Existing evidence suggests a strong correlation between nonalcoholic fatty liver disease (NAFLD) risk and dietary factors, and this investigation aimed to examine the association between dietary factors and NAFLD risk in American adults. Utilizing data from the National Health and Nutrition Examination Survey (NHANES) conducted between 2007 and 2014, the study employed chi-square tests of independence and t-tests to analyze differences between the NAFLD and control groups, while logistic regression analysis was used to identify factors influencing NAFLD risk and assess the association of plant-based dietary retinol intake with such risk. The NAFLD group consisted of 1,286 males (53.5%) and 1,138 females (46.9%), and logistic regression analysis identified uric acid (UA), high-density lipoprotein (HDL), smoking, vigorous recreational activity, hypertension, diabetes, gender, BMI, race, annual household income, and plant-based retinol intake as significant predictors of NAFLD (P < 0.05), with notably higher dietary intake of plant-based retinol being associated with a lower risk of NAFLD (OR = 0.670, 95% CI: 0.532-0.842). This study demonstrates that specific dietary components, especially plant-based retinol, play an important role in influencing NAFLD risk among American adults, and further long-term research is needed to inform public health initiatives aimed at reducing NAFLD prevalence.
| Published in | World Journal of Public Health (Volume 10, Issue 3) |
| DOI | 10.11648/j.wjph.20251003.29 |
| Page(s) | 379-388 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
NAFLD, Dietary Factor, Plant-based Retinol, Logistic Regression Model, NHANES
Group | NAFLD (total)a | p-valueb | |
|---|---|---|---|
no | yes | ||
Gender (n, %) | <0.001 | ||
Male | 1781 (42.52%) | 1286 (53.05%) | |
Female | 2408 (57.48%) | 1138 (46.95%) | |
Age Group (n, %) | <0.001 | ||
20-44 years | 1890 (45.12%) | 709 (29.25%) | |
45-59 years | 988 (23.59%) | 655 (27.02%) | |
60-74 years | 862 (20.58%) | 742 (30.61%) | |
≥75 years | 449 (10.72%) | 318 (13.12%) | |
Race/Ethnicity (n, %) | <0.001 | ||
Mexican American | 488 (11.65%) | 552 (22.77%) | |
Other Hispanic | 444 (10.60%) | 294 (12.13%) | |
Non-Hispanic White | 1845 (44.04%) | 1155 (47.65%) | |
Non-Hispanic Black | 931 (22.22%) | 269 (11.10%) | |
Other/Multiracial | 481 (11.48%) | 154 (6.35%) | |
BMI (n, %) | <0.001 | ||
<25 kg/m2 | 1716 (41.02%) | 108 (4.46%) | |
25 to <30 kg/m2 | 1568 (37.49%) | 637 (26.32%) | |
≥30 kg/m2 | 899 (21.49%) | 1675 (69.21%) | |
Educational Level (n, %) | <0.001 | ||
< High school | 902 (21.55%) | 802 (33.14%) | |
High school | 954 (22.80%) | 543 (22.44%) | |
> High school | 2329 (55.65%) | 1075 (44.42%) | |
Annual household income (n, %) | <0.001 | ||
<$20,000 | 780 (19.45%) | 561 (24.14%) | |
$20,000-$44,999 | 1352 (33.71%) | 931 (40.06%) | |
$45,000-$74,999 | 781 (19.47%) | 409 (17.60%) | |
≥$75,000 | 1098 (27.37%) | 423 (18.20%) | |
Smoking status (n, %) | <0.001 | ||
Yes | 1576 (37.64%) | 1131 (46.66%) | |
No | 2611 (62.36%) | 1293 (53.34%) | |
Vigorous recreational activity (n, %) | <0.001 | ||
Yes | 1031 (24.61%) | 270 (11.14%) | |
No | 3158 (75.39%) | 2154 (88.86%) | |
Hypertension (n, %) | <0.001 | ||
Yes | 1648 (39.34%) | 1539 (63.49%) | |
No | 2541 (60.66%) | 885 (36.51%) | |
Diabetes (n, %) | <0.001 | ||
Yes | 505 (12.06%) | 910 (37.54%) | |
No | 3684 (87.94%) | 1514 (62.46%) | |
Cholesterol: mean (SD), mg/dL | 192.16 (41.19) | 194.23 (41.79) | 0.051 |
Uric Acid: mean (SD), mg/dL | 5.14 (1.30) | 6.03 (1.43) | <0.001 |
HDL: mean (SD), mg/dL c | 56.28 (14.86) | 45.78 (11.87) | <0.001 |
LDL: mean (SD), mg/dL d | 114.86 (35.13) | 115.34 (35.95) | 0.605 |
