Abstract
Background: Sporadic occurrence of cholera is an epidemiological challenge to identify the source. In last week of November 2016, the World Health Organization (WHO) reported a 32-year-old Bangladeshi male overseas worker developed acute watery diarrhoea en route to Oman and was diagnosed with cholera. As the focal institute of the International Health Regulation (IHR), the Institute of Epidemiology, Disease Control and Research (IEDCR) initiated a retrospective investigation to identify possible sources of Vibrio cholerae exposure at the patient's departure. Methods: The investigation was conducted from December 2-4, 2016. We communicated with the patient's relative and traced the last 6 days of his stay in Bangladesh and his journey from his home village Bheramara subdistrict, Kushtia, to the Hazrat Shahjalal International Airport, Dhaka City, before boarding the aircraft. We interviewed with family members and tracked the patient's food and water exposures during the incubation period. Local subdistrict hospital admission data were reviewed to assess any concurrent outbreak in the locality. Water samples were collected and tested from identified consumption sites. Environmental observations focused on the water distribution infrastructure. Results: Patient was apparently healthy the day before his journey. Patient and his younger brother travelled through public transport to the capital and stayed overnight in a hotel near the airport to catch his flight the next day. Both of them drank supplied water in the residential hotel and restaurant near the airport. The subdistrict hospital surveillance data showed no unusual increase in diarrhoea admissions in patient's community. Five water samples that were collected from village and roadside vendors were tested negative for fecal contamination. However, water samples, collected from hotel and restaurants near the airport, showed the presence of fecal Echerichia coli. Environmental assessments revealed leakages in the water supply lines of the city corporation in Ashkona area. Conclusion: Although not confirmed, the most likely source of the sporadic cholera Vibrio cholerae infection was the contaminated supply water in hotels or restaurants near the airport. We recommend that hotels and restaurants regularly chlorinate their underground and overhead water tanks. The Dhaka city corporation office need to ensure a safe water supply line without any leakage. We also recommended providing health education regarding safe drinking water to the overseas workers.
|
Published in
|
World Journal of Medical Case Reports (Volume 6, Issue 3)
|
|
DOI
|
10.11648/j.wjmcr.20250603.14
|
|
Page(s)
|
38-44 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Cholera, Vibrio Cholerae, Water Microbiology, Fecal Contamination, Disease Outbreaks
1. Introduction
Cholera was once a major public health problem. Still, it poses a threat to human lives, especially in low- and middle-income countries where access to safe drinking water and improved sanitation is limited. Usually, people suffer from cholera after ingestion of food or water contaminated with toxigenic strains of
Vibrio cholerae, a Gram-negative bacterium that colonizes small intestine and induces profuse watery diarrhoea, which may lead to severe dehydration, shock, and even death if left untreated
. Although Bangladesh has strengthened cholera surveillance and control, the country continues to report sporadic cases and seasonal outbreaks
| [2] | Islam MT, Hegde ST, Khan AI, Bhuiyan MTR, Khan ZH, Ahmmed F, et al. National hospital-based sentinel surveillance for cholera in Bangladesh: Epidemiological results from 2014 to 2021. Am J Trop Med Hyg. 2023; 109(3): 575–83. https://doi.org/10.4269/ajtmh.23-0074 |
| [3] | Das JK, Bhutta ZA. Global challenges in diarrheal disease control. Curr Opin Infect Dis. 2020; 33(5): 405–12. https://doi.org/10.1097/MOG.0000000000000236 |
[2, 3]
.
The burden of cholera in Bangladesh is related to environmental, infrastructural, and behavioural factors. Contaminated drinking water, poor waste disposal, and consumption of unhygienic street food are among the leading factors in the transmission of
Vibrio cholerae in both rural and urban areas
. Additionally, city corporations or municipalities have intermittent water supply systems for households, increasing the risk of contamination at distribution endpoints, as occasionally the household creates negative suction pressure to get the water
| [5] | Vachon L, Thériault M, Amini H, Brisson-Carroll G, Wilson J, Cizauskas C, et al. Estimating infection risks and the global burden of diarrheal disease attributable to intermittent water supply using QMRA. Environmental Science & Technology. 2017; 51(18): 10693–703. https://doi.org/10.1021/acs.est.7b01014 |
[5]
. The negative pressure can suck out surrounding contaminated water in the distribution channel if there is any breach.
