Abstract
Malaria remains a major public health burden in Mali, requiring control strategies adapted to local epidemiological contexts. This study compared the evolution of malaria prevalence and determinants in the health districts of Kati (peri-urban/agricultural area) and Markala (agricultural/hydro-agricultural area). This was a cross-sectional, comparative study of malaria data from the districts of Kati and Markala from January 2018 to December 2022. The data were extracted from the District Health Information Software 2. The comparative statistical analysis used Chi-square tests and logistic regressions to identify the factors associated (age, sex, seasonality) with the observed variations. A total of 422,020 Cases of malaria were recorded in both districts. The Markala district had a higher average annual prevalence than Kati (6.038% vs 6.024%, p=0.001), although annual trends showed significant variability, notably a more pronounced increase in Kati in 2021. Seasonal analysis confirmed the epidemic peak during the high transmission period (July-October) in both districts, but the malaria burden in Markala appeared to be more chronic and less strictly seasonal, potentially linked to agricultural irrigation. This study revealed an epidemiological shift in Mali, with marked heterogeneity between peri-urban and hydro-agricultural areas. The increased prevalence in Kati in 2022 and the shift in disease burden towards those over 5 years of age, particularly women, necessitate adapting national strategies. Environmental management of rice cultivation, targeting of adults, and improved quality of routine data are crucial for precision vector control.
|
Published in
|
World Journal of Public Health (Volume 11, Issue 2)
|
|
DOI
|
10.11648/j.wjph.20261102.16
|
|
Page(s)
|
146-154 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Malaria, Epidemiology, Markala, Kati, Mali
1. Introduction
Although the biological mechanism of malaria (caused by the
Plasmodium parasite and transmitted by the Anopheles mosquito) has been documented for over a century, this disease remains one of the most devastating worldwide. Sub-Saharan Africa continues to bear the brunt of the outbreak, a situation that has become considerably more complex by 2025
| [1] | World Health Organization, “World Malaria Report 2025”, WHO, Geneva, Summary, Dec. 2025. |
| [2] | African Union, ALMA, and RBM Partnership to End Malaria, “African Union Malaria Progress Report 2025”, 39th AU Summit, Addis Ababa, Feb. 2026. |
[1, 2]
.
Indeed, the region now records approximately 263 million cases annually. This resurgence is explained by a critical convergence of factors: climate change which alters transmission areas, the emergence of resistance to insecticides and treatments, as well as chronic underfunding of control programs
| [1] | World Health Organization, “World Malaria Report 2025”, WHO, Geneva, Summary, Dec. 2025. |
| [2] | African Union, ALMA, and RBM Partnership to End Malaria, “African Union Malaria Progress Report 2025”, 39th AU Summit, Addis Ababa, Feb. 2026. |
[1, 2]
.
Analysis of WHO data for 2024 reveals Mali's particular vulnerability to malaria
| [3] | World Health Organization, “2024 Global Malaria Report”, WHO, Geneva, 2024. |
[3]
. With 8.15 million cases and over 14,000 deaths, the country contributes significantly to global morbidity. Among the eight nations that experienced a major resurgence (+1.4 million cases over four years), Mali exemplifies the health crisis affecting sub-Saharan Africa, the region where 95% of mortality related to the parasite occurs
| [3] | World Health Organization, “2024 Global Malaria Report”, WHO, Geneva, 2024. |
| [4] | Directorate General of Health and Public Hygiene of the Ministry of Health of Mali, “Directory of the local health information system of Mali 2022”. Bamako, 2022. |
[3, 4]
.
Despite the implementation of key strategies, including seasonal malaria chemoprevention (SMC) and the mass distribution of long-lasting insecticidal nets (LLINs)
| [5] | National Institute of Statistics (INSTAT), Bamako, Mali, National Malaria Control Program (PNLP), Bamako, Mali, and The DHS Program (ICF), Rockville, Maryland, USA, “Survey Report on Malaria Indicators in Mali 2021”, INSTAT, Bamako, 2022. |
| [6] | Global Malaria Community and Medicines for Malaria Venture (MMV), “Malaria in Mali: Statistics | Severe Malaria Observatory”, SEVERE MALARIA OBSERVATORY (SMO). Accessed: 22 February 2026. [Online]. Available at:
https://www.severemalaria.org/fr/pays/mali |
[5, 6]
, the path to elimination remains fraught with challenges
| [5] | National Institute of Statistics (INSTAT), Bamako, Mali, National Malaria Control Program (PNLP), Bamako, Mali, and The DHS Program (ICF), Rockville, Maryland, USA, “Survey Report on Malaria Indicators in Mali 2021”, INSTAT, Bamako, 2022. |
| [6] | Global Malaria Community and Medicines for Malaria Venture (MMV), “Malaria in Mali: Statistics | Severe Malaria Observatory”, SEVERE MALARIA OBSERVATORY (SMO). Accessed: 22 February 2026. [Online]. Available at:
https://www.severemalaria.org/fr/pays/mali |
[5, 6]
. The persistence of pockets of high transmission and the emergence of resistance to insecticides and antimalarial drugs threaten the progress made over the last decade. Its prevalence varies considerably across areas, depending on epidemiological, ecological, and socioeconomic factors. Malaria stratification in Mali has classified areas based on incidence adjusted for population size. Transmission zones range from hyperendemic (south, prevalence > 50%) to hypoendemic (urban areas such as Bamako, prevalence < 10%)
| [5] | National Institute of Statistics (INSTAT), Bamako, Mali, National Malaria Control Program (PNLP), Bamako, Mali, and The DHS Program (ICF), Rockville, Maryland, USA, “Survey Report on Malaria Indicators in Mali 2021”, INSTAT, Bamako, 2022. |
[5]
.