Average energy intake: mean (SD), kcal/day | 1903.27 (695.88) | 1912.03 (711.51) | 0.625 |
Total dietary retinol intake: mean (SD), μg/1000kcal/day | 338.66 (284.09) | 325.69 (279.77) | 0.072 |
Animal-derived dietary retinol intake: mean (SD), μg/1000kcal/day) | 122.70 (150.62) | 134.97 (205.69) | 0.005 |
Plant-based dietary retinol intake: mean (SD), μg/1000kcal/day) | 198.80 (238.80) | 171.24 (181.11) | <0.001 |
Variable | B | SE | Wald χ2 | P | OR (95%CI) |
|---|---|---|---|---|---|
Gender | 0.517 | 0.077 | 47.144 | <0.001 | 1.694 (1.139,1.374) |
BMI | 1.587 | 0.053 | 902.079 | <0.001 | 4.891 (4.410,5.425) |
Race/Ethnicity | -0.498 | 0.032 | 239.729 | <0.001 | 0.608 (0.571,0.647) |
Annual household income | -0.097 | 0.033 | 8.662 | 0.003 | 0.908 (0.851,0.968) |
Smoking | 0.266 | 0.070 | 14.481 | <0.001 | 1.305 (1.138,1.497) |
Vigorous recreational activity | -0.512 | 0.098 | 27.334 | 0.001 | 0.599 (0.495,0.726) |
Hypertension | 0.426 | 0.077 | 30.652 | <0.001 | 1.531 (1.316,1.779) |
Diabetes | 0.974 | 0.083 | 136.784 | <0.001 | 2.648 (2.250,3.118) |
Uric Acid | 0.308 | 0.028 | 122.992 | <0.001 | 1.360 (1.288,1.436) |
HDL | -0.043 | 0.003 | 197.819 | <0.001 | 0.958 (0.952,0.963) |
Plant-based dietary retinol intake | -0.121 | 0.023 | 28.106 | <0.001 | 0.886 (0.847,0.926) |
Variables | Model1a | Mode2b | Mode3c | |||
|---|---|---|---|---|---|---|
OR (95%CI) | P value | OR (95%CI) | P value | OR (95%CI) | P value | |
Plant-based dietary retinol intake (RAEs, μg/1000kcal/day) | ||||||
<70.37 | 1.00 (ref.) | 1.00 (ref.) | 1.00 (ref.) | |||
70.37 to <138.53 | 0.949 (0.781-1.152) | 0.589 | 0.943 (0.766-1.160) | 0.574 | 1.015 (0.820-1.258) | 0.886 |
138.53 to <253.07 | 0.855 (0.704-1.038) | 0.111 | 0.821 (0.668-1.010) | 0.062 | 0.899 (0.710-1.138) | 0.367 |
≥253.07 | 0.637 (0.515-0.788) | <0.001 | 0.588 (0.465-0.745) | <0.001 | 0.670 (0.532-0.842) | 0.001 |
NAFLD | Nonalcoholic Fatty Liver Disease |
NHANES | National Health and Nutrition Examination Survey |
HDL | High-density Lipoprotein |
UA | Uric Acid |
BMI | Body Mass Index |
NASH | Nonalcoholic Steatohepatitis |
HCC | Hepatocellular Carcinoma |
USFLI | United States Fatty Liver Index |
RAE | Retinol Activity Equivalents |
LDL | Low-density Lipoprotein |
TC | Total Cholesterol |
SD | Standard Deviation |
ORs | Odds Ratios |
CIs | Confidence Intervals |
hs-CRP | High-sensitivity C-reactive Protein |
NF-κB | Nuclear Factor-kappa B |
PUFAs | Polyunsaturated Fatty Acids |
| [1] | Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002; 346: 1221-31. |
| [2] | Vadarlis A, Antza C, Bakaloudi DR, Doundoulakis I, Kalopitas G, Samara M, Dardavessis T, Maris T, Chourdakis M. Systematic review with meta-analysis: The effect of vitamin E supplementation in adult patients with non-alcoholic fatty liver disease. J Gastroenterol Hepatol. 2021; 36: 311-9. |
| [3] | Afzali N, Ebadi SS, Afzali H, Sharif MR, Vazirian M, Ebadi SA, Shahkarami V, Rahimi H. Effect of beta vulgaris extract on liver enzymes in patients with non-alcoholic fatty liver disease: A randomized clinical trial. Hepat Mon. 2020; 20: e102125. |
| [4] | Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018; 15: 11-20. |
| [5] | Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology. 2018; 67: 123-33. |
| [6] | Lotfi A, Saneei P, Hekmatdost A, Salehisahlabadi A, Shiranian A, Ghiasvand R. The relationship between dietary antioxidant intake and physical activity rate with nonalcoholic fatty liver disease (NAFLD): A case - Control study. Clin Nutr ESPEN. 2019; 34: 45-9. |
| [7] | Le MH, Devaki P, Ha NB, Jun DW, Te HS, Cheung RC, Nguyen MH. Prevalence of non-alcoholic fatty liver disease and risk factors for advanced fibrosis and mortality in the United States. PLoS One. 2017; 12: e0173499. |