International travel by labour migrants from endemic regions introduces added complexity to cholera surveillance. In such cases, retrospective investigations sometimes help find out the origin of infection. These investigations also have implications for compliance with the International Health Regulations (IHR), which require timely notification and response to potential public health emergencies of international concern
| [6] | World Health Organization. International Health Regulations (2005). 3rd ed. Geneva: WHO; 2016. |
[6]
.
The poor overseas workers of Bangladesh occasionally need to stay in the cheaper hotels and take food and water from restaurants in Dhaka, the capital, before their final departure. Most of these overseas workers travel from their villages for the first time to Dhaka and lack knowledge regarding safe drinking water. Previous studies in urban Bangladesh have demonstrated that despite widespread outbreaks, localized faecal contamination in drinking water remains common due to infrastructural deficiencies and suboptimal monitoring of sewage and water distribution systems
| [7] | Lantagne D, Clasen T. Point-of-use water treatment in emergency response. Waterlines. 2012; 31(1–2): 30–52. https://doi.org/10.3362/1756-3488.2012.005 |
| [8] | Haque F, Hossain MJ, Kundu SK, Naser AM, Rahman M, Luby SP. Cholera outbreaks in urban Bangladesh in 2011. Epidemiology. 2013; 3: 126. https://doi.org/10.4172/2161-1165.1000126 |
| [9] | Nguyen VD, Sreenivasan N, Lam E, Ayers T, Kargbo D, Dafae F, et al. Cholera epidemic associated with consumption of unsafe drinking water and street-vended water-Freetown, Sierra Leone, 2012. Am J Trop Med Hyg. 2014; 90(3): 518–22. https://doi.org/10.4269/ajtmh.13-0567 |
[7-9]
.
On November 18, 2016, a 32-year-old Bangladeshi male failed to exit the plane at Muscat International Airport, Oman, due to hypovolemic shock, was later referred to the hospital, and diagnosed with cholera. The Institute of Epidemiology, Disease Control and Research (IEDCR) was notified of the event through the IHR National Focal Point in the last week of November 2016. IEDCR immediately initiated an investigation to determine the probable source of infection.
2. Methods
2.1. Investigation Design
We conducted a retrospective field investigation to identify potential sources of Vibrio cholerae exposure. The investigation was initiated by visiting the home village of the patient at Bheramara subdistrict, Kustia District, under Khulna Division. We explored his travel paths from his village, to Dhaka up to his departure from Bangladesh.
2.2. Variables and Case Definitions
The incubation period of cholera is 12 hours to 5 days before the onset of symptoms
. During the incubation period, we searched for sources of raw and cooked food and drinking water. We defined a suspected case as any person who suffered from three or more episodes of loose stool within 24 hours from November 11 – 18, 2016 in the village and other travel locations of the patient. A sporadic case was defined as one in which no clustering or additional cholera cases were detected in the community or travel route during the relevant time window.
2.3. Data Collection
Detailed interviews were conducted with the patient's family members to reconstruct his travel itinerary and dietary history between November 11 – 16, 2016. Hospital admission data for acute watery diarrhoea cases from Bheramara Upazila Health Complex from November 2015 – November, 2016, were reviewed to identify any rise in diarrheal reporting.
2.4. Sample Collection and Laboratory Investigation
Water samples were collected from tube wells in the premises of houses of the patient and his relatives. Additional water samples were collected from water pumps and distribution points at Hazrat Shahjalal International Airport, Dhaka. The samples were tested in the environmental microbiology laboratory of the International Centre for Diarrhoeal Disease Research (icddr,b) for Microbiological testing to detect faecal contamination and the presence of Vibrio cholerae and other coliform organisms.
2.5. Environmental Investigation
Environmental assessments included observations of water storage and supply systems where the patient stayed. An elaborate search of water pipelines to the Ashkona area was performed, where water was distributed to local hotels by the city corporations from the pump to the distribution points.
2.6. Statistical Analysis
Using Microsoft Excel and SATA 12, we performed a descriptive analysis of diarrhoea admission data from hospital records by time, place, and person to identify possible outbreaks in the patient's village or other investigation areas.
2.7. Ethical Considerations
The investigation was conducted as part of the public health response under the authority of IEDCR and the Directorate General of Health Services, Bangladesh. Formal institutional review board approval was not required, as the activity was deemed part of a routine outbreak investigation. No personal identifiers were collected or disclosed. Verbal consent was obtained from all interviewees.
3. Results
The index case was a 32-year-old married male Bangladeshi overseas worker who developed passage of loose watery stool on November 16, 2016, during his transit on his way to Oman. Symptoms developed after he had boarded his flight. Throughout the journey, he had multiple episodes of loose motion and developed severe dehydration. After the flight landed in Oman, he needed to transfer from the airport to the hospital by ambulance. He was treated in the hospital and tested positive for Vibrio cholerae. During the time of the investigation, the patient himself was not available for direct interview as he was abroad. So, all the exposure information was obtained from his wife, parents, siblings and close relatives.
