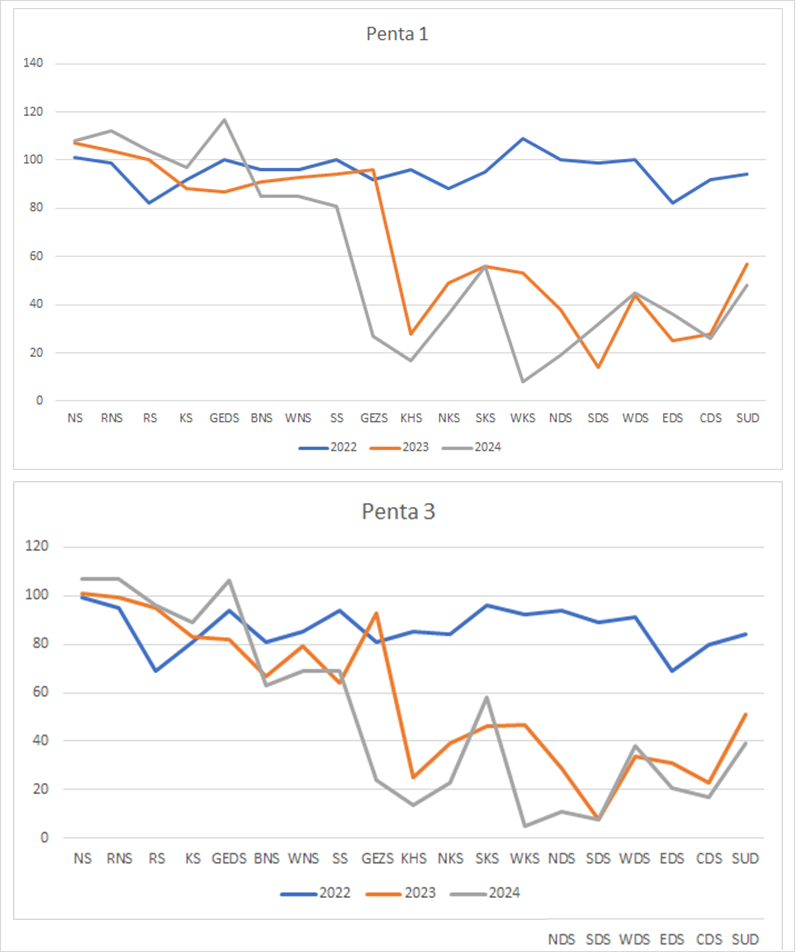
Northern | 101 | 99 | 107 | 101 | 108 | 107 |
River Nile | 99 | 95 | 104 | 99 | 112 | 107 |
Red Sea | 82 | 69 | 100 | 95 | 104 | 96 |
Kassala | 92 | 81 | 88 | 83 | 97 | 89 |
Gedarif | 100 | 94 | 87 | 82 | 117 | 106 |
Blue Nile | 96 | 81 | 91 | 67 | 85 | 63 |
White Nile | 96 | 85 | 93 | 79 | 85 | 69 |
Sennar | 100 | 94 | 94 | 64 | 81 | 69 |
Gezira | 92 | 81 | 96 | 93 | 27 | 24 |
Khartoum | 96 | 85 | 28 | 25 | 17 | 14 |
N. Kordofan | 88 | 84 | 49 | 39 | 36 | 23 |
S. Kordofan | 95 | 96 | 56 | 46 | 56 | 58 |
W. Kordofan | 109 | 92 | 53 | 47 | 8 | 5 |
N. Darfur | 100 | 94 | 38 | 29 | 19 | 11 |
S. Darfur | 99 | 89 | 14 | 8 | 32 | 8 |
W. Darfur | 100 | 91 | 44 | 34 | 45 | 38 |
E. Darfur | 82 | 69 | 25 | 31 | 36 | 21 |
C. Darfur | 92 | 80 | 28 | 23 | 26 | 17 |
Sudan | 94 | 84 | 57 | 51 | 48 | 39 |
Class and access level | Health system readiness | Target | Key challenges | Adapted strategies |
|---|---|---|---|---|
States | ||||
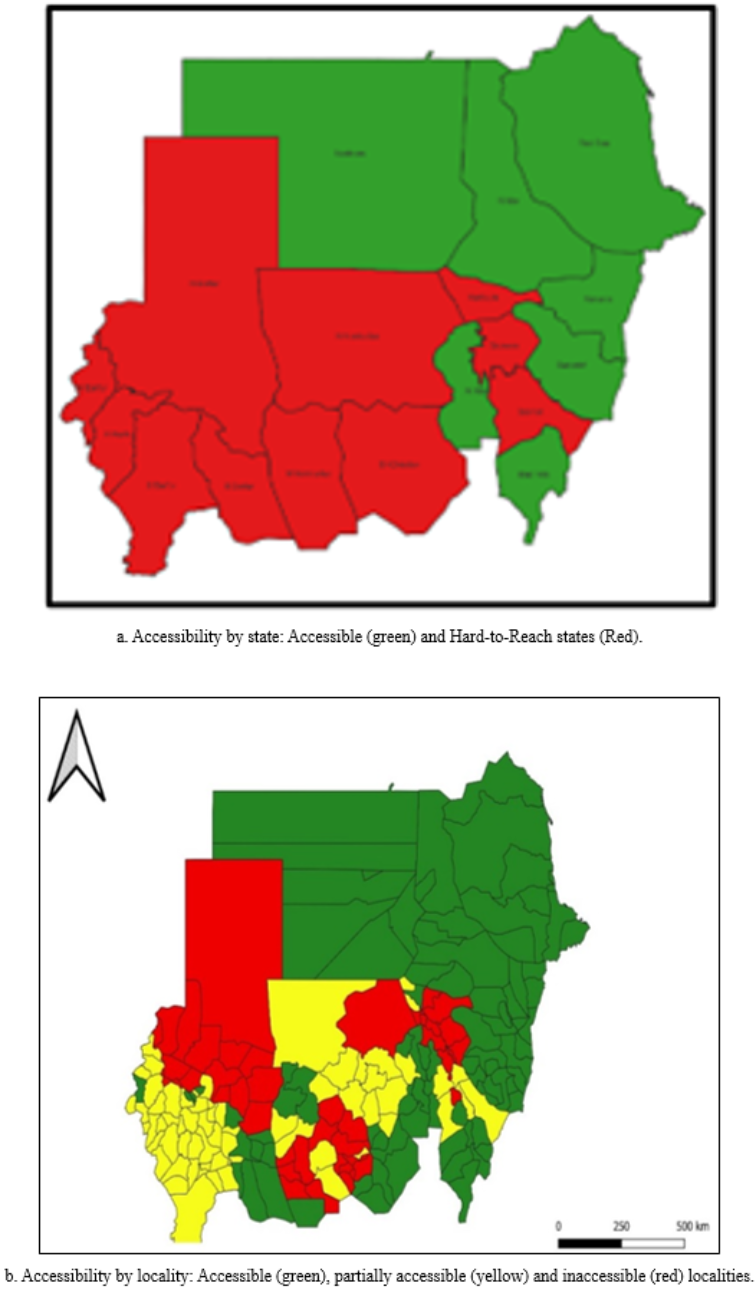
Group A (Accessible states) | High | 491,559 | IDPs, rainy season, change of the target population | Regular outreach Fixed site services maintained PIRI |
Group B (Hard-to-reach states) | Moderate/ low | 1,364,814 | Intermittent access, security threats, severe conflict, supply chain disruptions, change of the target population | Mobile health units Community-led campaigns Temporary vaccination posts Use of local mediators Hit and Run PIRI |
Localities | ||||
Accessible | High | 842,089 | IDPs, rainy season, change of the target population | Regular outreach Fixed site services maintained |
Partially accessible | Moderate | 660,372 | Intermittent access, security threats, IDPs, rainy season, change of the target population | Mobile health units Community-led campaigns |
Inaccessible | Low | 327,854 | Severe conflict, supply chain disruptions, change of the target population | Temporary vaccination posts Use of local mediators Hit and run |
State | April 2023- June 2023 | July 2023- December 2024 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
## of sites | ## of functioning sites | % of functioning sites | ## of reporting sites | % Reporting out of functioning | ## of sites | ## of functioning sites | % of functioning sites | ## of reporting sites | % Reporting out of functioning | |
Northern | 65 | 0 | 0 | 0 | 0 | 65 | 65 | 100 | 65 | 100 |
River Nile | 84 | 0 | 0 | 0 | 0 | 84 | 84 | 100 | 84 | 100 |
Red sea | 53 | 0 | 0 | 0 | 0 | 53 | 53 | 100 | 53 | 100 |
Kassala | 43 | 0 | 0 | 0 | 0 | 43 | 43 | 100 | 43 | 100 |
Gedarif | 56 | 0 | 0 | 0 | 0 | 56 | 56 | 100 | 56 | 100 |
Blue Nile | 33 | 0 | 0 | 0 | 0 | 33 | 28 | 85 | 28 | 100 |