| [8] | Li H, Gu Y, Wu X, Rayamajhi S, Bian S, Zhang Q, Meng G, Liu L, Wu H, Zhang S, et al. Association between consumption of edible seaweeds and newly diagnosed non-alcohol fatty liver disease: The TCLSIH Cohort Study. Liver Int. 2021; 41: 311-20. |
| [9] | Younossi ZM, Henry L. The impact of obesity and type 2 diabetes on chronic liver disease. Am J Gastroenterol. 2019; 114: 1714-5. |
| [10] | Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J Hepatol. 2016; 65: 589-600. |
| [11] | Vahid F, Hekmatdoost A, Mirmajidi S, Doaei S, Rahmani D, Faghfoori Z. Association between index of nutritional quality and nonalcoholic fatty liver disease: The role of vitamin D and B group. Am J Med Sci. 2019; 358: 212-8. |
| [12] | Aktary ML, Eller LK, Nicolucci AC, Reimer RA. Cross-sectional analysis of the health profile and dietary intake of a sample of Canadian adults diagnosed with non-alcoholic fatty liver disease. Food Nutr Res. 2020; 64: 4548. |
| [13] | Mollard RC, Sénéchal M, MacIntosh AC, Hay J, Wicklow BA, Wittmeier KD, Sellers EA, Dean HJ, Ryner L, Berard L, McGavock JM. Dietary determinants of hepatic steatosis and visceral adiposity in overweight and obese youth at risk of type 2 diabetes. Am J Clin Nutr. 2014; 99: 804-12. |
| [14] | Ouyang X, Cirillo P, Sautin Y, McCall S, Bruchette JL, Diehl AM, Johnson RJ, Abdelmalek MF. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J Hepatol. 2008; 48: 993-9. |
| [15] | Shim P, Choi D, Park Y. Association of blood fatty acid composition and dietary pattern with the risk of non-alcoholic fatty liver disease in patients who underwent cholecystectomy. Ann Nutr Metab. 2017; 70: 303-11. |
| [16] | Dorosti M, Jafary Heidarloo A, Bakhshimoghaddam F, Alizadeh M. Whole-grain consumption and its effects on hepatic steatosis and liver enzymes in patients with non-alcoholic fatty liver disease: a randomised controlled clinical trial. Br J Nutr. 2020; 123: 328-36. |
| [17] | Koutnikova H, Genser B, Monteiro-Sepulveda M, Faurie JM, Rizkalla S, Schrezenmeir J, Clément K. Impact of bacterial probiotics on obesity, diabetes and non-alcoholic fatty liver disease related variables: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2019; 9: e017995. |
| [18] | Maleki Z, Jazayeri S, Eslami O, Shidfar F, Hosseini AF, Agah S, Norouzi H. Effect of soy milk consumption on glycemic status, blood pressure, fibrinogen and malondialdehyde in patients with non-alcoholic fatty liver disease: a randomized controlled trial. Complement Ther Med. 2019; 44: 44-50. |
| [19] | Al-Busafi SA, Bhat M, Wong P, Ghali P, Deschenes M. Antioxidant therapy in nonalcoholic steatohepatitis. Hepat Res Treat. 2012; 2012: 947575. |
| [20] | Chen G. The link between hepatic vitamin a metabolism and nonalcoholic fatty liver disease. Curr Drug Targets. 2015; 16: 1281-92. |
| [21] | Lim HS, Choi J, Lee B, Kim SG, Kim YS, Yoo JJ. Association between inflammatory biomarkers and nutritional status in fatty liver. Clin Nutr Res. 2020; 9: 182-94. |
| [22] | Choi WJ, Ford ES, Curhan G, Rankin JI, Choi HK. Independent association of serum retinol and beta-carotene levels with hyperuricemia: A national population study. Arthritis Care Res. 2012; 64: 389-96. |
| [23] | Ruhl CE, Everhart JE. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment Pharmacol Ther. 2015; 41: 65-76. |
| [24] | Kim D, Kim W, Adejumo AC, Cholankeril G, Tighe SP, Wong RJ, Gonzalez SA, Harrison SA, Younossi ZM, Ahmed A. Race/ethnicity-based temporal changes in prevalence of NAFLD-related advanced fibrosis in the United States, 2005-2016. Hepatol Int. 2019; 13: 205-13. |