According to family members, the patient was relatively healthy at the time of his travel, and had no known chronic health conditions like diabetes, asthma, or hypertension, and he was a non-smoker. His medical history included motion sickness and irritable bowel syndrome. He had a previous history of working in the United Arab Emirates (UAE) from 2010 – 2011 and Iraq from 2011 - 2013.
The investigation focused on the incubation period for cholera, defined as the five days before symptom onset, from 11th to 16th November 2016. During this period, the patient was in his home village of Ramchandrapur, located in the Bheramara subdistrict of Kushtia district, from November 11 – 14, 2016. He drank tube-well water and ate food prepared at home and by the relatives. The tube-well water was consumed directly without storage. His relatives reported that he had general awareness of personal hygiene and did not have any diarrheal diseases recently. Interviews with neighbours and family members indicated that no other individuals in the village had developed diarrhoea in November 2016.
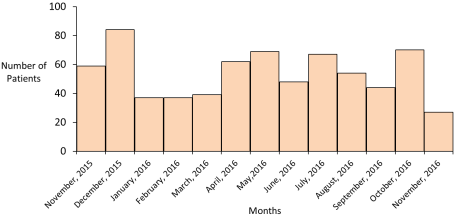
Residents of the village usually sought medical care from the Bheramara Upazila Health Complex, a government health facility, situated approximately four kilometers from the village. Hospital admission records from Bheramara Upazila Health Complex were reviewed to assess the presence of a possible outbreak. Data from November 2015 to November 2016 revealed no abnormal rise in diarrhea admissions among individuals older than five years (
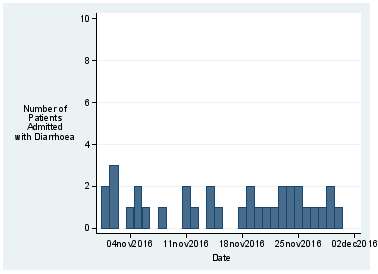
Figure 1). Similarly, no increase in diarrheal cases was recorded between November 1 – 30, 2016, suggesting that no cluster of cholera cases or outbreak activity occurred in the area during that period (
Figure 2).
Figure 1. Number of daily diarrhoea patients (> 5 years old) admitted in Upazila Health Complex, Bheramara.
On November 15, 2016, he travelled to Dhaka to catch his outbound flight. During his journey, the patient stopped at several locations to take food. On the way to Dhaka, he consumed food and water from a roadside tea stall. He stayed in a residential hotel in the Ashkona area of Dhaka City, which was located within two kilometers of Hazrat Shahjalal International Airport. There he took food and drank water from two restaurants along with the residential hotel. We interviewed nine boarders from the hotel registrar, who stayed at the same residential hotel from November 15 – 16, 2016. We found none of them had any symptoms of diarrhoea during or within five days of their stay.
Nine water samples were collected for microbiological testing from sources the patient reportedly consumed during the incubation period. These included two tube-well samples from the patient's village, two samples from the Dhaka airport water system (one from the pump and another from the distribution point), one sample of filtered water from a tea stall in Dhaka, one sample from a water pump (Ashkona Area), and three samples from distribution taps in hotels and restaurants where the index case stayed his last night before board to flight.
Figure 2. Number of daily diarrhoea patients (> 5 years old) admitted in Bheramara Upazila health complex from November 1 -30, 2016.
Laboratory examination showed that water samples collected from the village, airport, and tea stall, were free of faecal contamination. Similarly, the pump water sample from Ashkona tested negative for faecal contamination. However, all three samples collected from the distribution points within the hotels and restaurants in Ashkona showed the presence of
Escherichia coli. And none of the water samples tested positive for
Vibrio cholerae (
Table 1).
These restaurants and residential hotels received their water from the Dhaka Water Supply and Sewerage Authority (WASA). Dhaka WASA used to collect groundwater and river water by pumps. This water was followed several steps of cleaning and chlorination and stored in overhead tanks. The water was distributed to houses, hotels, restaurants and all types of facilities through an enclosed pipeline system. Dhaka WASA supplied water intermittently, occasionally at night for a few hours in a day. An environmental assessment at the Ashkona area revealed that water distribution pipelines were located near open drains and appeared vulnerable to leakage and potential cross-contamination. The water was supplied intermittently and most of the time required mechanical suction to draw water from the distribution pipes into the reservoirs of buildings. It created a negative suction in pipelines through which contaminants from the surroundings of the pipelines had a high chance of intrusion.