White Nile | 53 | 0 | 0 | 0 | 0 | 53 | 53 | 100 | 49 | 92 |
Sennar | 33 | 0 | 0 | 0 | 0 | 33 | 33 | 100 | 33 | 100 |
Gezira | 102 | 0 | 0 | 0 | 0 | 102 | 80 | 78 | 80 | 100 |
Khartoum | 108 | 0 | 0 | 0 | 0 | 108 | 22 | 20 | 22 | 100 |
N. Kordofan | 64 | 0 | 0 | 0 | 0 | 64 | 56 | 88 | 56 | 100 |
S. Kordofan | 32 | 0 | 0 | 0 | 0 | 32 | 27 | 84 | 27 | 100 |
W. Kordofan | 42 | 0 | 0 | 0 | 0 | 42 | 22 | 52 | 22 | 100 |
N. Darfur | 47 | 0 | 0 | 0 | 0 | 47 | 7 | 15 | 7 | 100 |
S. Darfur | 52 | 0 | 0 | 0 | 0 | 52 | 52 | 100 | 52 | 100 |
W. Darfur | 55 | 0 | 0 | 0 | 0 | 55 | 43 | 78 | 43 | 100 |
E. Darfur | 30 | 0 | 0 | 0 | 0 | 30 | 30 | 100 | 30 | 100 |
C. Darfur | 59 | 0 | 0 | 0 | 0 | 59 | 50 | 51 | 30 | 60 |
Sudan | 1011 | 0 | 0 | 0.0 | 0 | 1011 | 804 | 77 | 780 | 97.0 |
AEFIs | Adverse Events Following Immunization |
AFP | Acute Flaccid Paralysis |
CBS | Community-based Surveillance |
EPI | Expanded Program on Immunization |
EMRO | WHO Eastern Mediterranean Regional Office |
FMoH | Federal Ministry of Health |
GAVI | Global Alliance for Vaccines and Immunization |
MCV | Measles Containing Vaccine |
M&E | Monitoring and Evaluation |
MR | Measles-rubella |
MSF | Médecins Sans Frontières |
NCC | The National Certification Committee |
NEC | The National Expert Committee |
NGOs | Non-governmental Organizations |
NITAG | National Immunization Technical Advisory Group |
NPHL | National Public Health Laboratory |
OCV | Oral Cholera Vaccine |
PHC | Primary Health Care |
RI | Routine Immunization |
SBC | Social and Behavioral Change |
SCI | Save the Children International |
SIAs | Supplementary Immunization Activities |
VPDs | Vaccine Preventable Diseases |
WHO | World Health Organization |
| [1] | Ozawa S, Mirelman A, Stack ML, Walker DG, Levine OS. Cost-effectiveness and economic benefits of vaccines in low- and middle-income countries: A systematic review. Vaccine. 2012 Dec 17; 31(1): 96-108. |
| [2] |
WHO. Immunization Agenda 2030: A Global Strategy to Leave No One Behind [Internet]. 2020 [cited 2025 May 21]. Available from:
https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030 |
| [3] | World Health Organization (WHO). A guide for conducting an Expanded Program on Immunization (EPI) Review [Internet]. Geneva; 2017 [cited 2025 May 21]. Available from: |
| [4] | Shah MP, Morgan CJ, Beeson JG, Peach E, Davis J, McPake B, et al. Systematic Review Integrated Approaches for the Delivery of Maternal and Child Health Services with Childhood Immunization Programs in Low-and Middle-Income Countries: Systematic Review Update 2011-2020. 2024; 12: 1313. |
