Abstract
The aim of this study is to evaluate the contribution of neuromeningeal multiplex PCR in the diagnosis of infectious meningitis within a pediatric hospital population. The secondary objective is to compare the diagnostic performance of this technique compared with conventional methods in order to optimize the utilization of multiplex PCR. This work is a retrospective study of 112 children (1 month–17 years) investigated for suspected meningitis between 2020 and 2025. CSF samples were analyzed using conventional methods and the multiplex PCR panel, with demographic and biological data reviewed. The study included 67 boys (60%) and 45 girls (40%) (male-to-female ratio 1.49), with a mean age of 6.67 years; children aged 3–5 years were the most represented. Laboratory activity increased over time, reaching 37 multiplex PCR analyses in 2024–2025. Multiplex PCR was positive in 18 patients (16%). Viruses accounted for 85% of pathogens, mainly Enteroviruses (65%), followed by HHV-6 (29%) and HSV-2 (6%). Three bacterial cases and two co-infections (11.1%) were identified. Most patients had normal CSF cytology (71%); among PCR-positive cases, 33% showed elevated CSF protein, with normal glucose in all samples. CRP levels were elevated to very high in 55.6% of cases. In conclusion; the integration of multiplex PCR as a first-line test in symptomatic children, regardless of CSF parameters, appears justified. It allows for the optimization of the care pathway through a reduction in hospitalization duration and unnecessary treatments.
|
Published in
|
American Journal of Pediatrics (Volume 12, Issue 1)
|
|
DOI
|
10.11648/j.ajp.20261201.16
|
|
Page(s)
|
39-47 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Children, Multiplex PCR, Filmarray, Meningitis
1. Introduction
Infectious meningitis constitutes a diagnostic, therapeutic, and sometimes prophylactic emergency requiring rapid management to limit morbidity, mortality, and neurological complications.
In children, despite significant advancements in modern medicine, this infection remains one of the pathologies most feared by the medical community. Crucially, it is often difficult to suspect based solely on clinical signs, which are frequently misleading
.
Historically, definitive diagnosis relied on cerebrospinal fluid (CSF) culture, a traditional yet inherently slow technique requiring 24 to 48 hours—or even longer—to identify the pathogen and provide antimicrobial susceptibility testing
| [2] | Meningitis (Bacterial) and Meningococcal Disease: Recognition, Diagnosis and Management [D1] Evidence Reviews for Antibiotics for Bacterial Meningitis before or in the Absence of Identifying Causative Infecting Organism in Younger Infants. 2024. |
[2]
.
This "diagnostic gap" compelled pediatricians to hospitalize and overtreat many children, generating considerable human and economic costs, as well as unnecessary antibiotic selection pressure
| [2] | Meningitis (Bacterial) and Meningococcal Disease: Recognition, Diagnosis and Management [D1] Evidence Reviews for Antibiotics for Bacterial Meningitis before or in the Absence of Identifying Causative Infecting Organism in Younger Infants. 2024. |
[2]
.
The advent of molecular biology techniques, and specifically syndromic multiplex Polymerase chain reaction (PCR), has shifted this paradigm by promising comprehensive identification of the main etiological agents in less than one hour, increasing significantly diagnostic yield compared with culture and microscopy, with reported sensitivities around 90–95% and specificities often above 90%
| [3] | Hueth KD, Thompson-Leduc P, Totev TI, et al. Assessment of the Impact of a Meningitis/Encephalitis Panel on Hospital Length of Stay: A Systematic Review and Meta-Analysis. Antibiotics. MDPI. 2022; 11(8).
https://doi.org/10.3390/antibiotics11081028 |
| [4] | Biswal, D., Gautam, H., Kumar, V., Tyagi, S., Kumar, Y., Mohapatra, S., Sood, S., Dhawan, B., & Das, B. (2025). Utility of Multiplex PCR for Rapid Diagnosis of Acute Bacterial Meningitis: A North Indian Tertiary Care Experience.. Indian journal of medical microbiology, 100915.
https://doi.org/10.1016/j.ijmmb.2025.100915. |
| [5] | Sharma, N., Gautam, H., Tyagi, S., Raza, S., Mohapatra, S., Sood, S., Dhawan, B., Kapil, A., & Das, B. (2022). Clinical use of multiplex-PCR for the diagnosis of acute bacterial meningitis. Journal of Family Medicine and Primary Care, 11, 593 - 598. https://doi.org/10.4103/jfmpc.jfmpc_1162_21 |
[3-5]
.