| [25] | Kim D, Yoo ER, Li AA, Tighe SP, Cholankeril G, Harrison SA, Ahmed A. Depression is associated with non-alcoholic fatty liver disease among adults in the United States. Aliment Pharmacol Ther. 2019; 50: 590-8. |
| [26] | Meffert PJ, Baumeister SE, Lerch MM, Mayerle J, Kratzer W, Völzke H. Development, external validation, and comparative assessment of a new diagnostic score for hepatic steatosis. Am J Gastroenterol. 2014, 109: 1404-14. |
| [27] | Zhang P, Sun J, Guo Y, Han M, Yang F, Sun Y. Association between retinol intake and hyperuricaemia in adults. Public Health Nutr. 2021; 24: 2205-14. |
| [28] | Sun Y, Sun J, Wang J, Gao T, Zhang H, Ma A. Association between vitamin C intake and risk of hyperuricemia in US adults. Asia Pac J Clin Nutr. 2018; 27: 1271-6. |
| [29] | Feskanich D, Rimm EB, Giovannucci EL, Colditz GA, Stampfer MJ, Litin LB, Willett WC. Reproducibility and validity of food intake measurements from a semiquantitative food frequency questionnaire. J Am Diet Assoc. 1993; 93: 790-6. |
| [30] | Hu FB, Rimm E, Smith-Warner SA, Feskanich D, Stampfer MJ, Ascherio A, Sampson L, Willett WC. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am J Clin Nutr. 1999; 69: 243-9. |
| [31] | Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA. 2015; 314: 1021-9. |
| [32] | Whelton PK, Carey RM, Aronow WS, Casey DE, Jr., Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension. 2018; 71: e13-e115. |
| [33] | Zeng J, Zhang J, Li Z, Li T, Li G. Prediction model of artificial neural network for the risk of hyperuricemia incorporating dietary risk factors in a Chinese adult study. Food & nutrition research. 2020; 64. |
| [34] | Christensen K, Lawler T, Mares J. Dietary carotenoids and non-alcoholic fatty liver disease among US adults, NHANES 2003-2014. Nutrients. 2019; 11: 1101. |
| [35] | Yoneda M, Mawatari H, Fujita K, Iida H, Yonemitsu K, Kato S, Takahashi H, Kirikoshi H, Inamori M, Nozaki Y, et al. High-sensitivity C-reactive protein is an independent clinical feature of nonalcoholic steatohepatitis (NASH) and also of the severity of fibrosis in NASH. J Gastroenterol. 2007; 42: 573-82. |
| [36] | Abe RAM, Masroor A, Khorochkov A, Prieto J, Singh KB, Nnadozie MC, Abdal M, Shrestha N, Mohammed L. The role of vitamins in non-Alcoholic fatty liver disease: A systematic review. Cureus. 2021; 13: e16855. |
| [37] | Iwaki M, Matsuda M, Maeda N, Funahashi T, Matsuzawa Y, Makishima M, Shimomura I. Induction of adiponectin, a fat-derived antidiabetic and antiatherogenic factor, by nuclear receptors. Diabetes. 2003; 52: 1655-63. |
| [38] | Cimini FA, Barchetta I, Carotti S, Bertoccini L, Baroni MG, Vespasiani-Gentilucci U, Cavallo MG, Morini S. Relationship between adipose tissue dysfunction, vitamin D deficiency and the pathogenesis of non-alcoholic fatty liver disease. World J Gastroenterol. 2017; 23: 3407-17. |
| [39] | Ma C, Liu Y, He S, Zeng J, Li P, Ma C, Ping F, Zhang H, Xu L, Li W, Li Y. Negative association between antioxidant vitamin intake and non-alcoholic fatty liver disease in Chinese non-diabetic adults: mediation models involving superoxide dismutase. Free Radic Res. 2020; 54: 670-7. |
| [40] | Duseja A, Chalasani N. Epidemiology and risk factors of nonalcoholic fatty liver disease (NAFLD). Hepatol Int. 2013; 7 Suppl 2: 755-64. |
| [41] | Musso G, Gambino R, De Michieli F, Cassader M, Rizzetto M, Durazzo M, Fagà E, Silli B, Pagano G. Dietary habits and their relations to insulin resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology. 2003; 37: 909-16. |
| [42] | Marchesini G, Bugianesi E, Forlani G, Cerrelli F, Lenzi M, Manini R, Natale S, Vanni E, Villanova N, Melchionda N, Rizzetto M. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology. 2003; 37: 917-23. |