Table 1. Findings of water samples collected from the sites where the patient drank water 12 hours to 5 days before the onset of illness.
Serial | Site of collection | Sources of samples | Number of water samples | Findings |
1 | Patients' village | Tube well | 02 | Free of contamination |
2 | Hazrat Shahjalal International Airport, Dhaka | Pump water | 01 | Free of contamination |
3 | Hajrat Shahjalal International Airport, Dhaka | Distribution point | 01 | Free of contamination |
4 | Tea stall at the bus stand of Dhaka city | Filter water | 01 | Free of contamination |
5 | Ashkona area of Dhaka City | Pump water | 01 | Free of contamination |
6 | Ashkona area of Dhaka City | Hotels and restaurants | 03 | Fecal contamination found |
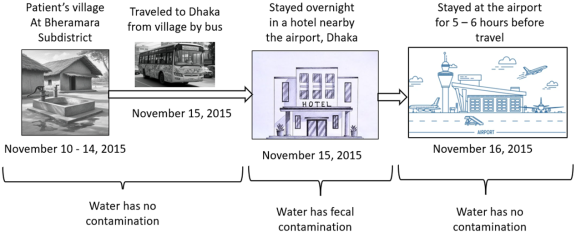
These findings and water sample reports suggested no evidence of a cholera outbreak or contamination in the patient’s home village or the areas he visited during travel. Although
Vibrio cholerae was not detected in any sample, the presence of fecal contamination in the hotel and restaurant water supplies in Ashkona indicated a potential risk for enteric disease transmission through the local distribution system (
Figure 3).
Figure 3. Schematic presentation of possible exposure for the infection of the patient.
4. Discussions
This retrospective investigation sought to determine the likely source of cholera infection in a middle-aged Bangladeshi overseas worker who developed acute watery diarrhea while traveling to Oman in November 2016. The patient's illness was confirmed by the presence of Vibrio cholerae in his stool during his admission to a hospital in Oman. Epidemiological data collected from his village of residence and transit route to the airport, in combination with microbiological testing of water sources, allowed us to evaluate potential exposures during the incubation period. While no outbreak was identified, and Vibrio cholerae was not isolated from any water samples, Escherichia coli was found in the city corporation supply water in the restaurants and residential hotels of Ashkona area of Dhaka City.
The investigation team did not find any concurrent cholera case in the patient's home village, Ramchandrapur, or the wider Bheramara subdistrict. Analysis of hospital admission data for diarrhoea during November 2016 demonstrated stable trends consistent with seasonal background levels. Interviews with family and community members further supported the absence of diarrheal clusters. These findings suggest that the case was not part of a community outbreak and likely represents a sporadic infection. Previous studies in rural Bangladesh have shown that community-level transmission of cholera is usually accompanied by a rise in local healthcare visits for diarrhoea, often concentrated in a short window of time
| [10] | Faruque AS, Eusof A. Medical care utilization prior to death in cholera outbreaks in rural Bangladesh. Trop Doct. 1986 Apr; 16(2): 87-9. https://doi.org/10.1177/004947558601600217 |
| [11] | Alam M, Hasan NA, Sadique A, Bhuiyan NA, Ahmed KU, Nusrin S, et al. Seasonal cholera caused by Vibrio cholerae serogroups O1 and O139 in the coastal aquatic environment of Bangladesh. Appl Environ Microbiol. 2006; 72(6): 4096–104. https://doi.org/10.1128/AEM.00066-06 |
[10, 11]
. In this case, the absence of such a pattern strengthens the conclusion that the patient's village was not the source of exposure.
The patient consumed food and water from multiple sources while traveling from Kushtia to Dhaka and staying in the Ashkona area of Dhaka city. The water samples, collected from his home village, the airport, and a local tea stall, were free from faecal contamination. The water samples, colleted from hotel and restaurants in Ashkona area, tested positive for faecal indicator bacteria like
Escherichia coli. This was consistent with earlier findings in Dhaka, where faecal contamination was frequently identified in distributed drinking water, even when the source water from WASA's central supply remained clear of coliform
| [12] | Mahbub KR, Nahar A, Ahmed MM, Chakraborty A. Quality analysis of Dhaka WASA drinking water: detection and microbial contamination. J Environ Sci Natural Resour. 2012; 4(2): 41–9. https://doi.org/10.3329/jesnr.v4i2.10133 |
| [13] | Sirajul Islam M, Brooks A, Kabir MS, Jahid IK, Shafiqul Islam M, Goswami D, et al. Faecal contamination of drinking water sources of Dhaka city during the 2004 flood in Bangladesh and use of disinfectants for water treatment. J Appl Microbiol. 2007; 103(1): 80–7. https://doi.org/10.1111/j.1365-2672.2006.03234.x |
[12, 13]
.