The effectiveness of national malaria control programs (NMCPs) relies on the ability to adapt interventions to local epidemiological realities, a concept known as epidemiological stratification
| [7] | Kouyaté, M., Keïta, M., Sidibé, A., & Traoré, M. (2021)., “Study of the prevalence of malaria in rural and urban districts”. Journal of Malian Health Studies, 15(3), 142-157.
https://doi.org/10.3389/fmala.2025.1596496 |
[7]
. In Mali, geographical heterogeneity is exacerbated by anthropogenic and environmental factors. Districts cannot be treated uniformly
| [7] | Kouyaté, M., Keïta, M., Sidibé, A., & Traoré, M. (2021)., “Study of the prevalence of malaria in rural and urban districts”. Journal of Malian Health Studies, 15(3), 142-157.
https://doi.org/10.3389/fmala.2025.1596496 |
[7]
. In particular, areas benefiting from hydro-agricultural projects, such as irrigated perimeters, are suspected of acting as permanent or prolonged transmission hotspots, providing long-term larval habitats for vectors
| [7] | Kouyaté, M., Keïta, M., Sidibé, A., & Traoré, M. (2021)., “Study of the prevalence of malaria in rural and urban districts”. Journal of Malian Health Studies, 15(3), 142-157.
https://doi.org/10.3389/fmala.2025.1596496 |
| [8] | M. Kamissoko, “The prevalence of malaria during pregnancy in the Bamako district,” University of Sciences, Techniques and Technologies of Bamako (USTTB)/Faculty of Medicine and Odonto-Stomatology (FMOS), Bamako, Mali, 2015. Accessed: February 22, 2026. [Online]. Available from:
https://www.bibliosante.ml/handle/123456789/973 |
[7, 8]
. In Mali, previous work has often focused on the effectiveness of LLINs and SPC in children, leaving an analytical gap regarding variations in incidence among adolescents and adults in areas of altered transmission. This study seeks to fill this gap by using a long-term comparative approach (2018-2022) based on routine data, thus providing an essential epidemiological and programmatic perspective. The overall objective was to conduct a comparative study of malaria prevalence in the health districts of Kati and Markala.
2. Materials and Methods
2.1. Type and Period of Study
This was a cross-sectional, comparative, analytical study of malaria data covering the period from 2018 to 2022.
2.2. Places of Study
The study was conducted in the health districts of Kati and Markala in the Koulikoro region, chosen for their contrasting socio-ecological profiles: Kati: a strongly peri-urban area, influenced by its proximity to the capital, Bamako. Agricultural activity is present but less intense, with transmission expected to follow a more strictly seasonal pattern. Markala: a district dominated by the Markala Dam and its vast irrigated rice paddies. This hydro-agricultural environment is known to maintain humidity conditions favorable to Anopheles mosquitoes over long periods, potentially beyond the typical rainy season.
2.3. Study Population and Sampling
The study included all suspected and confirmed cases of malaria seen in consultation and reported in the District Health Information Software 2 (DHIS2) database from 2018 to 2022. An exhaustive sampling was conducted using all available data in the database. Inclusion criteria included all suspected and confirmed cases of malaria reported in the two health districts during the study period.
2.4. Operational Definitions and Variables
Prevalence: the ratio of the total annual number of confirmed malaria cases to the total annual population during the period. Prevalence, RDTs (rapid diagnostic tests), smear tests, periods (trimes (T): T1, T2, T3, T4), sex, and age were studied. Age was categorized into two age groups: under 5 years and 5 years and over.
2.5. Data Collection and Analysis
Data were extracted from DHIS2 and then processed using Microsoft Excel® 2016. Analysis was performed with R Studio and StatsTester. Descriptive analysis involved using frequency and proportion tables for categorical variables, expressed as percentages. Etiological analysis focused on the Z-test, which was applied using StatsTester to compare proportions at a significance level of p-value 0.05.
2.6. Ethical and Professional Considerations
The research protocol was validated by the health authorities of the relevant health districts before the use of DHIS2. The data used did not contain any personally identifiable information. The analysis and dissemination of the results complied with medical ethics and professional standards.
2.6.1. Ethical Approval
The study was approved by the Technical Committee of the Faculty of Medicine and Odonto -Stomatology of Bamako at the University of Sciences, Techniques and Bamako Technologies (FMOS/USTTB). Authorization was obtained from the health authorities of the health district of commune I and the CSCOM-U of Banconi before the start of the study.
2.6.2. Consent to Participate
Not applicable. Verbal informed consent was obtained from individual participants included in the study after they had read the study information sheet, which specified the objectives and procedures of the study, the subsequent use of the data, and the entirely voluntary nature of participation. The data were collected anonymously, so that the identity of the study participants could not be identified or identified within the meaning of the applicable law relating to the protection of natural persons with regard to the processing of personal data.
3. Results
3.1. Overall Malaria Burden and Sociodemographic Data
Between 2018 and 2022, a total of 256,969 suspected cases of malaria were reported in the Kati district and 165,051 suspected cases in the Markala district. Of a total of 358,253 confirmed cases of malaria, 237,224 cases (66.2%) were recorded in Kati and 121,029 (33.7%) in Markala. Patients aged 5 years and older constituted the majority of confirmed cases in both districts, representing 70.2% of those affected by malaria. This proportion varied annually between 68% and 74% in the Kati health district and between 69% and 72% in the Markala district. Females were predominant among confirmed cases, representing 54.6% of all confirmed cases in the 5-year-old age group. Among children under 5, males were more affected, accounting for 53.8% of cases (53.2% in Kati and 55.0% in Markala). Among children 5 and over, females were more affected, accounting for 54.6% of cases (54.9% in Kati and 54.1% in Markala).