Beyond improving pathogen detection, multiplex PCR also helps distinguish bacterial from viral meningitis, thereby supporting early decisions on initiating, narrowing, or discontinuing antimicrobial therapy and potentially reducing hospital stay and unnecessary antibiotic exposure
| [6] | Naeem, A., Murtaza, M., Ayub, M., Bhatti, S., Khan, F., & Ayub, M. (2025). DIAGNOSTIC VALUE OF MULTIPLEX PCR IN DIFFERENTIATING BACTERIAL VS VIRAL MENINGITIS. Insights-Journal of Life and Social Sciences. https://doi.org/10.71000/1fwnpg52 |
| [7] | Ahmed, M., Askar, G., Farghaly, H., Ahmed, A., Kamal, D., Ahmed, S., & Mohamad, I. (2022). Evaluation of the accuracy of multiplex polymerase chain reaction in differentiation between bacterial and viral meningitis. Irish Journal of Medical Science, 192, 403 - 407.
https://doi.org/10.1007/s11845-022-02983-2 |
[6, 7]
.
Consequently, multiplex PCR is now considered an important complementary assay to conventional microbiological techniques, with the potential to reshape diagnostic algorithms for meningitis in both high and low resource settings
| [4] | Biswal, D., Gautam, H., Kumar, V., Tyagi, S., Kumar, Y., Mohapatra, S., Sood, S., Dhawan, B., & Das, B. (2025). Utility of Multiplex PCR for Rapid Diagnosis of Acute Bacterial Meningitis: A North Indian Tertiary Care Experience.. Indian journal of medical microbiology, 100915.
https://doi.org/10.1016/j.ijmmb.2025.100915. |
| [6] | Naeem, A., Murtaza, M., Ayub, M., Bhatti, S., Khan, F., & Ayub, M. (2025). DIAGNOSTIC VALUE OF MULTIPLEX PCR IN DIFFERENTIATING BACTERIAL VS VIRAL MENINGITIS. Insights-Journal of Life and Social Sciences. https://doi.org/10.71000/1fwnpg52 |
[4, 6]
.
The aim of this study is to evaluate the diagnostic contribution of neuromeningeal multiplex PCR in the diagnosis of infectious meningitis within a pediatric hospital population. The secondary objective is to compare the diagnostic performance of this technique compared with conventional methods in order to optimize the utilization of multiplex PCR.
2. Materials and Methods
This retrospective, descriptive, and analytical study was conducted over a five-year period, from September 2020 to September 2025, at the Virology Laboratory of the Mohammed V Military Teaching Hospital in Rabat (HMIMV).
The study population consisted of pediatric patients admitted for suspected meningitis who underwent a lumbar puncture. CSF samples were transported to the laboratories for cytobacteriological, biochemical, and molecular analysis using multiplex PCR (BioFire® FilmArray® Meningitis/Encephalitis).
We excluded patients who are not hospitalized in the pediatric ward, as well as examinations performed for control purposes or therapeutic monitoring. Data collection for the included patients was extracted from the Laboratory Information System (LIS). Data entry and management were performed using the Microsoft Excel spreadsheet (Version 2025). All statistical analyses were subsequently conducted using jamovi software (Version 2.6.44.0).
Our study has certain methodological limitations that must be acknowledged. First, its retrospective design makes it susceptible to inherent selection bias and missing data. Second, this is a single-center study, which may limit the external validity and generalizability of our findings to other populations. Therefore, large-scale, prospective, multicenter studies are required to validate our conclusions.