The contamination of water at the distribution points in Ashkona were attributed to infrastructure-related issues of water supply lines. In intermittent water supply systems of Dhaka WASA, and the use of mechanical pumps were commonly generated negative pressure at the consumer end to draw sufficient water through the distribution lines. This setup had increased the risk of introducing contaminants from surrounding soil or wastewater systems, where leakages or illegal connections were common
| [14] | Trevett AF, Carter RC, Tyrrel SF. Water quality deterioration: a study of household drinking water quality in rural Honduras. Int J Environ Health Res. 2004; 14(4): 273–83. https://doi.org/10.1080/09603120410001725612 |
[14]
. A study by Naser et al. (2017) found that in urban slums of Dhaka, nearly 59% of household storage containers and tap outlets tested positive for faecal coliforms, despite relatively clean source water by Dhaka WASA
| [5] | Vachon L, Thériault M, Amini H, Brisson-Carroll G, Wilson J, Cizauskas C, et al. Estimating infection risks and the global burden of diarrheal disease attributable to intermittent water supply using QMRA. Environmental Science & Technology. 2017; 51(18): 10693–703. https://doi.org/10.1021/acs.est.7b01014 |
[5]
. Similarly, environmental mapping in Mirpur and Hazaribagh demonstrated that pipelines near open drains or latrines were significantly more likely to yield contaminated samples
.
Although
Vibrio cholerae was not isolated from the tested samples, its absence does not rule out the possibility of prior exposure. The retrospective nature of this investigation meant that environmental sampling occurred more than two weeks following possible exposure of the patient. Given the known fragility of
Vibrio cholerae in environmental samples and its episodic shedding in contaminated water, delayed sample collection likely reduced the probability of detecting the organism
| [15] | Huq A, Sack RB, Nizam A, Longini IM, Nair GB, Ali A, et al. Critical factors influencing the occurrence of Vibrio cholerae in the environment of Bangladesh. Appl Environ Microbiol. 2005; 71(8): 4645–54. https://doi.org/10.1128/AEM.71.8.4645-4654.2005 |
[15]
. In similar investigations conducted during the cholera epidemic in Sierra Leone in 2012, the investigators could not isolate
Vibrio cholerae from suspected water sources, despite strong epidemiological links to the specific sites of exposure
| [9] | Nguyen VD, Sreenivasan N, Lam E, Ayers T, Kargbo D, Dafae F, et al. Cholera epidemic associated with consumption of unsafe drinking water and street-vended water-Freetown, Sierra Leone, 2012. Am J Trop Med Hyg. 2014; 90(3): 518–22. https://doi.org/10.4269/ajtmh.13-0567 |
[9]
.
The case raised broader concerns about travel-related transmission risks among outbound international workers. Labor migrants frequently move through multiple urban settings and transit hubs before departure, and often rely on affordable food and lodging options near airports. If unregulated or inadequately monitored, these environments can pose significant health risks. Previous reports from Bangladesh and other endemic settings have documented cases of diarrhoea strongly linked to street-vended food and low-cost hotel meals consumed by travellers
| [16] | Nizame FA, Alam MU, Masud AA, Shoab AK, Opel A, Islam MK, et al. Hygiene in restaurants and among street food vendors in Bangladesh. Am J Trop Med Hyg. 2019; 101(3): 566–75. https://doi.org/10.4269/ajtmh.18-0896 |
| [17] | Taylor DL, Kahawita TM, Cairncross S, Ensink JHJ. The impact of water, sanitation and hygiene interventions to control cholera: a systematic review. PLoS One. 2015; 10(8): e0135676. https://doi.org/10.1371/journal.pone.0135676 |
[16, 17]
. These findings underscore the need for strengthened regulation and oversight of food and water safety standards in high-traffic areas.
This investigation had several limitations. First, the absence of direct interviews with the patient may have introduced recall bias or incomplete reporting of exposures. Second, due to the retrospective, we could not collect food and water samples, which might have also served as vehicles of Vibrio cholerae transmission. The water samples were only tested for microbiology; however, we could not measure the amount of free residual chlorine in the supply water. We could not collect samples from from the employees or work surfaces in food preparation areas. Third, environmental testing was limited to a single time point and may not reflect the contamination status during the actual exposure window. Finally, while the sample size of nine water sources provides reasonable coverage of the patient's exposure route, it may not capture all relevant sources of infection.