Table 1. Distribution of confirmed malaria cases by age group, year, sex, and health district.
Age range (in years) | Districts | Total (%) |
Kati (%) | Markala (%) |
< 5 | | 72,928 (28.4) | 52,898 (32.0) | 125,826 (29.8) |
5 | | 184,041 (71.6) | 112,153 (68.0) | 296,194 (70.2) |
Total | | 256,969 (60.9) | 165,051 (39.1) | 422,020 (100.0) |
Year | Sex | Kati (%) | Markala (%) | Total (%) |
2018 | Male | 20,434 (43.5) | 13,897 (40.5) | 34,331 (8.1) |
| Female | 19,639 (56.5) | 15,135 (59.5) | 34,774 (11.2) |
2019 | Male | 17,642 (38.1) | 11,780 (40.0) | 29,422 (6.6) |
| Female | 19,069 (61.9) | 11,726 (60.0) | 30,795 (10.2) |
2020 | Male | 19,973 (38.4) | 12,851 (39.2) | 32,824 (7.4) |
| Female | 22,126 (61.6) | 13,805 (60.8) | 235,931 (11.8) |
2021 | Male | 24,122 (28.5) | 10,894 (31.1) | 35,016 (6.2) |
| Female | 28,426 (71.5) | 11,315 (68.9) | 39,741 (14.7) |
2022 | Male | 30,033 (22.0) | 9535 (24.1) | 39,568 (5.5) |
| Female | 35,760 (78.0) | 10,091 (75.9) | 45,851 (18.4) |
Total | | 237,224 (66.2) | 121,029 (33.7) | 358,253 (100.0) |
3.2. Comparison of Annual Prevalence Rates
The annual prevalence of malaria was statistically higher in the Markala health district than in the Kati health district in 2018 (8.72% vs 5.97%; p=0.001), in 2019 (6.87% vs 5.31%; p=0.001) and in 2020 (6.06% vs 5.14%; p=0.001) while the Kati health district was statistically higher than the Markala health district in 2021 (5.90% vs 4.61%; p=0.001) and in 2022 (7.80% vs 3.93%; p=0.001).
Table 2. Comparison of the annual prevalence of malaria in the health districts of Kati and Markala from 2018 to 2022.
Year | Districts | p -value |
Kati (%) | Markala (%) |
2018 | 5.97 | 8.72 | 0.001 |
2019 | 5.31 | 6.87 | 0.001 |
2020 | 5.14 | 6.06 | 0.001 |
2021 | 5.90 | 4.61 | 0.001 |
2022 | 7.80 | 3.93 | 0.001 |
3.3. Comparison of Prevalence in Relation to Diagnostic Methods for Malaria
A comparison of annual malaria prevalence rates using rapid diagnostic tests (RDTs) and general epidemiology (GE) in the Kati and Markala health districts revealed a significant difference between the two districts (p = 0.001). GE completion rates were higher in Kati (24.14% in 2018 and 30.03% in 2022) than in Markala (4.35% in 2018 and 6.8% in 2022), with a significant difference (p = 0.001). There was also a significant difference in RDT completion rates between the two health districts between 2018 and 2021 (p = 0.001). However, in 2022, the RDT completion rate in Markala was not significantly different from that in Kati.
Table 3. Comparison of annual malaria prevalence through two diagnostic tests in the health districts of Kati and Markala.
Year | GE | TDR |
Kati (%) | Markala (%) | p -value | Kati (%) | Markala (%) | p -value |
2018 | 24.14 | 4.35 | 0.001 | 51.71 | 60.28 | 0.001 |
2019 | 28.43 | 3.28 | 0.001 | 56.22 | 54.05 | 0.001 |
2020 | 28.29 | 9.58 | 0.001 | 58.35 | 43.23 | 0.001 |
2021 | 27.53 | 8.24 | 0.001 | 62.95 | 53.44 | 0.001 |
2022 | 30.03 | 6.80 | 0.001 | 58.88 | 58.93 | 0.90 |
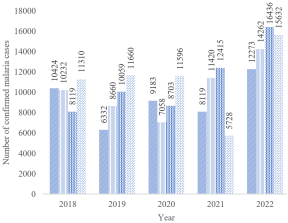
3.4. Comparison of Annual Confirmed Malaria Cases per Quarter in the Kati Health District
THE number of confirmed cases of malaria In the Kati district, a sharp increase (epidemic peak) was observed during the third and fourth quarters throughout the study period, except for 2021 for the fourth quarter and 2018 for the third quarter. Furthermore, malaria has become more chronic and less strictly seasonal.
Figure 1. Number of confirmed malaria cases per quarter and per year in the Kati health district from 2018 to 2022.
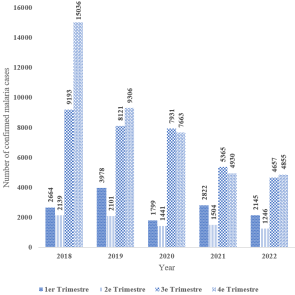
3.5. Comparison of Annual Confirmed Malaria Cases by Quarter in the Markala Health District
Figure 2. Number of confirmed malaria cases per quarter and per year in the Markala health district.
The number of confirmed malaria cases in the Markala district showed an epidemic peak during the high transmission period (3rd and 4th quarters) throughout the study period. However, malaria also appeared to be more chronic and endemic.
