People living with Parkinson’s disease or with essential tremors face many obstacles in their everyday lives. Being able to eat independently is one of them. Many technologies already exist to help people who have difficulty eating independently. However, following a review of existing devices with a team of occupational therapists, it was found that many commercially available solutions were either unhelpful or too expensive. The need for better adapted solutions was obvious so an iterative design methodology based on the user's needs was followed to create a new anti-tremor utensil. The starting point of the design was to analyze the existing utensils to understand better the pros and cons of the available solutions. During the iterative design methodology, several prototypes emerged and led to the creation of the final spoon prototype presented in this paper. A total of 5 different adaptative spoons were designed and are presented in this paper. A sensor-based frequential analysis combined with an occupational therapist review indicates that the proposed prototype is effective against certain types of tremors and that it could potentially help people living with tremor while they eat. The next step of the development will be to test the new prototype with potential users.
| Published in | Applied Engineering (Volume 8, Issue 1) |
| DOI | 10.11648/j.ae.20240801.15 |
| Page(s) | 47-60 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Occupational Therapy, Anti-Tremor Spoon, Assistive Eating Device, Essential Tremor, Parkinson Disease
6.1. Prototype 1 - Swivel Spoon
6.2. Prototype 2 - Four-Bar Mechanism Spoon
6.3. Prototype 3 - Balanced Spoon
6.4. Prototype 4 - Swivel and Balanced Spoon
6.5. Final Prototype - Spherical Balanced Spoon
Spoon model | Characteristics |
|---|---|
Final prototype – Spherical balanced spoon | Two degrees of freedom between the spoon and the handle (it means the handle can move/rotate in two directions without affecting the spoon) The spoon is balanced and stays in the same orientation. |
Zero degree of freedom between spoon and handle. The weight lowers the natural frequency of the spoon, which lowers the impact of tremors. | |
One degree of freedom between spoon and handle. | |
Two degrees of freedom between spoon and handle. Contains motors and sensors. |
7.1. Methodology of Vibration Testing
7.2. Results of Vibration Testing
8.1. Methodology of Occupational Therapists’ Review
8.2. Occupational Therapists Review
| [1] | Statistics Canada, “Disability in Canada: initial findings from the Canadian Survey on Disability”, 2013. |
| [2] |
Parkinson’s Foundation, Statistics. Available:
https://www.parkinson.org/Understanding-Parkinsons/Statistics#:~:text=Who%20Has%20Parkinson’s%3F&text=Approximately%2060%2C000%20Americans%20are%20diagnosed,are%20diagnosed%20before%20age%2050 (Accessed: 04-april-2020) |
| [3] | Ramage-Morin, P. (2014). Parkinson’s disease: Prevalence, diagnosis and impact. |
| [4] | Louis, E. D., & Ottman, R. (2014). How Many People in the USA Have Essential Tremor? Deriving a Population Estimate Based on Epidemiological Data. Tremor and Other Hyperkinetic Movements, 4(0), 259. |
| [5] |
Sunnybrook Research Institute, Essential tremor. Available:
https://sunnybrook.ca/research/content/?page=sri-centres-focused-ultrasound-tremor#:~:text=Photo%3A%20Doug%20Nicholson.,of%20the%20population%20in%20Canada (Accessed: 04-april-2020) |
| [6] |
“La maladie de Parkinson: prévalence, diagnostic et conséquences.” [Online]. Available:
https://www150.statcan.gc.ca/n1/pub/82-003-x/2014011/article/14112-fra.htm (Accessed: 20-Oct-2020). |
| [7] | S. Federici, F. Meloni, and S. Borsci, “The abandonment of assistive technology in Italy: a survey of National Health Service users.,” Eur. J. Phys. Rehabil. Med., vol. 52, no. 4, pp. 516–26, Aug. 2016. |
| [8] | R. Verza, M. L. L. Carvalho, M. A. Battaglia, and M. M. Uccelli, “An interdisciplinary approach to evaluating the need for assistive technology reduces equipment abandonment,” (2006), Mult. Scler. J., vol. 12, no. 1, pp. 88–93. |
| [9] | R. Arim, A profile of persons with disabilities among Canadians aged 15 years or older. (2012) Statistics Canada. |