Despite these limitations, the findings offered important insights for public health planning. The faecal contamination in water samples from the Ashkona distribution system suggested systematic weaknesses in the urban water distribution system, particularly in commercial zones near major transport hubs. Improving the integrity of water distribution lines, enforcing routine inspection for leakage, and preventing illegal connections were critical steps to mitigate contamination risks. In addition, overseas workers and travelers should be educated on personal hygiene, safe food practices, and the use of bottled or treated water during transit.
5. Conclusion
In conclusion, while the cholera case in this overseas worker was classified as sporadic, the presence of faecal contamination in multiple water samples from distribution points in Dhaka city, especially in the hotels of the airport area, highlighted the risk of infection of overseas workers during travelling abroad. Strengthening routine monitoring of water quality in the restaurants and residential hotels surrounding the airport areas of Daka city and incorporating targeted hygiene education for outbound travellers may reduce the risk of similar events in the future.
Abbreviations
icddr,b | International Centre for Diarrhoeal Disease Research, Bangladesh |
IEDCR | Institute of Epidemiology, Disease Control and Research |
IHR | International Health Regulations |
SOP | Standard Operating Procedure |
WASA | Water Supply and Sewerage Authority |
WHO | World Health Organization |
Acknowledgments
The authors acknowledge the support from patients' relatives in sharing their travel history to complete the investigation. We are also grateful to Bheramara Upazila Health Complex, Dhaka City Corporation staff and the Ashkona area hotel staff for providing key information to the inquiry. Authors also acknowledge the International Centre for Diarrhoeal Disease Research, Bangladesh and the Institute of Epidemiology, Disease Control and Research (IEDCR) for providing laboratory support and logistics for the investigation.
Author Contributions
Mallick Masum Billah: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Kazi Munisul Islam: Data curation, Investigation, Methodology, Visualization, Writing – review & editing
ASM Alamgir: Investigation, Methodology, Project administration, Resources, Writing – review & editing
Meerjady Sabrina Flora: Methodology, Project administration, Supervision, Validation, Writing – review & editing
Funding
The authors declare that there is no fund received to conduct the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Ali M, Nelson AR, Lopez AL, Sack DA. Updated global burden of cholera in endemic countries. PLoS Negl Trop Dis. 2015; 9(6): e0003832.
https://doi.org/10.1371/journal.pntd.0003832
|
| [2] |
Islam MT, Hegde ST, Khan AI, Bhuiyan MTR, Khan ZH, Ahmmed F, et al. National hospital-based sentinel surveillance for cholera in Bangladesh: Epidemiological results from 2014 to 2021. Am J Trop Med Hyg. 2023; 109(3): 575–83.
https://doi.org/10.4269/ajtmh.23-0074
|
| [3] |
Das JK, Bhutta ZA. Global challenges in diarrheal disease control. Curr Opin Infect Dis. 2020; 33(5): 405–12.
https://doi.org/10.1097/MOG.0000000000000236
|
| [4] |
Harris JB, LaRocque RC, Qadri F, Ryan ET, Calderwood SB. Cholera. Lancet. 2012; 379(9835): 2466–76.
https://doi.org/10.1016/S0140-6736(12)60436-X
|
| [5] |
Vachon L, Thériault M, Amini H, Brisson-Carroll G, Wilson J, Cizauskas C, et al. Estimating infection risks and the global burden of diarrheal disease attributable to intermittent water supply using QMRA. Environmental Science & Technology. 2017; 51(18): 10693–703.
https://doi.org/10.1021/acs.est.7b01014
|
| [6] |
World Health Organization. International Health Regulations (2005). 3rd ed. Geneva: WHO; 2016.
|
| [7] |
Lantagne D, Clasen T. Point-of-use water treatment in emergency response. Waterlines. 2012; 31(1–2): 30–52.
https://doi.org/10.3362/1756-3488.2012.005
|
| [8] |
Haque F, Hossain MJ, Kundu SK, Naser AM, Rahman M, Luby SP. Cholera outbreaks in urban Bangladesh in 2011. Epidemiology. 2013; 3: 126.