4. Discussion
4.1. Predominance of Subjects Aged 5 and over
Our study reveals that the majority of suspected malaria cases (70.2%) involved individuals aged 5 years and older. This finding is consistent with data from Togola et al. (2022) and Keita N, who reported an increasing proportion of cases among older children and adults in areas of seasonal transmission
| [9] | OB Togola et al., “Analysis of Malaria Surveillance Data in Mali from 2017 to 2019”, Sci. Tech. Sci. Sante, vol. 45, no. 2, pp. 175–192, 2022, Accessed March 4, 2026. [Online]. Available at:
https://www.ajol.info/index.php/stss/article/view/249528 |
| [10] | Naman KEITA, “ Study of the Seasonality of Malaria in Children from 0 to 15 Years at the District Hospital of Commune IV of Bamako, Mali in 2023”, Thesis, University of sciences, techniques and technologies of Bamako faculty of medicine and odontostomatology, Bamako, 2024. |
[9, 10]
. This result can be explained by immunity acquired in endemic areas such as Kati and Markala; repeated exposure to the parasite allows adults to develop some clinical immunity. Individuals over 5 years of age (schoolchildren, agricultural workers) often engage in nighttime or twilight activities outdoors, increasing their risk of being bitten by Anopheles mosquitoes, unlike infants who are more often protected under mosquito nets after sunset
| [6] | Global Malaria Community and Medicines for Malaria Venture (MMV), “Malaria in Mali: Statistics | Severe Malaria Observatory”, SEVERE MALARIA OBSERVATORY (SMO). Accessed: 22 February 2026. [Online]. Available at:
https://www.severemalaria.org/fr/pays/mali |
| [11] | SS Kambou, “Behavioral resistance: characterization and impact of sensory detection by malaria-carrying mosquitoes of control tools,” Theses, University of Montpellier, 2024. Accessed: March 4, 2026. [Online]. Available at:
https://theses.hal.science/tel-04957482 |
| [12] | World Health Organization, “World Malaria Report 2022.”, WHO, Geneva, 2022. |
[6, 11, 12]
.
4.2. Vulnerability of Children Under 5
Although numerically fewer in our table (29.8%), children under 5 years of age constitute the most vulnerable group. According to Kabore (2019), the burden of disease is more critical in this age group due to the lack of protective immunity
| [13] | ST Kaboré, “Regional disparities in malaria morbidity among children under five years of age in Burkina Faso,” Sidbewende Theodore Kabore, vol. HAL Id: hal-02527694, no. hal -02527694, p. 21, Apr. 2020, [Online]. Available at:
https://auf.hal.science/hal-02527694v1 |
[13]
. The difference in proportion between Markala (32%) and Kati (28.4%) for this age group could suggest earlier parasite pressure in Markala, a rice-growing area conducive to permanent larval habitats.
4.3. Female Predominance
Our results highlight a higher vulnerability or notification rate among women, reaching up to 78% in Kati in 2022. This observation is consistent with data from the Mali Malaria Indicator Survey (MIIS, 2021), which underscores increased use of health services by women
| [5] | National Institute of Statistics (INSTAT), Bamako, Mali, National Malaria Control Program (PNLP), Bamako, Mali, and The DHS Program (ICF), Rockville, Maryland, USA, “Survey Report on Malaria Indicators in Mali 2021”, INSTAT, Bamako, 2022. |
[5]
. Factors that may explain this disparity include the fact that in Mali, pregnant women benefit from free malaria diagnosis and treatment policies, as well as the free distribution of insecticide-treated bed nets (ITNs) during prenatal consultations. This targeted care promotes better malaria case capture among women in the DHIS2 system compared to adult men. Early morning and evening domestic activities (water collection, preparing meals outdoors) expose women more to Anopheles mosquito bites during peak vector activity hours. Our figures are higher than those reported by Tapily et al. (2020) in a study conducted in Bamako, which found a female predominance of 54%
| [14] | A. Tapily, “Spatial Variation of Malaria Transmission in Urban Areas: Case of the District of Bamako, Mali”, International Journal of Biological and Chemical Sciences 18(4): 1522-1540 https://doi.org/10.4314/ijbcs.v18i4.24 |
[14]
. The accentuation of this trend in 2021 and 2022 in our study area (78% in Kati) could suggest an improvement in systematic screening among women in community health centers (CSCOM) in the districts of Kati and Markala.
Conversely, the proportion of men is gradually decreasing in the statistics (only 22% in Kati in 2022). As indicated by Mboni in 2023, men in rural or peri-urban areas often tend to resort to self-medication or traditional medicine, only going to health facilities in case of complications
| [15] | HM Mboni et al., “ Evaluation of self-medication practices and their characteristics among students in Uvira in the Democratic Republic of Congo”, Pan Afr. Med. J., vol. 45, no. 53, May 2023, https://doi.org/10.11604/pamj.2023.45.53.39690. |
[15]
, which leads to an underreporting of simple male cases in official reports.
The male predominance among those under 5 years old (53.8%) and female predominance among those 5 years and older (54.6%) could reflect dynamics of exposure or attendance at health facilities specific to each district and age group.
4.4. Geographic and Seasonal Dynamics
The reversal in prevalence between Kati and Markala from 2021 onwards is a major finding. The initially high prevalence in Markala can be explained by its epidemiological characteristics: the proximity of the Niger River and the rice-growing areas create permanent larval breeding sites. The decrease observed in Markala at the end of the period (3.93% in 2022) could reflect the effectiveness of prevention campaigns (distribution of long-lasting insecticidal nets). Meanwhile, the increase in Kati (7.80%) could be linked to improved data completeness in the reporting system or to increased parasite pressure in this densely populated district.