| [5] | Ngo NV, Pemunta NV, Muluh NE, Adedze M, Basil N, Agwale S. Armed conflict, a neglected determinant of childhood vaccination: some children are left behind. Vol. 16, Human Vaccines and Immunotherapeutics. Taylor and Francis Inc.; 2020. p. 1454-63. |
| [6] | Bouaddi O, Seedat F, Hasaan Mohammed HE, Evangelidou S, Deal A, Requena-Méndez A, et al. Vaccination coverage and access among children and adult migrants and refugees in the Middle East and North African region: a systematic review and meta-analysis. EClinicalMedicine. 2024 Dec 1; 78. |
| [7] |
United Nations Children’s Fund (UNICEF). UNICEF Immunization Roadmap 2018-2030 [Internet]. New York, NY 100017; 2018 [cited 2025 May 22]. Available from:
https://www.unicef.org/sites/default/files/2019-01/UNICEF_Immunization_Roadmap_2018.pdf |
| [8] | Wigley A, Lorin J, Hogan D, Utazi CE, Hagedorn B, Dansereau E, et al. Estimates of the number and distribution of zero-dose and under-immunized children across remote-rural, urban, and conflict-affected settings in low and middle-income countries. PLOS Global Public Health. 2022 Oct 1; 2(10 October). |
| [9] | Haq Z, Shaikh BT, Tran N, Hafeez A, Ghaffar A. System within systems: Challenges and opportunities for the expanded program on immunization in Pakistan. Health Res Policy Syst. 2019 May 17; 17(1). |
| [10] | Asrade G, Alemu K, Gebeye E, Walle M, Teklu A, Mekonnen ZA, et al. The Burden of Internal Conflict on Expanded Programs on Immunization in Northwest Ethiopia: Implementation Science Study. Vol. 35. 2021. |
| [11] | Sabahelzain MM, Almaleeh A, Abdelmagid N, Abdalla O, Nor B, Mounier-Jack S, et al. Vaccination strategies to identify and reach zero-dose and under-immunized children in crisis-affected states in Sudan: a qualitative study. Confl Health. 2024 Dec 1; 18(1). |
| [12] |
CIOMS and WHO. International ethical guidelines for health-related research involving humans [Internet]. Geneva: CIOMS; 2017 [cited 2025 May 22]. 122 p. Available from:
https://cioms.ch/wp-content/uploads/2017/01/WEB-CIOMS-EthicalGuidelines.pdf |
| [13] | Obradovic Z, Balta S, Obradovic A, Mesic S. The Impact of War on Vaccine Preventable Diseases. Materia Socio Medica. 2014; 26(6): 382. |
| [14] | Baatz RK, Ekzayez A, Najib Y, Alkhalil M, Salem M, Alshiekh MA, et al. Vaccination governance in protracted conflict settings: the case of northwest Syria. BMC Health Serv Res. 2024 Dec 1; 24(1). |
| [15] | Rzymski P, Falfushynska H, Fal A. Vaccination of Ukrainian Refugees: Need for Urgent Action. Vol. 75, Clinical Infectious Diseases. Oxford University Press; 2022. p. 1103-8. |
| [16] |
World Health Organization (WHO). Ten threats to global health in 2019. 2019 [cited 2025 May 22]; Available from:
https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 |
| [17] | Tankwanchi AS, Bowman B, Garrison M, Larson H, Wiysonge CS. Vaccine hesitancy in migrant communities: a rapid review of latest evidence. Vol. 71, Current Opinion in Immunology. Elsevier Ltd; 2021. p. 62-8. |
| [18] | Nnadi C, Etsano A, Uba B, Ohuabunwo C, Melton M, Wa Nganda G, et al. Approaches to Vaccination among Populations in Areas of Conflict. Journal of Infectious Diseases. 2017 Jul 1; 216: S368-72. |
| [19] | Hassan IN, Abuassa N, Ibrahim M. The Sudan conflict: A catalyst for the spread of infectious diseases in displaced populations. Vol. 151, International Journal of Infectious Diseases. Elsevier B. V.; 2025. |
| [20] | Al-Dar AA, Al-Qassimi M, Ezzadeen FH, Qassime M, Al murtadha AM, Ghaleb Y. Diphtheria resurgence in Sada’a-Yemen, 2017-2020. BMC Infect Dis. 2022 Dec 1; 22(1). |
| [21] | Hussain SF, Boyle P, Patel P, Sullivan R. Eradicating polio in Pakistan: An analysis of the challenges and solutions to this security and health issue. Vol. 12, Globalization and Health. BioMed Central Ltd.; 2016. |
| [22] | Wiesen E, Dankoli R, Musa M, Higgins J, Forbi J, Idris J, et al. Conducting public health surveillance in areas of armed conflict and restricted population access: a qualitative case study of polio surveillance in conflict-affected areas of Borno State, Nigeria. Confl Health. 2022 Dec 1; 16(1). |
APA Style
Aladani, I., Adam, A., Babakir, A., Alnair, N. M. A., Hammad, N., et al. (2025). Sustaining Immunization Under the Roar of Cannons: Lessons Learned from Sudan, June 2023 to December 2024. Science Journal of Public Health, 13(5), 283-295. https://doi.org/10.11648/j.sjph.20251305.14
ACS Style
Aladani, I.; Adam, A.; Babakir, A.; Alnair, N. M. A.; Hammad, N., et al. Sustaining Immunization Under the Roar of Cannons: Lessons Learned from Sudan, June 2023 to December 2024. Sci. J. Public Health 2025, 13(5), 283-295. doi: 10.11648/j.sjph.20251305.14
@article{10.11648/j.sjph.20251305.14,
author = {Ismail Aladani and Abdulaziz Adam and Abdelrahim Babakir and Nada Mohamed Ali Alnair and Nadir Hammad and Sahar Abd Elmoniem Alrayah and Nassir Gobara and Ekhlas Elgeli and Mohammed Elhussien and Ali Babiker Habour and Elfatih Mohamed Malik},
title = {Sustaining Immunization Under the Roar of Cannons: Lessons Learned from Sudan, June 2023 to December 2024
},
journal = {Science Journal of Public Health},
volume = {13},
number = {5},
pages = {283-295},
doi = {10.11648/j.sjph.20251305.14},
url = {https://doi.org/10.11648/j.sjph.20251305.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251305.14},