https://doi.org/10.4172/2161-1165.1000126
|
| [9] |
Nguyen VD, Sreenivasan N, Lam E, Ayers T, Kargbo D, Dafae F, et al. Cholera epidemic associated with consumption of unsafe drinking water and street-vended water-Freetown, Sierra Leone, 2012. Am J Trop Med Hyg. 2014; 90(3): 518–22.
https://doi.org/10.4269/ajtmh.13-0567
|
| [10] |
Faruque AS, Eusof A. Medical care utilization prior to death in cholera outbreaks in rural Bangladesh. Trop Doct. 1986 Apr; 16(2): 87-9.
https://doi.org/10.1177/004947558601600217
|
| [11] |
Alam M, Hasan NA, Sadique A, Bhuiyan NA, Ahmed KU, Nusrin S, et al. Seasonal cholera caused by Vibrio cholerae serogroups O1 and O139 in the coastal aquatic environment of Bangladesh. Appl Environ Microbiol. 2006; 72(6): 4096–104.
https://doi.org/10.1128/AEM.00066-06
|
| [12] |
Mahbub KR, Nahar A, Ahmed MM, Chakraborty A. Quality analysis of Dhaka WASA drinking water: detection and microbial contamination. J Environ Sci Natural Resour. 2012; 4(2): 41–9.
https://doi.org/10.3329/jesnr.v4i2.10133
|
| [13] |
Sirajul Islam M, Brooks A, Kabir MS, Jahid IK, Shafiqul Islam M, Goswami D, et al. Faecal contamination of drinking water sources of Dhaka city during the 2004 flood in Bangladesh and use of disinfectants for water treatment. J Appl Microbiol. 2007; 103(1): 80–7.
https://doi.org/10.1111/j.1365-2672.2006.03234.x
|
| [14] |
Trevett AF, Carter RC, Tyrrel SF. Water quality deterioration: a study of household drinking water quality in rural Honduras. Int J Environ Health Res. 2004; 14(4): 273–83.
https://doi.org/10.1080/09603120410001725612
|
| [15] |
Huq A, Sack RB, Nizam A, Longini IM, Nair GB, Ali A, et al. Critical factors influencing the occurrence of Vibrio cholerae in the environment of Bangladesh. Appl Environ Microbiol. 2005; 71(8): 4645–54.
https://doi.org/10.1128/AEM.71.8.4645-4654.2005
|
| [16] |
Nizame FA, Alam MU, Masud AA, Shoab AK, Opel A, Islam MK, et al. Hygiene in restaurants and among street food vendors in Bangladesh. Am J Trop Med Hyg. 2019; 101(3): 566–75.
https://doi.org/10.4269/ajtmh.18-0896
|
| [17] |
Taylor DL, Kahawita TM, Cairncross S, Ensink JHJ. The impact of water, sanitation and hygiene interventions to control cholera: a systematic review. PLoS One. 2015; 10(8): e0135676.
https://doi.org/10.1371/journal.pone.0135676
|
Cite This Article
-
APA Style
Billah, M. M., Islam, K. M., Alamgir, A., Flora, M. S. (2025). Retrospective Field Investigation of a Cholera Case in Bangladesh Following IHR Notification. World Journal of Medical Case Reports, 6(3), 38-44. https://doi.org/10.11648/j.wjmcr.20250603.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Billah, M. M.; Islam, K. M.; Alamgir, A.; Flora, M. S. Retrospective Field Investigation of a Cholera Case in Bangladesh Following IHR Notification. World J. Med. Case Rep. 2025, 6(3), 38-44. doi: 10.11648/j.wjmcr.20250603.14
Copy
|
Download
AMA Style
Billah MM, Islam KM, Alamgir A, Flora MS. Retrospective Field Investigation of a Cholera Case in Bangladesh Following IHR Notification. World J Med Case Rep. 2025;6(3):38-44. doi: 10.11648/j.wjmcr.20250603.14
Copy
|
Download
-
@article{10.11648/j.wjmcr.20250603.14,
author = {Mallick Masum Billah and Kazi Munisul Islam and ASM Alamgir and Meerjady Sabrina Flora},
title = {Retrospective Field Investigation of a Cholera Case in Bangladesh Following IHR Notification
},
journal = {World Journal of Medical Case Reports},
volume = {6},
number = {3},
pages = {38-44},
doi = {10.11648/j.wjmcr.20250603.14},
url = {https://doi.org/10.11648/j.wjmcr.20250603.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20250603.14},
abstract = {Background: Sporadic occurrence of cholera is an epidemiological challenge to identify the source. In last week of November 2016, the World Health Organization (WHO) reported a 32-year-old Bangladeshi male overseas worker developed acute watery diarrhoea en route to Oman and was diagnosed with cholera. As the focal institute of the International Health Regulation (IHR), the Institute of Epidemiology, Disease Control and Research (IEDCR) initiated a retrospective investigation to identify possible sources of Vibrio cholerae exposure at the patient's departure. Methods: The investigation was conducted from December 2-4, 2016. We communicated with the patient's relative and traced the last 6 days of his stay in Bangladesh and his journey from his home village Bheramara subdistrict, Kushtia, to the Hazrat Shahjalal International Airport, Dhaka City, before boarding the aircraft. We interviewed with family members and tracked the patient's food and water exposures during the incubation period. Local subdistrict hospital admission data were