The results of our study revealed that during the study periods, the Markala district recorded higher malaria prevalence rates than Kati, from 2018 to 2020, reaching up to 8.72% of confirmed cases, compared to 5.97% in Kati in 2018. These results were consistent with those of Kouyate et al. (2021)
| [7] | Kouyaté, M., Keïta, M., Sidibé, A., & Traoré, M. (2021)., “Study of the prevalence of malaria in rural and urban districts”. Journal of Malian Health Studies, 15(3), 142-157.
https://doi.org/10.3389/fmala.2025.1596496 |
[7]
, where the prevalence in the Kati district was 30%, while Markala showed slightly higher rates, around 32%, highlighting a persistent trend of higher transmission in rural areas. This finding is consistent with those of Mugabo et al. (2024)
| [16] | AS: Mugabo Kalisa G. (2024). Comparative Analysis of Malaria Transmission in Urban and Rural Settings: Exploring Population Density, Sanitation, and Vector Ecology to Address Regional Disparities in Malaria Risk. Eurasian experiment journal of scientific and applied research, 6(3): 27-32.
https://www.eejournals.org |
[16]
, who also found an overall malaria prevalence in rural areas of Mali (such as Markala) of around 35% to 40%, while in urban areas (such as Kati), the prevalence was lower, around 15% to 20%.
This trend is attributed to the rainy season, which is conducive to mosquito breeding. Diallo et al. (2024)
| [17] | Diallo, D., et al. (2024). Evaluation of the performance of rapid diagnostic tests for malaria diagnosis and mapping of different Plasmodium species in Mali. International Journal of Environmental Research and Public Health, 21(2), 228.
https://doi.org/10.3390/ijerph21020228. |
[17]
reported that the annual prevalence in Kati in 2019 showed transmission peaks during the third and fourth quarters, with rates reaching 42.1% and 40.7%, respectively. Diarra et al. (2022)
| [18] | Diarra, Y., Coulibaly, K., Sangaré, M., & Diarra, T. (2022)., “Seasonal patterns in malaria transmission in Mali. International Journal of Malaria Control, 22(1), 32-45. ". Spatio-temporal analysis of malaria within a transmission season in Bandiagara, Mali. Malaria Journal. Volume 12, article numéro 82, (2013),
https://doi.org/10.1186/1475-2875-12-82 |
[18]
also reported results for the same period, although not specifically detailed for each quarter, revealing high prevalences during the rainy season, a period during which malaria transmission rates increase. The distribution of cases also follows this dynamic, with a peak in cases observed in the third and fourth quarters in rural areas such as Markala.
4.5. The Influence of the Epidemiological Profile
The initially higher prevalence in Markala (8.72% in 2018) is closely linked to its hydrographic environment. The proximity of the Niger River and the presence of rice-growing areas create ideal ecological conditions (constant humidity, stagnant water) for the continued existence of Anopheles larval habitats. This observation aligns with the findings of Sissoko et al., who emphasize that dam and rice-growing areas in Mali exhibit more sustained transmission
| [19] | M. Cissoko, “ Study of the epidemiology of malaria according to meteorological and societal factors in Mali”, thesis, Aix-Marseille, 2022. Accessed: February 23, 2026. [Online]. Available at: https://theses.fr/2022AIXM0245 |
[19]
.
4.6. Seasonality and Climate Change
The significantly higher prevalence in Markala during the first three years of the study (8.72% in 2018) is explained by its biophysical environment. Located in a rice-growing area near the Niger River, Markala presents an epidemiological profile of the "lagoon" or "rice-growing" type, characterized by a near-permanent presence of larval breeding sites. According to Dossou et al. (1989), irrigated agricultural areas in Mali promote more intense and prolonged malaria transmission than dry savanna areas, due to the persistent humidity which favors the survival of vectors (Anopheles). gambiae)
| [20] | J. Dossou- Yovo, A. Ouattara, JMC Doannio, S. Diarrassouba, and G. Chauvancy, “Paludometric surveys in the humid savannah zone of Côte d'Ivoire,” Medecine Trop., vol. 58, no. 1, 1998, accessed: March 5, 2026. [Online]. Available from:
https://www.documentation.ird.fr/hor/fdi:010014918 |
[20]
.
The shift observed in 2021, where Kati became more affected (5.90% then 7.80% in 2022), is a significant finding. This increase in Kati could be attributed to rapid urbanization. As a crossroads city with strong population growth, Kati faces sanitation challenges. Wastewater and construction sites create new urban breeding grounds for malaria larvae, a phenomenon described by Dossou et al. (1998) and Ntonka et al. as "urban malaria," where transmission is no longer solely dependent on rainfall
| [21] | P. Ntonga Akono, A. Mbida Mbida, P. Awono Ambene, L. Youmbi Enga, Y. Abdel Kayoum, and S. Kekeunou, “Larval habitats and sensitivity of malaria vectors to insecticides in localities (semi-urban and rural) of the coastal region of Cameroon: preliminary data”, 2018,
https://doi.org/10.3406/revec.2018.1921. |
| [22] | D. Belisse and PL Vanessa, “Mosquito population dynamics and malaria transmission during a larvicide program in the city of Yaounde, Cameroon,” Thesis, University of Yaounde I, 2022. Accessed: March 5, 2026. [Online]. Available from:
https://dicames.online/jspui/handle/20.500.12177/11129 |
[21, 22]
. Improved reporting completeness in the DHIS2 system in Kati could also explain this apparent increase in cases compared to previous years.
4.7. Effectiveness of Control Measures in Markala
The continued decline in prevalence in Markala (from 8.72% to 3.93%) suggests a positive impact of public health interventions. As highlighted in the 2022 National Malaria Control Program (NMCP) annual report, the scaling up of Long-Lasting Insecticide-Treated Net (LLIN) distribution and Seasonal Malaria Chemoprevention (SMC) in high-risk areas like Markala has significantly reduced the disease burden
| [23] | National Malaria Control Programme (PNLP), “Annual Report on Malaria Control in Mali. Ministry of Health and Social Development.”, Ministry of Health and Social Development, Bamako, Annual, 2022. |
[23]
. The favorable prevalence gap in Markala in 2022 demonstrates the success of these local strategies.
