Pediatric spontaneous biliary duct perforation (SBDP) represents a rare clinical condition. The vast majority of pediatric cases typically manifest around 6 months of age; however, the initial onset of this condition has been documented to occur as early as 25 weeks of gestation and, conversely, as late as 7 years postnatally. Despite the encouraging fact that the condition is treatable with appropriate intervention, the often non-specific nature of its associated symptoms and signs can unfortunately result in a significantly delayed diagnosis. This delay, in turn, carries the potential for the development of severe, life-threatening conditions such as biliary peritonitis and sepsis. Therefore, it is of paramount importance for clinicians to establish an early suspicion and achieve a prompt diagnosis to mitigate these risks. An exceptionally uncommon variant within the spectrum of spontaneous biliary duct perforation is the spontaneous rupture of the common hepatic duct. This report presents an illustrative case of a 5-month-old male infant who experienced a spontaneous perforation of the common hepatic duct, leading to the formation of a biloma. This diagnosis was successfully established pre-operatively through the utilization of a contrasted abdominal computed topography (CT) scan. Subsequently, the patient underwent a primary surgical repair of the identified perforation site, in addition to percutaneous drainage facilitated by a biliary T-tube. The postoperative recovery period was remarkably uneventful, and the T-tube was successfully removed on the 12th postoperative day. Six weeks following discharge from the hospital, the patient exhibited entirely satisfactory progress, with a complete absence of any discernible complications.
| Published in | American Journal of Pediatrics (Volume 11, Issue 3) |
| DOI | 10.11648/j.ajp.20251103.11 |
| Page(s) | 114-118 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Spontaneous Perforation of Common Hepatic Duct, Biloma, Pediatric Surgery
SBDP | Spontaneous Biliary Duct Perforation |
CT | Computed Topography |
ERCP | Endoscopic Retrograde Cholangiopancreatography |
Kg | Kilogram |
CBC | Complete Blood Count |
WBC | White Blood Cells |
LDH | Lactate Dehydrogenase |
MCV | Mean Corpuscular Volume |
ESR | Erythrocyte Sedimentation rate |
| [1] | Evans K, Marsden N, Desai A. Spontaneous perforation of the bile duct in infancy and childhood: a systematic review. J Pediatr Gastroenterol Nutr. (2010) 50: 677–81. |
| [2] | Yan X, Zheng N, Jia J, Kuang H, Lei H, Bian H, Qin X, Sun X, Duan X, Zhan J. Analysis of the Clinical Characteristics of Spontaneous Bile Duct Perforation in Children. Front Pediatr. 2022 Mar 23; 10: 799524. |
| [3] | Chardot C, Iskandarani F, De Dreuzy O, Duquesne B, Pariente D, Bernard O, Gauthier F, Valayer J. Spontaneous perforation of the biliary tract in infancy: a series of 11 cases. Eur J Pediatr Surg. 1996 Dec; 6(6): 341-6. |
| [4] | Tagiyev A, Tuna Kırsaçlıoğlu C, Demir E, et al. Rare cause of ascites and jaundice in infancy: Spontaneous bile duct perforation. J Paediatr Child Health. 2022; 58(9): 1669-1671. |
| [5] | Workye Tigabie, Goytom Knfe Tesfay, Yeneneh Yirga, Spontaneous perforation of the cystic duct in an infant, Journal of Pediatric Surgery Case Reports, Volume 77, 2022, |
| [6] | Mishra, Purbasha; Sahoo, Tanushree; Som, Tapas Kumar; Sahoo, Subrat Kumar. Biliary Perforation in a Neonate – A Rare Cause of Infantile Cholestasis. Journal of Indian Association of Pediatric Surgeons 29(4): p 393-394, Jul–Aug 2024. |
| [7] | Naghi Dara, Hamed Ebrahimibagha, Amirali Soheili, Zhale Nahavandi, Leily Mohajerzadeh, Amirhossein Hosseini, Mohsen Rouzrokh, Spontaneous bile duct perforation in late infancy, Journal of Pediatric Surgery Case Reports, Volume 93, 2023, 102610, ISSN 2213-5766. |
| [8] | Sunil K, Gupta A, Verma AK, Singh AK, Kureel SN, Pandey A. Spontaneous common hepatic duct perforation in a child: A rare case report. Afr J Paediatr Surg. 2018 Jan-Mar; 15(1): 53-55. |