| [43] | Zelber-Sagi S, Nitzan-Kaluski D, Goldsmith R, Webb M, Blendis L, Halpern Z, Oren R. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): a population based study. J Hepatol. 2007; 47: 711-7. |
| [44] | Sathiaraj E, Chutke M, Reddy MY, Pratap N, Rao PN, Reddy DN, Raghunath M. A case-control study on nutritional risk factors in non-alcoholic fatty liver disease in Indian population. Eur J Clin Nutr. 2011; 65: 533-7. |
| [45] | Fan JG, Cao HX. Role of diet and nutritional management in non-alcoholic fatty liver disease. J Gastroenterol Hepatol. 2013; 28 Suppl 4: 81-7. |
| [46] | Asrih M, Jornayvaz FR. Diets and nonalcoholic fatty liver disease: the good and the bad. Clin Nutr. 2014; 33: 186-90. |
| [47] | Fan JG, Li F, Cai XB, Peng YD, Ao QH, Gao Y. Effects of nonalcoholic fatty liver disease on the development of metabolic disorders. J Gastroenterol Hepatol. 2007; 22: 1086-91. |
| [48] | Jung HS, Chang Y, Kwon MJ, Sung E, Yun KE, Cho YK, Shin H, Ryu S. Smoking and the risk of non-alcoholic fatty liver disease: A cohort study. Am J Gastroenterol. 2019; 114: 453-63. |
| [49] | Jia WP. The impact of cigarette smoking on metabolic syndrome. Biomed Environ Sci. 2013; 26: 947-52. |
APA Style
Liu, C., Bai, Z., Cheng, J. (2025). Plant-Based Retinol Intake and Risk of Nonalcoholic Fatty Liver Disease in American Adults: Insights from NHANES 2007-2014. World Journal of Public Health, 10(3), 379-388. https://doi.org/10.11648/j.wjph.20251003.29
ACS Style
Liu, C.; Bai, Z.; Cheng, J. Plant-Based Retinol Intake and Risk of Nonalcoholic Fatty Liver Disease in American Adults: Insights from NHANES 2007-2014. World J. Public Health 2025, 10(3), 379-388. doi: 10.11648/j.wjph.20251003.29
@article{10.11648/j.wjph.20251003.29,
author = {Can Liu and Zeming Bai and Jingmin Cheng},
title = {Plant-Based Retinol Intake and Risk of Nonalcoholic Fatty Liver Disease in American Adults: Insights from NHANES 2007-2014
},
journal = {World Journal of Public Health},
volume = {10},
number = {3},
pages = {379-388},
doi = {10.11648/j.wjph.20251003.29},
url = {https://doi.org/10.11648/j.wjph.20251003.29},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251003.29},
abstract = {Existing evidence suggests a strong correlation between nonalcoholic fatty liver disease (NAFLD) risk and dietary factors, and this investigation aimed to examine the association between dietary factors and NAFLD risk in American adults. Utilizing data from the National Health and Nutrition Examination Survey (NHANES) conducted between 2007 and 2014, the study employed chi-square tests of independence and t-tests to analyze differences between the NAFLD and control groups, while logistic regression analysis was used to identify factors influencing NAFLD risk and assess the association of plant-based dietary retinol intake with such risk. The NAFLD group consisted of 1,286 males (53.5%) and 1,138 females (46.9%), and logistic regression analysis identified uric acid (UA), high-density lipoprotein (HDL), smoking, vigorous recreational activity, hypertension, diabetes, gender, BMI, race, annual household income, and plant-based retinol intake as significant predictors of NAFLD (P < 0.05), with notably higher dietary intake of plant-based retinol being associated with a lower risk of NAFLD (OR = 0.670, 95% CI: 0.532-0.842). This study demonstrates that specific dietary components, especially plant-based retinol, play an important role in influencing NAFLD risk among American adults, and further long-term research is needed to inform public health initiatives aimed at reducing NAFLD prevalence.