4.8. The Predominance of the RDT
The widespread use of rapid diagnostic tests (RDTs) (approximately 60%) in both districts aligns with the WHO (2022) and National Malaria Control Program (NMCP) guidelines, which recommend systematic laboratory testing before any treatment. The simplicity of RDTs, requiring neither electricity nor advanced microscopic expertise, explains their widespread adoption, particularly in the community health centers (CSCOMs) of Markala.
4.9. The Specificity of the Thick Drop in Kati
The high rate of smear microscopy (SM) in Kati (up to 30.03%) compared to Markala (6.08%) reflects a difference in technical capacity. Kati, being a more urban district with denser hospital infrastructure, has a better capacity for microscopic diagnosis. As Benaiou et al. (2024) point out, SM remains the gold standard because it not only confirms the Plasmodium species but also quantifies parasitemia, which is essential for monitoring severe cases
| [24] | Benaiou and F. Mahammedi, “Evaluation of biological diagnostic procedures for specific Plasmodium infections in the southern region (The Sahara)”, Thesis, KASDI MERBAH UNIVERSITY – OUARGLA, 2024. Accessed: March 5, 2026. [Online]. Available at:
http://dspace.univ-ouargla.dz/jspui/handle/123456789/37541 |
[24]
.
4.10. Convergence of Practices in 2022
The disappearance of the significant difference for RDTs in 2022 (p=0.90) suggests a standardization of care practices. This result could reflect improved availability of supplies (RDT kits) throughout the country thanks to the efforts of the National Malaria Control Program. This "diagnostic equity" is crucial for reducing presumptive treatment (treating without evidence), which is a major cause of antimalarial drug resistance according to the WHO. (2023)
.
5. Conclusions
This comparative study made it possible to establish the epidemiological burden of malaria and to highlight significant differences in prevalence between the health districts of Kati and Markala in the period from 2018 to 2022. It also underlines the importance of malaria cases according to age, the age group of 5 years and over and the variability of prevalence according to sex and age, offering avenues for adapting malaria control strategies.
Abbreviations
DHIS2 | District Health Information Software 2 |
CPS | Chemoprevention of Seasonal Malaria |
MIILD | Long-lasting Insecticide-treated Bed Nets |
PNLP | National Malaria Control Programs |
RDT | Rapid Diagnostic Tests |
GE | Thick Drop |
EIPM | Survey on Malaria Indicators in Mali |
CPS | Chemoprevention of Seasonal Malaria |
WHO | World Health Organization |
DS | Health District |
CSCOM | Community Health Center |
ASACO | Community Health Association |
GE | Thick Drop |
DERSP | Department of Teaching and Research in Public Health |
FMOS | Faculty of Medicine and Odonto- Stomatology |
USTTB | University of Sciences, Techniques and Technologies of Bamako |
Acknowledgments
The authors wish to express their gratitude to the Department of Teaching and Research in Public Health (DERSP) of the Faculty of Medicine and Odonto-Stomatology (Bamako, Mali) for the institutional and technical support provided throughout this research.
The authors thank the health authorities of the health district of Commune I in the Bamako district. We would also like to thank the staff of the CSCOM-U for their availability and technical support, the members of the Banconi Community Health Association (ASACOBA) for their support and availability, and all the participants who took part in this study.
Author Contributions
Fanta Sangho: Conceptualization, Project administration, Resources, Validation, Writing – review & editing
Borodjan Diarra: Conceptualization, Formal Analysis, Supervision, Writing – review & editing
Cheick Abou Coulibaly: Conceptualization, Formal Analysis, Writing – review & editing, Validation
Fatoumata Bintou Konate: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft
Oumar Kone: Writing – review & editing
Mariam Sekou Kone: Writing – review & editing
Souleymane Sekou Diarra: Writing – review & editing
Abdoul Salam Diarra: Writing – review & editing
Abou Sogodogo: Writing – review & editing
Mariam Bocar Toure: Writing – review & editing
Jean Paul Tchapebong: Writing – review & editing
Salia Keita: Writing – review & editing
Oumar Sangho: Project administration, Resources, Supervision, Validation
Data Availability Statement
The data is available from the corresponding author upon request. Reasonable request.
The data supporting the results of this research are presented in this manuscript.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
| [1] |
World Health Organization, “World Malaria Report 2025”, WHO, Geneva, Summary, Dec. 2025.
|
| [2] |
African Union, ALMA, and RBM Partnership to End Malaria, “African Union Malaria Progress Report 2025”, 39th AU Summit, Addis Ababa, Feb. 2026.
|
| [3] |
World Health Organization, “2024 Global Malaria Report”, WHO, Geneva, 2024.
|
| [4] |
Directorate General of Health and Public Hygiene of the Ministry of Health of Mali, “Directory of the local health information system of Mali 2022”. Bamako, 2022.
|
| [5] |
National Institute of Statistics (INSTAT), Bamako, Mali, National Malaria Control Program (PNLP), Bamako, Mali, and The DHS Program (ICF), Rockville, Maryland, USA, “Survey Report on Malaria Indicators in Mali 2021”, INSTAT, Bamako, 2022.
|
| [6] |
Global Malaria Community and Medicines for Malaria Venture (MMV), “Malaria in Mali: Statistics | Severe Malaria Observatory”, SEVERE MALARIA OBSERVATORY (SMO). Accessed: 22 February 2026. [Online]. Available at:
https://www.severemalaria.org/fr/pays/mali
|
| [7] |
Kouyaté, M., Keïta, M., Sidibé, A., & Traoré, M. (2021)., “Study of the prevalence of malaria in rural and urban districts”. Journal of Malian Health Studies, 15(3), 142-157.