| [9] | Pattanaik P, Pattanaik SK. Spontaneous perforation of the common hepatic duct in a child: an unexpected intraoperative encounter. BMJ Case Rep. 2024; 17(7): e261041. Published 2024 Jul 16. |
| [10] | Kasat LS, Borwankar SS, Jain M, Naregal A. Spontaneous perforation of the extrahepatic bile duct in an infant. Pediatr Surg Int. (2001) 17: 463–4. |
| [11] | Barnes BH, Narkewicz MR, Sokol RJ. Spontaneous perforation of the bile duct in a toddler: the role of endoscopic retrograde cholangiopancreatography in diagnosis and therapy. J Pediatr Gastroenterol Nutr. 2006; 43(5): 695-697. |
| [12] | Malik HS, Cheema HA, Fayyaz Z, Hashmi MA, Parkash A, Waheed N, Mushtaq I, Anjum N. Spontaneous Perforation Of Bile Duct, Clinical Presentation, Laboratory Work Up, Treatment And Outcome. J Ayub Med Coll Abbottabad. 2016 Jul-Sep; 28(3): 518-522. |
| [13] | Gupta, Tarun; Mandelia, Ankur; Yadav, Rajanikant R.; Kumar, Tarun; Agarwal, Nishant; Kanneganti, Pujana; Verma, Anju; Nair, Biju; Buan, Amit. Laparoscopic Management of a Rare Case of Spontaneous Biliary Perforation in an Infant. Journal of Indian Association of Pediatric Surgeons 29(6): p 640-643, Nov–Dec 2024. |
| [14] | Freeland, J. (1882) Rupture of the hepatic duct. Lancet, 1, 731-732. |
| [15] | Dijkstra CH. Graluistorting in de buikholte bij een zuigeling. Maandschr Kindergeneeskd. 1932; 1: 409-14. |
APA Style
Herzallah, R., Al-Rahamneh, S., Altarawneh, Q., Abuqubu, S. (2025). Spontaneous Rupture of Common Hepatic Duct in an Infant, a Rare Entity. American Journal of Pediatrics, 11(3), 114-118. https://doi.org/10.11648/j.ajp.20251103.11
ACS Style
Herzallah, R.; Al-Rahamneh, S.; Altarawneh, Q.; Abuqubu, S. Spontaneous Rupture of Common Hepatic Duct in an Infant, a Rare Entity. Am. J. Pediatr. 2025, 11(3), 114-118. doi: 10.11648/j.ajp.20251103.11
@article{10.11648/j.ajp.20251103.11,
author = {Ranya Herzallah and Samer Al-Rahamneh and Qusay Altarawneh and Sarah Abuqubu},
title = {Spontaneous Rupture of Common Hepatic Duct in an Infant, a Rare Entity
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {3},
pages = {114-118},
doi = {10.11648/j.ajp.20251103.11},
url = {https://doi.org/10.11648/j.ajp.20251103.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251103.11},
abstract = {Pediatric spontaneous biliary duct perforation (SBDP) represents a rare clinical condition. The vast majority of pediatric cases typically manifest around 6 months of age; however, the initial onset of this condition has been documented to occur as early as 25 weeks of gestation and, conversely, as late as 7 years postnatally. Despite the encouraging fact that the condition is treatable with appropriate intervention, the often non-specific nature of its associated symptoms and signs can unfortunately result in a significantly delayed diagnosis. This delay, in turn, carries the potential for the development of severe, life-threatening conditions such as biliary peritonitis and sepsis. Therefore, it is of paramount importance for clinicians to establish an early suspicion and achieve a prompt diagnosis to mitigate these risks. An exceptionally uncommon variant within the spectrum of spontaneous biliary duct perforation is the spontaneous rupture of the common hepatic duct. This report presents an illustrative case of a 5-month-old male infant who experienced a spontaneous perforation of the common hepatic duct, leading to the formation of a biloma. This diagnosis was successfully established pre-operatively through the utilization of a contrasted abdominal computed topography (CT) scan. Subsequently, the patient underwent a primary surgical repair of the identified perforation site, in addition to percutaneous drainage facilitated by a biliary T-tube. The postoperative recovery period was remarkably uneventful, and the T-tube was successfully removed on the 12th postoperative day. Six weeks following discharge from the hospital, the patient exhibited entirely satisfactory progress, with a complete absence of any discernible complications.