abstract = {Background: Immunization is known to be a cost-effective intervention; addressing more than (20) diseases. The Expanded Program on Immunization (EPI) was established to ensure target population, especially children, benefit from life-saving immunization services. Securing resources, establishing systems, and demand generation are crucial for successful immunization programs. The ongoing conflict in Sudan, resulting in displacement of over 10 million people, had severely affected country’s immunization services. This study explores the impact of the conflict on Sudan’s EPI and examines the strategies employed to mitigate these challenges. Methods: A qualitative synthesis and desk review were conducted to explore the best practices, innovations, challenges, and lessons learned from June 2023- to December 2024. Five of the authors collaborated to identify sources and extracted data from the EPI reports and records. Two other authors verified the outcomes and complemented it using meeting memos. Compiled findings were shared with other authors for review and feedback. Data was manually organized and analyzed using a thematic analysis. Key themes reflected the situation of EPI program before the conflict, the impact of war on the program, and the response of EPI program. Thematic areas encompassed human resources, cold chain, routine immunization, supplementary immunization activities, surveillance and outbreak investigation. Results: By the end of 2024, the EPI in Sudan started to reverse the decline in immunization services’ coverage and accessibility resulting from war. Modification of service delivery strategies; contemplating the security status district by district was key success factor. Furthermore, program’s resilience was supported by a dedicated, committed, and responsive EPI teams at national and sub-national levels, operating in collaboration and coordination with partners, motivated by a unified vision encapsulated in the slogan “Despite what is happening, vaccination must continue”. Conclusions: To sustain the immunization services in Sudan, the EPI prioritized the cohesion and solidarity of the team, adopting a collaborative approach. This durable essence of unity was especially evident is expanding partnership in security compromised states.
},
year = {2025}
}
TY - JOUR T1 - Sustaining Immunization Under the Roar of Cannons: Lessons Learned from Sudan, June 2023 to December 2024 AU - Ismail Aladani AU - Abdulaziz Adam AU - Abdelrahim Babakir AU - Nada Mohamed Ali Alnair AU - Nadir Hammad AU - Sahar Abd Elmoniem Alrayah AU - Nassir Gobara AU - Ekhlas Elgeli AU - Mohammed Elhussien AU - Ali Babiker Habour AU - Elfatih Mohamed Malik Y1 - 2025/10/10 PY - 2025 N1 - https://doi.org/10.11648/j.sjph.20251305.14 DO - 10.11648/j.sjph.20251305.14 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 283 EP - 295 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20251305.14 AB - Background: Immunization is known to be a cost-effective intervention; addressing more than (20) diseases. The Expanded Program on Immunization (EPI) was established to ensure target population, especially children, benefit from life-saving immunization services. Securing resources, establishing systems, and demand generation are crucial for successful immunization programs. The ongoing conflict in Sudan, resulting in displacement of over 10 million people, had severely affected country’s immunization services. This study explores the impact of the conflict on Sudan’s EPI and examines the strategies employed to mitigate these challenges. Methods: A qualitative synthesis and desk review were conducted to explore the best practices, innovations, challenges, and lessons learned from June 2023- to December 2024. Five of the authors collaborated to identify sources and extracted data from the EPI reports and records. Two other authors verified the outcomes and complemented it using meeting memos. Compiled findings were shared with other authors for review and feedback. Data was manually organized and analyzed using a thematic analysis. Key themes reflected the situation of EPI program before the conflict, the impact of war on the program, and the response of EPI program. Thematic areas encompassed human resources, cold chain, routine immunization, supplementary immunization activities, surveillance and outbreak investigation. Results: By the end of 2024, the EPI in Sudan started to reverse the decline in immunization services’ coverage and accessibility resulting from war. Modification of service delivery strategies; contemplating the security status district by district was key success factor. Furthermore, program’s resilience was supported by a dedicated, committed, and responsive EPI teams at national and sub-national levels, operating in collaboration and coordination with partners, motivated by a unified vision encapsulated in the slogan “Despite what is happening, vaccination must continue”. Conclusions: To sustain the immunization services in Sudan, the EPI prioritized the cohesion and solidarity of the team, adopting a collaborative approach. This durable essence of unity was especially evident is expanding partnership in security compromised states. VL - 13 IS - 5 ER -
Expanded Program on Immunization, Federal Ministry of Health, Khartoum, Sudan
Faculty of Medicine, University of Khartoum, Khartoum, Sudan
Information