| [10] | A. G. Dell, D. A. Newton, and J. G. Petroff, Assistive technology in the classroom: Enhancing the school experiences of students with disabilities. (2008), Pearson. |
| [11] | Statistics Canada. Participation and Activity Limitation Survey: Assistive aids and devices for adults, 2008. |
| [12] | M. L. Riemer-Reiss and R. R. Wacker, “Factors associated with assistive technology discontinuance among individuals with disabilities,” J. Rehabil., vol. 66, no. 3, 2000. |
| [13] | Guo, M., Shi, P., & Yu, H. (2017). Development a feeding assistive robot for eating assist. 2017 2nd Asia-Pacific Conference on Intelligent Robot Systems, ACIRS 2017, 299–304. |
| [14] |
“Manque criant de personnel dans les CHSLD” [Online]. Available:
https://www.lapresse.ca/actualites/sante/2019-09-26/manque-criant-de-personnel-dans-leschsld [Accessed: 06-Nov-2020]. |
| [15] |
“Plus de 60 000 travailleurs de la santé recherchés | Le Devoir.” [Online]. Available:
https://www.ledevoir.com/politique/quebec/553217/mot-cle-besoin-de-60-000-travailleurs-de-lasante-d-ici-5-ans [Accessed: 06-Nov-2020]. |
| [16] | H. F. M. Van der Loos, D. J. Reinkensmeyer, and E. Guglielmelli, “Rehabilitation and health care robotics,” (2016), in Springer handbook of robotics, Springer, pp. 1685–1728. |
| [17] | R. Choinière, Vieillissement de la population, état fonctionnel des personnes âgées et besoins futurs en soins de longue durée au Québec. (2010) Institut national de santé publique Québec. |
| [18] | S. Chatterji, J. Byles, D. Cutler, T. Seeman, and E. Verdes, “Health, functioning, and disability in older adults—present status and future implications,” (2015), Lancet, vol. 385, no. 9967, pp. 563–575. |
| [19] |
Government of Canada – Action for Seniors report (2014). Available:
https://www.canada.ca/en/employment-social-development/programs/seniors-action-report.html (Accessed: 04-april-2020) |
| [20] |
An Aging Nation: Projected Number of Children and Older Adults (2018). Available:
https://www.census.gov/library/visualizations/2018/comm/historic-first.html (Accessed: 04-april-2020) |
| [21] | A.Q. Rana and K. L. Chou, Essential Tremor in Clinical Practice. (2015), Cham: Springer International Publishing. |
| [22] | M. J. Fuhrer, “Subjectifying quality of life as a medical rehabilitation outcome.,”, (2000), Disabil. Rehabil., vol. 22, no. 11, pp. 481–489. |
| [23] | D. Yachnin, G. Gharib, J. Jutai, and H. Finestone, “Technology-assisted toilets: Improving independence and hygiene in stroke rehabilitation.,”, (2017), J. Rehabil. Assist. Technol. Eng., vol. 4. |
| [24] | J. A. Lenker, F. Harris, M. Taugher, and R. O. Smith, “Consumer perspectives on assistive technology outcomes.,” (2013), Disabil. Rehabil. Assist. Technol., vol. 8, no. 5, pp. 373–380, Sep. |
| [25] |
Sure Grip Weighted Utensils | Adaptive Eating Utensils | Performance Health. [Online]. Available:
https://www.performancehealth.ca/sure-grip-weighted-utensils [Accessed: 20-Oct-2020]. |
| [26] |
Performance Health, “Steady spoon”. Available from:
https://www.performancehealth.ca/steady-spoons [Accessed: 20-Oct-2020]. |
| [27] |
Homepage - ELISpoon. [Online]. Available:
https://elispoon.com/ [Accessed: 20-Oct-2020]. |
| [28] |
Liftware Level | Liftware. [Online]. Available:
https://www.liftware.com/level/ [Accessed: 20-Oct-2020]. |
| [29] |
Liftware Steady | Liftware. [Online]. Available:
https://www.liftware.com/steady/ [Accessed: 20-Oct-2020]. |
| [30] | Pathak, A. J., & Owens, D. U.S. Patent Application No. 10/058,445, 2018. |
| [31] | J. L. Pons, E. Rocon, A. F. Ruiz, and J. C. Moreno, “Upper-limb robotic rehabilitation exoskeleton: Tremor suppression,” (2007), in Rehabilitation robotics, InTech. |
| [32] |
Obi – The first dining robot of its kind. [Online]. Available:
https://meetobi.com/ [Accessed: 20-Oct-2020]. |
| [33] | Hallett, M. (2013). Parkinsonism and Related Disorders 20S1 (2014) S118-S122 Tremor: Pathophysiology. |
| [34] | DeLong, M. R., Huang, K. T., Gallis, J., Lokhnygina, Y., Parente, B., Hickey, P., Turner, D. A., & Lad, S. P. (2014). Effect of advancing age on outcomes of deep brain stimulation for parkinson disease. JAMA Neurology, 71(10), 1290–1295. |