3. Results
The study included a cohort of 112 pediatric patients over a 5-year period. Demographic analysis revealed a male predominance, with 67 boys (60%) and 45 girls (40%), corresponding to a male-to-female sex ratio of 1.49. Patient ages ranged from 1 month to 17 years, with a mean age of 6.67 years. The preschool age group (3 to 5 years) was the most represented. Temporally, a progressive increase in the volume of processed samples was observed, peaking at 37 analyses performed during the 2024–2025 period (
Table 1).
Table 1. Demographic and Epidemiological Profile of the Study Serie.
Variable | Levels | Frequencies | % of total | Cumulative% |
Sex | F | 45 | 40,2 | 40,2 |
M | 67 | 59,8 | 100 |
Age | 0-2 | 17 | 15,2 | 15,2 |
3-5 | 38 | 33,9 | 49,1 |
6-8 | 21 | 18,8 | 67,9 |
9-11 | 16 | 14,3 | 82,1 |
12-14 | 11 | 9,8 | 92,0 |
15-17 | 9 | 8,0 | 100,0 |
Year | 2020-2021 | 5 | 4,5 | 4,5 |
2021-2022 | 25 | 22,3 | 26,8 |
2022-2023 | 27 | 24,1 | 50,9 |
2023-2024 | 18 | 16,1 | 67,0 |
2024-2025 | 37 | 33,0 | 100,0 |
CSF cytologic analysis showed pleocytosis (elevated white blood cells) in only 29% of patients (n=33), while the majority (71%) presented normal cytology. Importantly, conventional bacteriological culture proved sterile for all 112 samples (100%).
In children, normal CSF values are defined as 0.5–0.6 g/L for glucose (glycorrhachia) and 0.15–0.45 g/L for protein (proteinorrhachia); most of the patients (n=82) presented with normal protein levels, whereas 78 patients presented with hypoglycorrhachia.
Regarding blood inflammatory markers, leucocytosis was observed in 33.9% of patients, while leukocyte counts remained within normal limits in 56.3%. The mean C-reactive protein (CRP) level was 47.7 mg/L, with 45.5% of patients (n = 51) showing CRP values > 20 mg/L (high or very high categories).
CSF analysis using multiplex PCR identified a pathogen in 18 samples, corresponding to an overall positivity rate of 16%. Three samples were excluded due to technical non-conformity. Viruses accounted for 85% of detected pathogens (n = 17), whereas bacteria represented 15% (n = 3). No fungal infections were identified in our paediatric population.
Among detected viruses, enteroviruses accounted for 65% (n = 11), followed by Human Herpesvirus 6 (HHV-6) (29%, n = 5) and HSV-2 (6%, n = 1). Haemophilus influenzae, Neisseria meningitidis, and Escherichia coli K1 were the three bacterial species detected, each in one sample. Two cases of co-infection (11.1% of positive samples) were observed: one involving N. meningitidis + enterovirus, and another involving enterovirus + HHV-6.
The study of concordance between standard biology and multiplex PCR revealed normal CSF cytology in 55.5% (10/18) of PCR-positive samples.
CSF biochemical parameters, specifically protein and glucose levels, were conserved (normal) in 67% (12/18) and 100% of cases, respectively. CRP was strictly normal (< 5 mg/L) in 27.8% of patients with a positive PCR. Enterovirus infections were associated with a moderate mean CRP of 36.7 mg/L.
4. Discussion
Our pediatric population was characterized by a male predominance (60%, M/F sex ratio: 1.49). This finding corroborates a quasi-universal trend reported in the literature regarding pediatric meningitis investigated via multiplex PCR.
As summarized in
Table 2, similar ratios have been observed in Turkey (1.82) and Chile (1.41). The median age in our series was 6 years, with a predominance of the 3–5 years age group, which aligns closely with data from Vietnam (median: 5 years) and Chile (median: 4 years).
Table 2.
