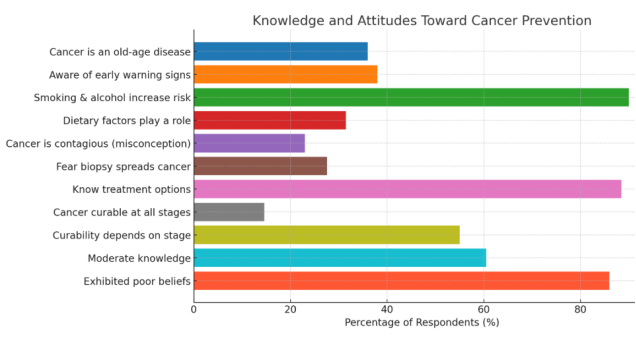
Background: Cancer remains a significant public health concern in Nigeria. Awareness and early detection are critical for reducing morbidity and mortality. This study assessed the knowledge, beliefs, and preventive practices related to cancer among civil servants in Abia State, Nigeria. Methods: A cross-sectional survey was conducted among 364 civil servants using a structured questionnaire. Knowledge, beliefs, and practice were scored and categorized as "good" or "poor." Data were analyzed using descriptive statistics, chi-square tests, and logistic regression to determine the associations between demographic variables and cancer-related knowledge, attitudes, and practices (KAP). Results: While 63.1% of respondents had good knowledge of cancer causes and warning signs, only 46.2% reported engaging in preventive practices such as routine screening and lifestyle modification. Preventive behaviors were lowest for mammography (12.6%), cervical screening (21.7%), and colonoscopy (7.4%). Although 90% recognized smoking and alcohol as risk factors, 86.5% held at least one poor belief, including the views that cancer is contagious (23.1%) or that biopsies spread cancer (27.6%). Logistic regression analysis revealed that higher education was a significant predictor of good knowledge (p < 0.01), while age and the number of children were significant predictors of practice level (p < 0.05). Conclusion: Despite moderate awareness, preventive behaviors remain suboptimal. Myths and poor beliefs persist, undermining early detection. Health promotion should focus on correcting false beliefs and increasing access to screening programs.
| Published in | World Journal of Public Health (Volume 10, Issue 2) |
| DOI | 10.11648/j.wjph.20251002.21 |
| Page(s) | 187-192 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Cancer Awareness, Prevention, Civil Servants, Nigeria, Early Detection, Public Health
Variable | Category | Practice = Yes, n (%) | Practice = No, n (%) |
|---|---|---|---|
Age group | 18–24 | 57 (82.6) | 12 (17.4) |
25–34 | 77 (74.8) | 26 (25.2) | |
35–44 | 78 (87.6) | 11 (12.4) | |
≥45 | 27 (69.2) | 12 (30.8) | |
Chi-square (df=3) | – | – | |
p-value | – | 0.046 | |
Gender | Female | 204 (81.0) | 48 (19.0) |
Male | 35 (72.9) | 13 (27.1) | |
χ² (df=1) | – | – | |
p-value | – | 0.284 | |
Education level | No formal | 11 (42.3) | 15 (57.7) |
Primary | 53 (69.7) | 23 (30.3) | |
Secondary | 127 (86.4) | 20 (13.6) | |
Tertiary | 48 (94.1) | 3 (5.9) | |
χ² (df=3) | – | – | |
p-value | – | <0.001 | |
Knowledge level | Good | 176 (91.7) | 16 (8.3) |
Poor | 63 (58.3) | 45 (41.7) | |
χ² (df=1) | – | – | |
p-value | – | <0.001 |
Predictor (reference) | OR (95% CI) | p-value |
|---|---|---|
Gender (Male vs Female) | 0.54 (0.24–1.25) | 0.150 |
Age 25–34 vs 18–24 | 0.54 (0.22–1.29) | 0.166 |
Age 35–44 vs 18–24 | 1.28 (0.47–3.46) | 0.629 |
Age ≥45 vs 18–24 | 0.45 (0.15–1.33) | 0.147 |
Education Primary vs No formal | 2.30 (0.82–6.46) | 0.113 |
Education Secondary vs No formal | 6.45 (2.35–17.71) | <0.001 |
Education Tertiary vs No formal | 8.20 (1.80–37.40) | 0.007 |
Knowledge Poor vs Good | 0.15 (0.08–0.30) | <0.001 |
Misconception | Yes n (%) | No n (%) |
|---|---|---|
Biopsy spreads cancer | 200 (55.0) | 164 (45.0) |
Cancer is contagious | 150 (41.2) | 214 (58.8) |
Age group (years) | Misconception Yes n (%) | Misconception No n (%) |
|---|---|---|
18–30 | 92 (79.3) | 24 (20.7) |
31–50 | 139 (85.3) | 24 (14.7) |
>50 | 81 (95.3) | 4 (4.7) |
Sex | Misconception Yes n (%) | Misconception No n (%) |
|---|---|---|
Female | 160 (87.4) | 23 (12.6) |
Male | 152 (84.0) | 29 (16.0) |
Education (highest level) | Misconception Yes n (%) | Misconception No n (%) |
|---|---|---|
Low (primary/none) | 101 (88.6) | 13 (11.4) |
Medium (secondary) | 161 (86.6) | 25 (13.4) |
High (tertiary) | 50 (78.1) | 14 (21.9) |
Knowledge level | Misconception Yes n (%) | Misconception No n (%) |
|---|---|---|
Low | 99 (90.0) | 11 (10.0) |
High | 213 (83.9) | 41 (16.1) |
Predictor | OR (95% CI) | p-value |
|---|---|---|
Age 31–50 vs 18–30 | 1.58 (0.83–2.99) | 0.165 |