},
year = {2025}
}
TY - JOUR T1 - Spontaneous Rupture of Common Hepatic Duct in an Infant, a Rare Entity AU - Ranya Herzallah AU - Samer Al-Rahamneh AU - Qusay Altarawneh AU - Sarah Abuqubu Y1 - 2025/06/23 PY - 2025 N1 - https://doi.org/10.11648/j.ajp.20251103.11 DO - 10.11648/j.ajp.20251103.11 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 114 EP - 118 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20251103.11 AB - Pediatric spontaneous biliary duct perforation (SBDP) represents a rare clinical condition. The vast majority of pediatric cases typically manifest around 6 months of age; however, the initial onset of this condition has been documented to occur as early as 25 weeks of gestation and, conversely, as late as 7 years postnatally. Despite the encouraging fact that the condition is treatable with appropriate intervention, the often non-specific nature of its associated symptoms and signs can unfortunately result in a significantly delayed diagnosis. This delay, in turn, carries the potential for the development of severe, life-threatening conditions such as biliary peritonitis and sepsis. Therefore, it is of paramount importance for clinicians to establish an early suspicion and achieve a prompt diagnosis to mitigate these risks. An exceptionally uncommon variant within the spectrum of spontaneous biliary duct perforation is the spontaneous rupture of the common hepatic duct. This report presents an illustrative case of a 5-month-old male infant who experienced a spontaneous perforation of the common hepatic duct, leading to the formation of a biloma. This diagnosis was successfully established pre-operatively through the utilization of a contrasted abdominal computed topography (CT) scan. Subsequently, the patient underwent a primary surgical repair of the identified perforation site, in addition to percutaneous drainage facilitated by a biliary T-tube. The postoperative recovery period was remarkably uneventful, and the T-tube was successfully removed on the 12th postoperative day. Six weeks following discharge from the hospital, the patient exhibited entirely satisfactory progress, with a complete absence of any discernible complications. VL - 11 IS - 3 ER -
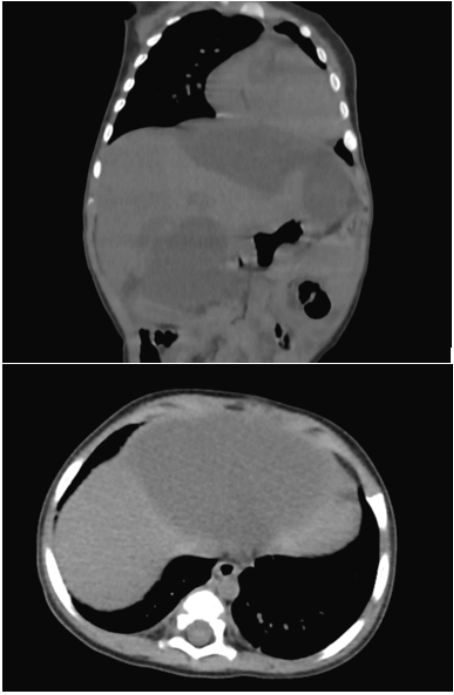
Figure 1. A large subhepatic encysted fluid collection and a multiseptated collection in the gallbladder region.

Figure 2. Biliary drainage from the percutaneous drain.
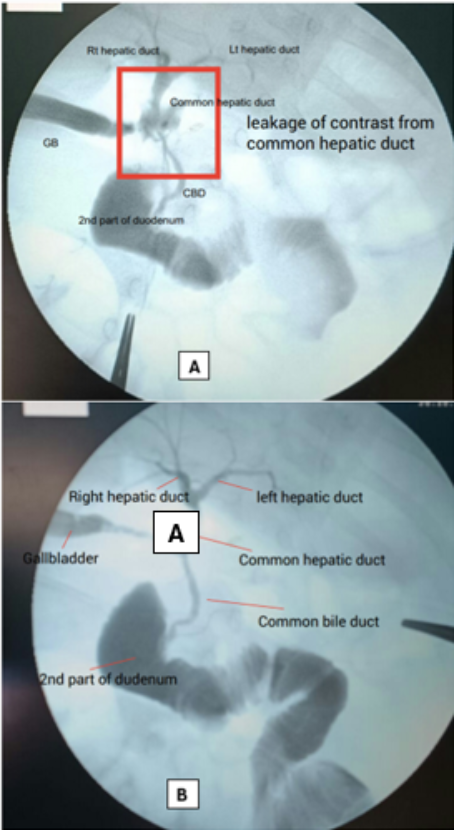
Figure 3. Intraoperative cholangiogram. A: Contrast leakage from the common hepatic duct. B: Repeat intraoperative cholangiogram showed no contrast leakage from the previous site.
Information