Comparison of demographic characteristics (Sex Ratio and Age) of pediatric meningitis cohorts using syndromic testing | [8] | Goktug A, Gundogdu IA, Duyu M, Besli E. Clinical Impact of Cerebrospinal Fluid Multiplex Polymerase Chain Reaction (PCR) Testing in Children with Suspected Central Nervous System Infection. Medeni Med J. 2025; 40(3): 128-135.
https://doi.org/10.4274/MMJ.galenos.2025.43895 |
| [11] | Aldriweesh MA, Shafaay EA, Alwatban SM, et al. Viruses Causing Aseptic Meningitis: A Tertiary Medical Center Experience With a Multiplex PCR Assay. Front Neurol. 2020; 11. https://doi.org/10.3389/fneur.2020.602267 |
Study | Sample size | Sex ratio M/F | Median age (years) |
Our series | 112 | 1,49 | 6 |
Turkey8 | 114 | 1,82 | 2,7 |
Chile9 | 84 | 1,41 | 4 |
Vietnam10 | 99 | - | 5 |
saudi arabia11 | 240 | 1,2 | - |
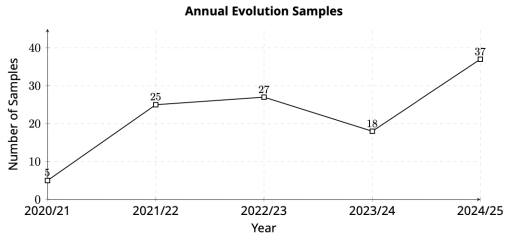
Temporal analysis reveals a significant increase in testing volume, rising from 5 tests in 2020/2021 to 37 tests in 2024/2025. This growth curve (
Figure 1) illustrates the progressive clinical adoption of the Meningitis/Encephalitis (ME) panel within our institution. This implementation phase mirrors data from the literature, notably the study by Messacar et al., which associates panel adoption with diagnostic time savings. Although our absolute volume remains lower than that of major Asian centers, the growth dynamic testifies to its successful integration into the patient care pathway
| [12] | Messacar K, Breazeale G, Robinson CC, Dominguez SR. Potential clinical impact of the film array meningitis encephalitis panel in children with suspected central nervous system infections. Diagn Microbiol Infect Dis. 2016; 86(1): 118-120.
https://doi.org/10.1016/j.diagmicrobio.2016.05.020 |
[12]
.
Figure 1. Annual Evolution of Multiplex PCR Requests at the HMIMV Virology Laboratory (2020–2025).
The overall positivity rate of 16% places our study in an intermediate position compared to large North American cohorts (8.7%) and Asian (36.8%) or South American series (40%). This disparity does not reflect a difference in analytical sensitivity but is rather attributable to the high rates reported in Asia and Brazil, which are often correlated with significant circulation of arboviruses or neurotropic enteroviruses (
Table 3).
Table 3.
Comparative diagnostic yield and co-detection rates of the FilmArray ME panel across diverse geographical settings | [13] | Du B, Hua C, Xia Y, et al. Evaluation of the BioFire FilmArray meningitis/encephalitis panel for the detection of bacteria and yeast in Chinese children. Ann Transl Med. 2019; 7(18): 437-437. https://doi.org/10.21037/atm.2019.08.103 |
| [14] | Rasti R, Kumbakumba E, Nanjebe D, et al. Clinical utility of the FilmArray® meningitis/encephalitis panel in children with suspected central nervous system infection in a low-resource setting - a prospective study in Southwestern Uganda. BMC Infect Dis. 2025; 25(1).
https://doi.org/10.1186/s12879-025-10732-w |
| [15] | Leber AL, Everhart K, Balada-Llasat JM, et al. Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. 2016; 54(9): 2251-2261.
https://doi.org/10.1128/JCM.00730-16 |
| [16] | Domingues RB, Santos MV dos, Leite FBV de M, Senne C. FilmArray Meningitis/Encephalitis (ME) panel in the diagnosis of bacterial meningitis. Brazilian Journal of Infectious Diseases. 2019; 23(6): 468-470.