Age >50 vs 18–30 | 5.37 (1.78–16.25) | 0.003 |
Male vs Female | 0.79 (0.43–1.45) | 0.448 |
Education (Medium vs Low) | 0.85 (0.41–1.77) | 0.666 |
Education (High vs Low) | 0.42 (0.18–0.99) | 0.047 |
Knowledge (High vs Low) | 0.53 (0.25–1.10) | 0.089 |
AOR | Adjusted Odds Ratio |
CI | Confidence Interval |
HIV | Human Immunodeficiency Virus |
KAP | Knowledge, Attitude, and Practice |
LGA | Local Government Area |
LMICs | Low- and Middle-income Countries |
NCDs | Non-communicable Diseases |
OR | Odds Ratio |
SPSS | Statistical Package for the Social Sciences |
WHO | World Health Organization |
| [1] | Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates. CA Cancer J Clin. 2021; 71(3): 209–249. |
| [2] | Bray F, Laversanne M, Weiderpass E, Soerjomataram I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer. 2021; 127(16): 3029–3030. |
| [3] | Nigeria Federal Ministry of Health. National Cancer Control Plan 2018–2022. Abuja: FMoH; 2018. |
| [4] | Akokuwebe ME, Idemudia ES. Women's knowledge and attitudes towards cervical cancer screening in Nigeria: a scoping review. BMC Public Health. 2021; 21: 1985. |
| [5] | Adeloye D, David RA, Aderemi AV, et al. An estimate of the incidence of breast cancer in Africa: a systematic review and meta-analysis. J Glob Health. 2018; 8(1): 010419. |
| [6] | Ogunwale A, Ndikom CM. Knowledge, attitude and practice of breast cancer early detection among women in a semi-urban area of Nigeria. Afr J Reprod Health. 2020; 24(2): 102–110. |
| [7] | Ezechi OC, Musa ZA, David AN, et al. Awareness and knowledge of child sexual abuse among mothers in Enugu, Nigeria. Pan Afr Med J. 2022; 42: 186. |
| [8] | Nwabueze SA, Adogu POU, Ilika AL. Health beliefs and cancer screening behaviors among women in South-East Nigeria. Niger J Clin Pract. 2014; 17(2): 165–171. |
| [9] | Iliyasu Z, Abubakar IS, Galadanci HS, et al. Cervical cancer risk perception and screening uptake among women in northern Nigeria. BMC Public Health. 2021; 21: 1632. |
| [10] | Duru CB, Iwu AC, Diwe KC, et al. Awareness, perception and utilization of cancer screening services among adults in Imo State, Nigeria. Int J Med Health Dev. 2018; 23(2): 71–82. |
| [11] | Adefuye PO, Brimah A, Adeyemi AO, et al. Socioeconomic determinants of barriers to cervical cancer screening in rural and urban Nigerian women. J Public Health Afr. 2022; 13: 2057. |
| [12] | Ifegwu OJ, Nwobi EA, Ekwueme CO, et al. Knowledge, beliefs and barriers to cervical cancer screening among women in South-East Nigeria: a qualitative study. BMC Women's Health. 2022; 22: 276. |
| [13] | Wako E, Desalegn D, Adamu A. Misconceptions and barriers toward cervical cancer screening among women in Ethiopia: a qualitative study. Front Public Health. 2023; 11: 1102090. |
| [14] | Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011; 155(2): 97–107. |
| [15] | Yaya S, Uthman OA, Amouzou A, et al. Inequalities in awareness and attitude toward cancer screening: evidence from Nigerian Demographic and Health Survey. BMC Public Health. 2021; 21: 1791. |
| [16] | Chukwu EO, Odimegwu C, Ntoimo LFC, Ajayi AI. Factors associated with parental knowledge of child sexual abuse in sub-Saharan Africa: a scoping review. BMC Public Health. 2022; 22: 1211. |
| [17] | World Health Organization. Nigeria cancer profile. WHO; 2022. https://gco.iarc.who.int/media/globocan/factsheets/populations/566-nigeria-fact-sheet.pdf |
APA Style
Ijeoma, N., Nwadiuto, I. (2025). Cancer Prevention Knowledge, Practices, and Misconceptions Among Civil Servants in Abia State, Nigeria: A Cross-sectional Analysis. World Journal of Public Health, 10(2), 187-192. https://doi.org/10.11648/j.wjph.20251002.21
ACS Style
Ijeoma, N.; Nwadiuto, I. Cancer Prevention Knowledge, Practices, and Misconceptions Among Civil Servants in Abia State, Nigeria: A Cross-sectional Analysis. World J. Public Health 2025, 10(2), 187-192. doi: 10.11648/j.wjph.20251002.21
@article{10.11648/j.wjph.20251002.21,
author = {Nduka Ijeoma and Ifeoma Nwadiuto},
title = {Cancer Prevention Knowledge, Practices, and Misconceptions Among Civil Servants in Abia State, Nigeria: A Cross-sectional Analysis},