reviewed to assess any concurrent outbreak in the locality. Water samples were collected and tested from identified consumption sites. Environmental observations focused on the water distribution infrastructure. Results: Patient was apparently healthy the day before his journey. Patient and his younger brother travelled through public transport to the capital and stayed overnight in a hotel near the airport to catch his flight the next day. Both of them drank supplied water in the residential hotel and restaurant near the airport. The subdistrict hospital surveillance data showed no unusual increase in diarrhoea admissions in patient's community. Five water samples that were collected from village and roadside vendors were tested negative for fecal contamination. However, water samples, collected from hotel and restaurants near the airport, showed the presence of fecal Echerichia coli. Environmental assessments revealed leakages in the water supply lines of the city corporation in Ashkona area. Conclusion: Although not confirmed, the most likely source of the sporadic cholera Vibrio cholerae infection was the contaminated supply water in hotels or restaurants near the airport. We recommend that hotels and restaurants regularly chlorinate their underground and overhead water tanks. The Dhaka city corporation office need to ensure a safe water supply line without any leakage. We also recommended providing health education regarding safe drinking water to the overseas workers.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Retrospective Field Investigation of a Cholera Case in Bangladesh Following IHR Notification
AU - Mallick Masum Billah
AU - Kazi Munisul Islam
AU - ASM Alamgir
AU - Meerjady Sabrina Flora
Y1 - 2025/09/26
PY - 2025
N1 - https://doi.org/10.11648/j.wjmcr.20250603.14
DO - 10.11648/j.wjmcr.20250603.14
T2 - World Journal of Medical Case Reports
JF - World Journal of Medical Case Reports
JO - World Journal of Medical Case Reports
SP - 38
EP - 44
PB - Science Publishing Group
SN - 2994-726X
UR - https://doi.org/10.11648/j.wjmcr.20250603.14
AB - Background: Sporadic occurrence of cholera is an epidemiological challenge to identify the source. In last week of November 2016, the World Health Organization (WHO) reported a 32-year-old Bangladeshi male overseas worker developed acute watery diarrhoea en route to Oman and was diagnosed with cholera. As the focal institute of the International Health Regulation (IHR), the Institute of Epidemiology, Disease Control and Research (IEDCR) initiated a retrospective investigation to identify possible sources of Vibrio cholerae exposure at the patient's departure. Methods: The investigation was conducted from December 2-4, 2016. We communicated with the patient's relative and traced the last 6 days of his stay in Bangladesh and his journey from his home village Bheramara subdistrict, Kushtia, to the Hazrat Shahjalal International Airport, Dhaka City, before boarding the aircraft. We interviewed with family members and tracked the patient's food and water exposures during the incubation period. Local subdistrict hospital admission data were reviewed to assess any concurrent outbreak in the locality. Water samples were collected and tested from identified consumption sites. Environmental observations focused on the water distribution infrastructure. Results: Patient was apparently healthy the day before his journey. Patient and his younger brother travelled through public transport to the capital and stayed overnight in a hotel near the airport to catch his flight the next day. Both of them drank supplied water in the residential hotel and restaurant near the airport. The subdistrict hospital surveillance data showed no unusual increase in diarrhoea admissions in patient's community. Five water samples that were collected from village and roadside vendors were tested negative for fecal contamination. However, water samples, collected from hotel and restaurants near the airport, showed the presence of fecal Echerichia coli. Environmental assessments revealed leakages in the water supply lines of the city corporation in Ashkona area. Conclusion: Although not confirmed, the most likely source of the sporadic cholera Vibrio cholerae infection was the contaminated supply water in hotels or restaurants near the airport. We recommend that hotels and restaurants regularly chlorinate their underground and overhead water tanks. The Dhaka city corporation office need to ensure a safe water supply line without any leakage. We also recommended providing health education regarding safe drinking water to the overseas workers.
VL - 6
IS - 3
ER -
Copy
|
Download