https://doi.org/10.1016/j.bjid.2019.10.008 |
Study | Sample size | Positivity rate | Co-infection rate |
Our series | 112 | 16% | 11% |
China13 | 68 | 36,8% | - |
Uganda14 | 194 | 20,62% | 18% |
USA15 | 1560 | 8,7% | - |
Beazil16 | 436 | 40% | - |
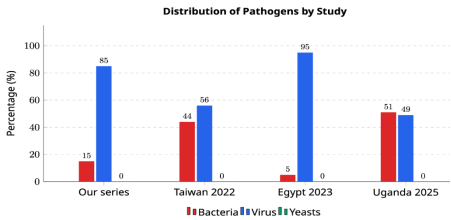
The major contribution of multiplex PCR is the confirmation of the paradigm shift in pediatric meningitis. With 85% viral etiologies versus 15% bacterial (
Figure 2), our study aligns with the international consensus (Taiwan, Egypt)
| [17] | Hara M, Ishihara M, Nakajima H. Use of the FilmArray® Meningitis/Encephalitis panel to detect pathogenic microorganisms in cerebrospinal fluid specimens: a single-center retrospective study. Journal of International Medical Research. 2022; 50(10). https://doi.org/10.1177/03000605221129561 |
| [18] | Zakariya Mohammed M, Ramadan M, Abdelhalim M, Elarab HE, Wahab Garrad A. The Results of Meningitis/Encephalitis Panel in Children with Suspected Central Nervous System Infections. Vol 90. 2023. |
[17, 18]
.
The low bacterial prevalence (
N. meningitidis,
H. influenzae,
E. coli K1 detected sporadically) must not be interpreted as a limitation of the panel, but rather as a reflection of vaccine efficacy (
H. influenzae B, Pneumococcus) and early antibiotic use. Here, PCR retains critical added value: the detection of "residual" yet invasive bacteria, often rendered culture-negative by antibiotic therapy and undetected by bacteriological culture, as highlighted by Messacar et al
| [12] | Messacar K, Breazeale G, Robinson CC, Dominguez SR. Potential clinical impact of the film array meningitis encephalitis panel in children with suspected central nervous system infections. Diagn Microbiol Infect Dis. 2016; 86(1): 118-120.
https://doi.org/10.1016/j.diagmicrobio.2016.05.020 |
[12]
.
Figure 2. Distribution of Pathogens Identified in Various Pediatric Studies Using Neuromeningeal Multiplex PCR.
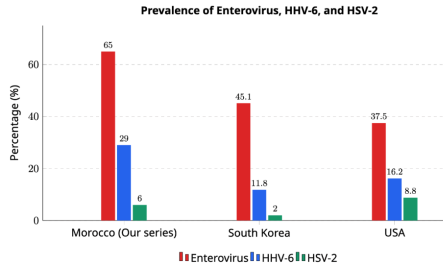
In contrast to Enteroviruses, where causality is rarely ambiguous, the detection of HHV-6 (29% of viral findings)—often co-detected with other agents—requires differentiating between an active infection (primary infection), viral reactivation, or chromosomally integrated HHV-6 (ci-HHV-6), which occurs in approximately 1% of the population (
Figure 3). Consequently, the syndromic approach demands, more than ever, rigorous correlation with clinical presentation and standard biological markers (CSF cytology).
4.1. Contribution of Multiplex PCR Compared to Conventional Examinations
The analysis of concordance between molecular detection and conventional biological parameters reveals a frequent dissociation, calling into question the reliability of screening algorithms based solely on cytology or systemic inflammation.
A major finding of our series is the high proportion of "biologically normal" CSF samples among PCR-positive cases. With 55.5% presenting normal cytology and 67% showing physiological protein levels among infected patients, our results confirm the frequent existence of viral meningitis that is paucisymptomatic from a biological standpoint.
This "cyto-molecular dissociation" aligns with data from Kim et al. (30% normal CSF) and Cresswell et al. (33%), highlighting that the absence of pleocytosis does not exclude an active infection, particularly with Enterovirus or HHV-6
| [19] | Park SE, Lim TJ, Nam SO, et al. Clinical utility of the FilmArray meningitis/encephalitis panel in children at a tertiary center in South Korea. Brain Dev. 2021; 43(2): 234-243.
https://doi.org/10.1016/j.braindev.2020.08.010 |
| [20] | Bridge S, Hullsiek KH, Nerima C, et al. Evaluation of the BioFire® FilmArray® Meningitis/Encephalitis panel in an adult and pediatric Ugandan population. Journal of Medical Mycology. 2021; 31(3). https://doi.org/10.1016/j.mycmed.2021.101170 |
[19, 20]
.