| [35] | Louis, E. D., Yu, Q., Floyd, A. G., Moskowitz, C., & Pullman, S. L. (2006). Axis is a feature of handwritten spirals in essential tremor. Movement Disorders, 21(8), 1294–1295. |
| [36] | Calzetti, S., Baratti, M., Gresty, M., & Findleyt, L. (1987). Frequency/amplitude characteristics of postural tremor of the hands in a population of patients with bilateral essential tremor: implications for the classification and mechanism of essential tremor. Consortia. Protected by Copyright. on February, 50, 561–567. |
| [37] | Woods, A. M., Nowostawski, M., Franz, E. A., & Purvis, M. (2014). Parkinson’s disease and essential tremor classification on mobile device. Pervasive and Mobile Computing, 13, 1–12. |
| [38] |
Channels Television, “Gyroscope Gloves Reduces Hand Tremors For Parkinson's Patients”. Available from:
https://www.youtube.com/watch?v=eZvvB9WX1Tg&ab_channel=ChannelsTelevision (@ 0:45). [Accessed 28 April 2024]. |
| [39] |
Brian Allen, ““Smart” Spoon for Parkinson's Sufferers”. Available:
https://www.youtube.com/watch?v=WiVQcgmIi08&ab_channel=BrianMKAllen (@ 0:06, 0:38, 0:56, 1:14). [Accessed 28 April 2024]. |
| [40] |
CTOOM Creative, “GYENNO Spoon – Smart Self-Stabilizing Spoon for Hand Tremor and Parkinson’s Sufferers”. Available from:
https://www.youtube.com/watch?v=dVd7M7xuK5w&ab_channel=CTOOMCreative (@ 0:08, 0:13). [Accessed 28 April 2024]. |
| [41] |
STAT, “Living with essential tremor”. Available from:
https://www.youtube.com/watch?v=SFnWlqQ1z60&ab_channel=STAT (@ 0:42, 0:49). [Accessed 28 April 2024]. |
| [42] |
Associated press, “Google Spoon Helps People With Tremors Eat”. Available from:
https://www.youtube.com/watch?v=99t5c6j8BR0&ab_channel=AssociatedPress (@ 0:12). [Accessed 28 April 2024]. |
| [43] |
Liftware, “Using Liftware: Berta (Severe Tremor)”. Available from:
https://www.youtube.com/watch?v=Yn8VDA_I6b8&ab_channel=Liftware (@ 2:33). [Accessed 28 April 2024]. |
| [44] | Brown, T., & Katz, B. (2011). Change by Design. Journal of Product Innovation Management, 28(3), 381-383. |
APA Style
Dubé, M., Laliberté, T., Flamand, V. H., Campeau-Lecours, A. (2024). Development of a New and Mechanically Intelligent Anti-Tremor Utensil. Applied Engineering, 8(1), 47-60. https://doi.org/10.11648/j.ae.20240801.15
ACS Style
Dubé, M.; Laliberté, T.; Flamand, V. H.; Campeau-Lecours, A. Development of a New and Mechanically Intelligent Anti-Tremor Utensil. Appl. Eng. 2024, 8(1), 47-60. doi: 10.11648/j.ae.20240801.15
@article{10.11648/j.ae.20240801.15,
author = {Michaël Dubé and Thierry Laliberté and Véronique H. Flamand and Alexandre Campeau-Lecours},
title = {Development of a New and Mechanically Intelligent Anti-Tremor Utensil
},
journal = {Applied Engineering},
volume = {8},
number = {1},
pages = {47-60},
doi = {10.11648/j.ae.20240801.15},
url = {https://doi.org/10.11648/j.ae.20240801.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ae.20240801.15},
abstract = {People living with Parkinson’s disease or with essential tremors face many obstacles in their everyday lives. Being able to eat independently is one of them. Many technologies already exist to help people who have difficulty eating independently. However, following a review of existing devices with a team of occupational therapists, it was found that many commercially available solutions were either unhelpful or too expensive. The need for better adapted solutions was obvious so an iterative design methodology based on the user's needs was followed to create a new anti-tremor utensil. The starting point of the design was to analyze the existing utensils to understand better the pros and cons of the available solutions. During the iterative design methodology, several prototypes emerged and led to the creation of the final spoon prototype presented in this paper. A total of 5 different adaptative spoons were designed and are presented in this paper. A sensor-based frequential analysis combined with an occupational therapist review indicates that the proposed prototype is effective against certain types of tremors and that it could potentially help people living with tremor while they eat. The next step of the development will be to test the new prototype with potential users.