journal = {World Journal of Public Health},
volume = {10},
number = {2},
pages = {187-192},
doi = {10.11648/j.wjph.20251002.21},
url = {https://doi.org/10.11648/j.wjph.20251002.21},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251002.21},
abstract = {Background: Cancer remains a significant public health concern in Nigeria. Awareness and early detection are critical for reducing morbidity and mortality. This study assessed the knowledge, beliefs, and preventive practices related to cancer among civil servants in Abia State, Nigeria. Methods: A cross-sectional survey was conducted among 364 civil servants using a structured questionnaire. Knowledge, beliefs, and practice were scored and categorized as "good" or "poor." Data were analyzed using descriptive statistics, chi-square tests, and logistic regression to determine the associations between demographic variables and cancer-related knowledge, attitudes, and practices (KAP). Results: While 63.1% of respondents had good knowledge of cancer causes and warning signs, only 46.2% reported engaging in preventive practices such as routine screening and lifestyle modification. Preventive behaviors were lowest for mammography (12.6%), cervical screening (21.7%), and colonoscopy (7.4%). Although 90% recognized smoking and alcohol as risk factors, 86.5% held at least one poor belief, including the views that cancer is contagious (23.1%) or that biopsies spread cancer (27.6%). Logistic regression analysis revealed that higher education was a significant predictor of good knowledge (p < 0.01), while age and the number of children were significant predictors of practice level (p < 0.05). Conclusion: Despite moderate awareness, preventive behaviors remain suboptimal. Myths and poor beliefs persist, undermining early detection. Health promotion should focus on correcting false beliefs and increasing access to screening programs.},
year = {2025}
}
TY - JOUR T1 - Cancer Prevention Knowledge, Practices, and Misconceptions Among Civil Servants in Abia State, Nigeria: A Cross-sectional Analysis AU - Nduka Ijeoma AU - Ifeoma Nwadiuto Y1 - 2025/06/25 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251002.21 DO - 10.11648/j.wjph.20251002.21 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 187 EP - 192 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251002.21 AB - Background: Cancer remains a significant public health concern in Nigeria. Awareness and early detection are critical for reducing morbidity and mortality. This study assessed the knowledge, beliefs, and preventive practices related to cancer among civil servants in Abia State, Nigeria. Methods: A cross-sectional survey was conducted among 364 civil servants using a structured questionnaire. Knowledge, beliefs, and practice were scored and categorized as "good" or "poor." Data were analyzed using descriptive statistics, chi-square tests, and logistic regression to determine the associations between demographic variables and cancer-related knowledge, attitudes, and practices (KAP). Results: While 63.1% of respondents had good knowledge of cancer causes and warning signs, only 46.2% reported engaging in preventive practices such as routine screening and lifestyle modification. Preventive behaviors were lowest for mammography (12.6%), cervical screening (21.7%), and colonoscopy (7.4%). Although 90% recognized smoking and alcohol as risk factors, 86.5% held at least one poor belief, including the views that cancer is contagious (23.1%) or that biopsies spread cancer (27.6%). Logistic regression analysis revealed that higher education was a significant predictor of good knowledge (p < 0.01), while age and the number of children were significant predictors of practice level (p < 0.05). Conclusion: Despite moderate awareness, preventive behaviors remain suboptimal. Myths and poor beliefs persist, undermining early detection. Health promotion should focus on correcting false beliefs and increasing access to screening programs. VL - 10 IS - 2 ER -
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Department of Community Medicine, Rivers State University, Port Harcourt, Nigeria
Information