},
year = {2025}
}
TY - JOUR T1 - Plant-Based Retinol Intake and Risk of Nonalcoholic Fatty Liver Disease in American Adults: Insights from NHANES 2007-2014 AU - Can Liu AU - Zeming Bai AU - Jingmin Cheng Y1 - 2025/09/05 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251003.29 DO - 10.11648/j.wjph.20251003.29 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 379 EP - 388 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251003.29 AB - Existing evidence suggests a strong correlation between nonalcoholic fatty liver disease (NAFLD) risk and dietary factors, and this investigation aimed to examine the association between dietary factors and NAFLD risk in American adults. Utilizing data from the National Health and Nutrition Examination Survey (NHANES) conducted between 2007 and 2014, the study employed chi-square tests of independence and t-tests to analyze differences between the NAFLD and control groups, while logistic regression analysis was used to identify factors influencing NAFLD risk and assess the association of plant-based dietary retinol intake with such risk. The NAFLD group consisted of 1,286 males (53.5%) and 1,138 females (46.9%), and logistic regression analysis identified uric acid (UA), high-density lipoprotein (HDL), smoking, vigorous recreational activity, hypertension, diabetes, gender, BMI, race, annual household income, and plant-based retinol intake as significant predictors of NAFLD (P < 0.05), with notably higher dietary intake of plant-based retinol being associated with a lower risk of NAFLD (OR = 0.670, 95% CI: 0.532-0.842). This study demonstrates that specific dietary components, especially plant-based retinol, play an important role in influencing NAFLD risk among American adults, and further long-term research is needed to inform public health initiatives aimed at reducing NAFLD prevalence. VL - 10 IS - 3 ER -
School of Management, Shanxi Medical University, Taiyuan, China; School of Public Health, Shanxi Medical University, Taiyuan, China
School of Medicine and Food Engineering, Shanxi University of Chinese Medicine, Jinzhong, China
School of Management, Shanxi Medical University, Taiyuan, China
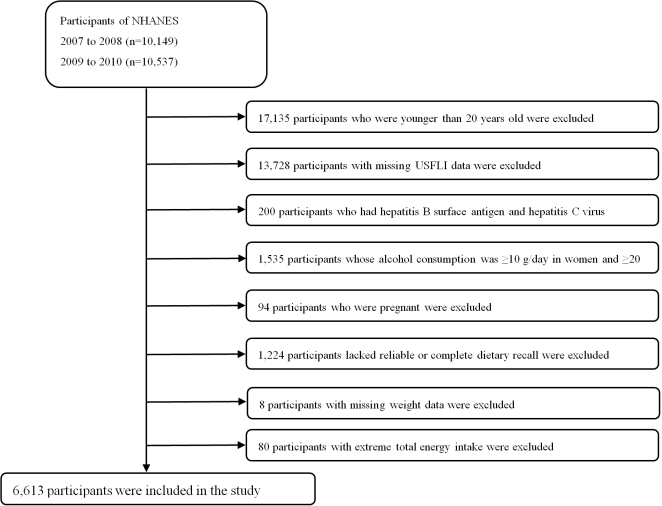
Figure 1. Flowchart of individual selection.
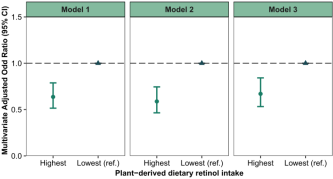
Figure 2. Association between plant-based dietary retinol intake and NAFLD risk. Hazard ratios and 95% confidence intervals (error bars) were calculated using covariate-adjusted method. Covariates were as follows: gender, age, race, education level, smoking status, physical activity, income level, BMI, hypertension, diabetes, TC and UA.
Information