},
year = {2024}
}
TY - JOUR T1 - Development of a New and Mechanically Intelligent Anti-Tremor Utensil AU - Michaël Dubé AU - Thierry Laliberté AU - Véronique H. Flamand AU - Alexandre Campeau-Lecours Y1 - 2024/05/17 PY - 2024 N1 - https://doi.org/10.11648/j.ae.20240801.15 DO - 10.11648/j.ae.20240801.15 T2 - Applied Engineering JF - Applied Engineering JO - Applied Engineering SP - 47 EP - 60 PB - Science Publishing Group SN - 2994-7456 UR - https://doi.org/10.11648/j.ae.20240801.15 AB - People living with Parkinson’s disease or with essential tremors face many obstacles in their everyday lives. Being able to eat independently is one of them. Many technologies already exist to help people who have difficulty eating independently. However, following a review of existing devices with a team of occupational therapists, it was found that many commercially available solutions were either unhelpful or too expensive. The need for better adapted solutions was obvious so an iterative design methodology based on the user's needs was followed to create a new anti-tremor utensil. The starting point of the design was to analyze the existing utensils to understand better the pros and cons of the available solutions. During the iterative design methodology, several prototypes emerged and led to the creation of the final spoon prototype presented in this paper. A total of 5 different adaptative spoons were designed and are presented in this paper. A sensor-based frequential analysis combined with an occupational therapist review indicates that the proposed prototype is effective against certain types of tremors and that it could potentially help people living with tremor while they eat. The next step of the development will be to test the new prototype with potential users. VL - 8 IS - 1 ER -
Science and Engineering Department, Mechanical Engineering, Laval University, Québec, Canada
Science and Engineering Department, Mechanical Engineering, Laval University, Québec, Canada
Interdisciplinary Center for Research in Rehabilitation and Social Integration, Québec, Canada
Science and Engineering Department, Mechanical Engineering, Laval University, Québec, Canada; Interdisciplinary Center for Research in Rehabilitation and Social Integration, Québec, Canada

Figure 1. Weighted spoon (https://www.caregiverproducts.com/good-grips-weighted-utensils-3.html).

Figure 2. Swivel spoon (https://www.caregiverproducts.com/swivel-spoon-with-built-up-handle.html).

Figure 3. Liftware Steady (https://store.liftware.com/products/liftware-starter-kit).
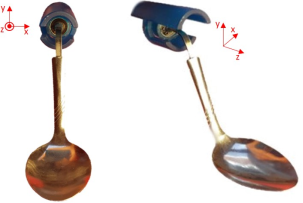

Figure 5. Four-bar mechanism spoon prototype.
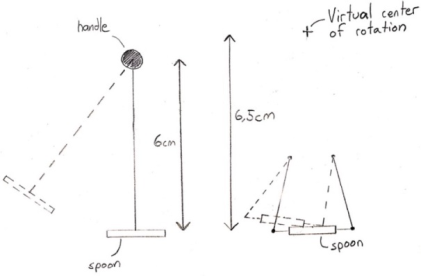
Figure 6. Swivel spoon trajectory (left) and four-bar mechanism trajectory (right).
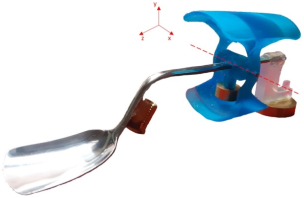
Figure 7. Balanced spoon prototype.

Figure 8. Balanced spoon prototype with 2 different handle orientations.
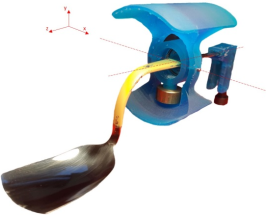
Figure 9. Swivel and balanced spoon prototype.
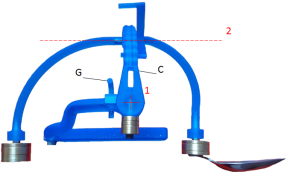
Figure 10. Side view of the final prototype.
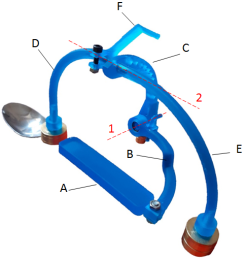
Figure 11. Isometric view of the final prototype.