https://doi.org/10.3389/fmala.2025.1596496
|
| [8] |
M. Kamissoko, “The prevalence of malaria during pregnancy in the Bamako district,” University of Sciences, Techniques and Technologies of Bamako (USTTB)/Faculty of Medicine and Odonto-Stomatology (FMOS), Bamako, Mali, 2015. Accessed: February 22, 2026. [Online]. Available from:
https://www.bibliosante.ml/handle/123456789/973
|
| [9] |
OB Togola et al., “Analysis of Malaria Surveillance Data in Mali from 2017 to 2019”, Sci. Tech. Sci. Sante, vol. 45, no. 2, pp. 175–192, 2022, Accessed March 4, 2026. [Online]. Available at:
https://www.ajol.info/index.php/stss/article/view/249528
|
| [10] |
Naman KEITA, “ Study of the Seasonality of Malaria in Children from 0 to 15 Years at the District Hospital of Commune IV of Bamako, Mali in 2023”, Thesis, University of sciences, techniques and technologies of Bamako faculty of medicine and odontostomatology, Bamako, 2024.
|
| [11] |
SS Kambou, “Behavioral resistance: characterization and impact of sensory detection by malaria-carrying mosquitoes of control tools,” Theses, University of Montpellier, 2024. Accessed: March 4, 2026. [Online]. Available at:
https://theses.hal.science/tel-04957482
|
| [12] |
World Health Organization, “World Malaria Report 2022.”, WHO, Geneva, 2022.
|
| [13] |
ST Kaboré, “Regional disparities in malaria morbidity among children under five years of age in Burkina Faso,” Sidbewende Theodore Kabore, vol. HAL Id: hal-02527694, no. hal -02527694, p. 21, Apr. 2020, [Online]. Available at:
https://auf.hal.science/hal-02527694v1
|
| [14] |
A. Tapily, “Spatial Variation of Malaria Transmission in Urban Areas: Case of the District of Bamako, Mali”, International Journal of Biological and Chemical Sciences 18(4): 1522-1540
https://doi.org/10.4314/ijbcs.v18i4.24
|
| [15] |
HM Mboni et al., “ Evaluation of self-medication practices and their characteristics among students in Uvira in the Democratic Republic of Congo”, Pan Afr. Med. J., vol. 45, no. 53, May 2023,
https://doi.org/10.11604/pamj.2023.45.53.39690.
|
| [16] |
AS: Mugabo Kalisa G. (2024). Comparative Analysis of Malaria Transmission in Urban and Rural Settings: Exploring Population Density, Sanitation, and Vector Ecology to Address Regional Disparities in Malaria Risk. Eurasian experiment journal of scientific and applied research, 6(3): 27-32.
https://www.eejournals.org
|
| [17] |
Diallo, D., et al. (2024). Evaluation of the performance of rapid diagnostic tests for malaria diagnosis and mapping of different Plasmodium species in Mali. International Journal of Environmental Research and Public Health, 21(2), 228.
https://doi.org/10.3390/ijerph21020228.
|
| [18] |
Diarra, Y., Coulibaly, K., Sangaré, M., & Diarra, T. (2022)., “Seasonal patterns in malaria transmission in Mali. International Journal of Malaria Control, 22(1), 32-45. ". Spatio-temporal analysis of malaria within a transmission season in Bandiagara, Mali. Malaria Journal. Volume 12, article numéro 82, (2013),
https://doi.org/10.1186/1475-2875-12-82
|
| [19] |
M. Cissoko, “ Study of the epidemiology of malaria according to meteorological and societal factors in Mali”, thesis, Aix-Marseille, 2022. Accessed: February 23, 2026. [Online]. Available at:
https://theses.fr/2022AIXM0245
|
| [20] |
J. Dossou- Yovo, A. Ouattara, JMC Doannio, S. Diarrassouba, and G. Chauvancy, “Paludometric surveys in the humid savannah zone of Côte d'Ivoire,” Medecine Trop., vol. 58, no. 1, 1998, accessed: March 5, 2026. [Online]. Available from:
https://www.documentation.ird.fr/hor/fdi:010014918
|
| [21] |
P. Ntonga Akono, A. Mbida Mbida, P. Awono Ambene, L. Youmbi Enga, Y. Abdel Kayoum, and S. Kekeunou, “Larval habitats and sensitivity of malaria vectors to insecticides in localities (semi-urban and rural) of the coastal region of Cameroon: preliminary data”, 2018,
https://doi.org/10.3406/revec.2018.1921.
|
| [22] |
D. Belisse and PL Vanessa, “Mosquito population dynamics and malaria transmission during a larvicide program in the city of Yaounde, Cameroon,” Thesis, University of Yaounde I, 2022. Accessed: March 5, 2026. [Online]. Available from:
https://dicames.online/jspui/handle/20.500.12177/11129
|
| [23] |
National Malaria Control Programme (PNLP), “Annual Report on Malaria Control in Mali. Ministry of Health and Social Development.”, Ministry of Health and Social Development, Bamako, Annual, 2022.
|
| [24] |
Benaiou and F. Mahammedi, “Evaluation of biological diagnostic procedures for specific Plasmodium infections in the southern region (The Sahara)”, Thesis, KASDI MERBAH UNIVERSITY – OUARGLA, 2024. Accessed: March 5, 2026. [Online]. Available at:
http://dspace.univ-ouargla.dz/jspui/handle/123456789/37541
|
| [25] |
WHO, “Malaria: Management of Plasmodium falciparum malaria patients jeopardized in the Horn of Africa”, Pasteur Institute. Accessed: 5 March 2026. [Online]. Available at:
https://www.pasteur.fr/fr/espace-presse/documents-presse/paludisme-prise-charge-malades-du-paludisme-plasmodium-falciparum-mise-peril-corne-afrique
|
Cite This Article
-
APA Style
Sangho, F., Diarra, B., Coulibaly, C. A., Konate, F. B., Kone, O., et al. (2026). Contrasting Dynamics of Malaria: Comparative Analysis Between Peri-urban (Kati) and Hydro-agricultural (Markala) Environments in Mali 2018-2022. World Journal of Public Health, 11(2), 146-154. https://doi.org/10.11648/j.wjph.20261102.16
 Copy
|
Copy
|
 Download
Download
ACS Style
Sangho, F.; Diarra, B.; Coulibaly, C. A.; Konate, F. B.; Kone, O., et al. Contrasting Dynamics of Malaria: Comparative Analysis Between Peri-urban (Kati) and Hydro-agricultural (Markala) Environments in Mali 2018-2022. World J. Public Health 2026, 11(2), 146-154. doi: 10.11648/j.wjph.20261102.16
Copy
|
Download
AMA Style
Sangho F, Diarra B, Coulibaly CA, Konate FB, Kone O, et al. Contrasting Dynamics of Malaria: Comparative Analysis Between Peri-urban (Kati) and Hydro-agricultural (Markala) Environments in Mali 2018-2022. World J Public Health. 2026;11(2):146-154. doi: 10.11648/j.wjph.20261102.16
Copy
|
Download
-
@article{10.11648/j.wjph.20261102.16,
author = {Fanta Sangho and Borodjan Diarra and Cheick Abou Coulibaly and Fatoumata Bintou Konate and Oumar Kone and Mariam Sekou Kone and Souleymane Sekou Diarra and Abdoul Salam Diarra and Abou Sogodogo and Mariam Bocar Toure and Jean Paul Tchapebong and Salia Keita and Oumar Sangho},
title = {Contrasting Dynamics of Malaria: Comparative Analysis Between Peri-urban (Kati) and Hydro-agricultural (Markala) Environments in Mali 2018-2022},
journal = {World Journal of Public Health},
volume = {11},
number = {2},
pages = {146-154},
doi = {10.11648/j.wjph.20261102.16},
url = {https://doi.org/10.11648/j.wjph.20261102.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20261102.16},
abstract = {Malaria remains a major public health burden in Mali, requiring control strategies adapted to local epidemiological contexts. This study compared the evolution of malaria prevalence and determinants in the health districts of Kati (peri-urban/agricultural area) and Markala (agricultural/hydro-agricultural area). This was a cross-sectional, comparative study of malaria data from the districts of Kati and Markala from January 2018 to December 2022. The data were extracted from the District Health Information Software 2. The comparative statistical analysis used Chi-square tests and logistic regressions to identify the factors associated (age, sex, seasonality) with the observed variations. A total of 422,020 Cases of malaria were recorded in both districts. The Markala district had a higher average annual prevalence than Kati (6.038% vs 6.024%, p=0.001), although annual trends showed significant variability, notably a more pronounced increase in Kati in 2021. Seasonal analysis confirmed the epidemic peak during the high transmission period (July-October) in both districts, but the malaria burden in Markala appeared to be more chronic and less strictly seasonal, potentially linked to agricultural irrigation. This study revealed an epidemiological shift in Mali, with marked heterogeneity between peri-urban and hydro-agricultural areas. The increased prevalence in Kati in 2022 and the shift in disease burden towards those over 5 years of age, particularly women, necessitate adapting national strategies. Environmental management of rice cultivation, targeting of adults, and improved quality of routine data are crucial for precision vector control.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Contrasting Dynamics of Malaria: Comparative Analysis Between Peri-urban (Kati) and Hydro-agricultural (Markala) Environments in Mali 2018-2022
AU - Fanta Sangho
AU - Borodjan Diarra
AU - Cheick Abou Coulibaly
AU - Fatoumata Bintou Konate
AU - Oumar Kone
AU - Mariam Sekou Kone
AU - Souleymane Sekou Diarra
AU - Abdoul Salam Diarra
AU - Abou Sogodogo
AU - Mariam Bocar Toure
AU - Jean Paul Tchapebong
AU - Salia Keita
AU - Oumar Sangho
Y1 - 2026/04/28
PY - 2026
N1 - https://doi.org/10.11648/j.wjph.20261102.16
DO - 10.11648/j.wjph.20261102.16
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 146
EP - 154
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20261102.16
AB - Malaria remains a major public health burden in Mali, requiring control strategies adapted to local epidemiological contexts. This study compared the evolution of malaria prevalence and determinants in the health districts of Kati (peri-urban/agricultural area) and Markala (agricultural/hydro-agricultural area). This was a cross-sectional, comparative study of malaria data from the districts of Kati and Markala from January 2018 to December 2022. The data were extracted from the District Health Information Software 2. The comparative statistical analysis used Chi-square tests and logistic regressions to identify the factors associated (age, sex, seasonality) with the observed variations. A total of 422,020 Cases of malaria were recorded in both districts. The Markala district had a higher average annual prevalence than Kati (6.038% vs 6.024%, p=0.001), although annual trends showed significant variability, notably a more pronounced increase in Kati in 2021. Seasonal analysis confirmed the epidemic peak during the high transmission period (July-October) in both districts, but the malaria burden in Markala appeared to be more chronic and less strictly seasonal, potentially linked to agricultural irrigation. This study revealed an epidemiological shift in Mali, with marked heterogeneity between peri-urban and hydro-agricultural areas. The increased prevalence in Kati in 2022 and the shift in disease burden towards those over 5 years of age, particularly women, necessitate adapting national strategies. Environmental management of rice cultivation, targeting of adults, and improved quality of routine data are crucial for precision vector control.
VL - 11
IS - 2
ER -
Copy
|
Download