Figure 12. Different positions of the spherical spoon prototype.
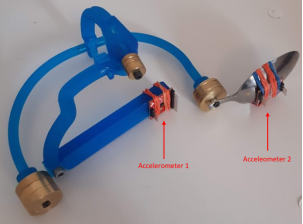
Figure 13. The accelerometers installed on the final spoon prototype.
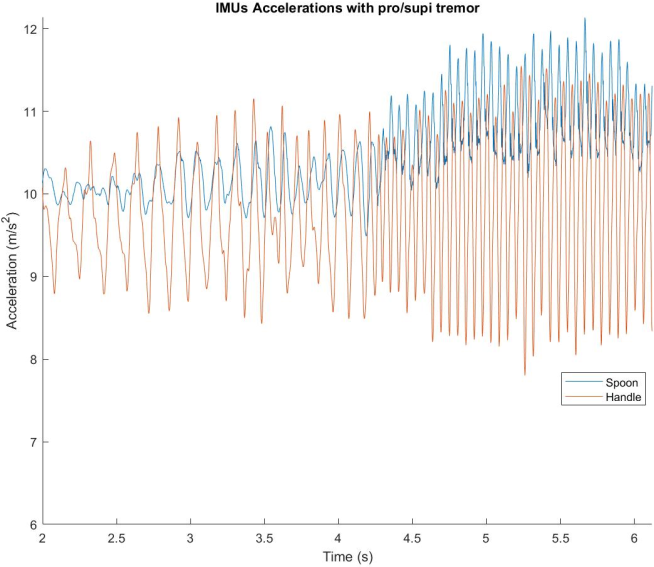
Figure 14. Graphic showing acceleration over time for the pro/supi tremor test.
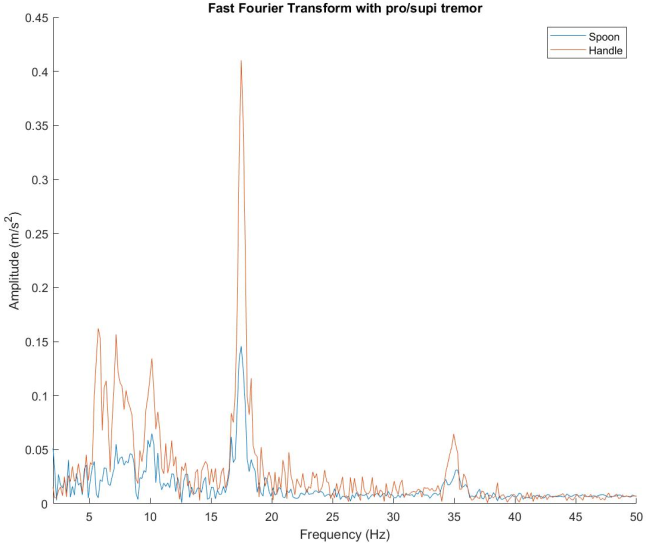
Figure 15. Graphic showing the Fast Fourier Transform of the pro/supi tremor test.
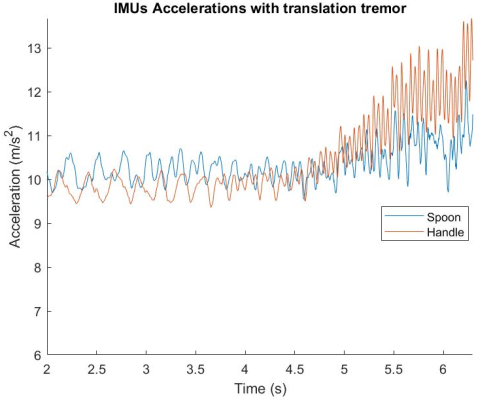
Figure 16. Graphic showing acceleration over time for the translation tremor test.
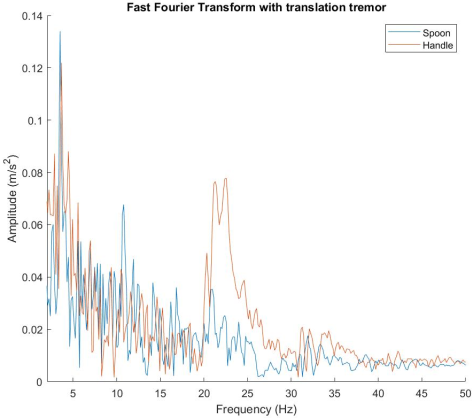
Figure 17. Graphic showing the Fast Fourier Transform of the translation tremor test.
Information