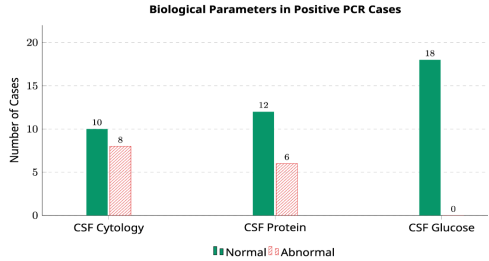
As illustrated in
Figure 4, the absence of hypoglycorrhachia (100% of cases) and the rarity of hyperproteinorrhachia delineate a "silent" biochemical profile typical of viral etiologies, contrasting with the inflammatory cascade of bacterial meningitis. This observation validates the strategy of not conditioning the performance of the ME panel on the presence of pleocytosis, as doing so would result in missing more than half of viral diagnoses.
Figure 4. Comparison of Biological Profiles of Multiplex PCR-Positive CSF Samples.
The analysis of systemic markers (Leukocytes, CRP) demonstrates their inability to discriminate patients requiring molecular investigation; notably, over half (56.3%) of patients with PCR-positive CSF presented with normal leukocyte counts. This result consolidates the conclusions of Messacar et al. and Precit et al., establishing that the peripheral leukocytic response is a poor indicator of neuromeningeal infection, particularly of viral origin
| [12] | Messacar K, Breazeale G, Robinson CC, Dominguez SR. Potential clinical impact of the film array meningitis encephalitis panel in children with suspected central nervous system infections. Diagn Microbiol Infect Dis. 2016; 86(1): 118-120.
https://doi.org/10.1016/j.diagmicrobio.2016.05.020 |
| [21] | Precit MR, Yee R, Pandey U, et al. Cerebrospinal fluid findings are poor predictors of appropriate filmarray meningitis/encephalitis panel utilization in pediatric patients. J Clin Microbiol. 2020; 58(3). https://doi.org/10.1128/JCM.01592-19 |
[12, 21]
.
Regarding CRP, the heterogeneity of values (27.8% normal, 50% elevated) highlights the absence of a linear correlation. Although bacterial infections are classically associated with elevated CRP (>50 mg/L), our data and that of Leber et al. confirm that low or normal CRP does not possess sufficient negative predictive value (NPV) to rule out viral Central nervous system involvement
| [15] | Leber AL, Everhart K, Balada-Llasat JM, et al. Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. 2016; 54(9): 2251-2261.
https://doi.org/10.1128/JCM.00730-16 |
[15]
.
The discordance observed in our study between multiplex PCR positivity and the normality of conventional biological markers mandates a re-evaluation of triage strategies. The fact that 55% of molecularly confirmed infections (primarily viral) present with strictly normal cytology, and that nearly 30% progress without significant biological inflammatory syndrome, highlights a major "diagnostic gap".
In summary, neither CSF cyto-biochemical analysis nor the absence of a biological inflammatory syndrome constitutes an exclusion criterion for infectious meningitis in pediatrics.
In practice, the absence of a cellular reaction in the CSF or a systemic inflammatory response should not be considered an exclusion criterion (insufficient NPV) for meningoencephalitis, particularly of viral origin. This finding reinforces the positioning of neuromeningeal multiplex PCR as a first-line test in the diagnostic workup for suspected meningoencephalitis in pediatrics.
4.2. Rationalization of Antibiotic and Antiviral Therapy in Pediatrics
The analysis of our series reveals that 85% of identified etiologies were viral, offering a major lever for a key tool for reducing unnecessary antibiotic use. The critical contribution of the syndromic panel lies in its high NPV for the targeted bacteria, theoretically permitting rapid therapeutic de-escalation.
Messacar et al. were the first to demonstrate that the implementation of the ME panel significantly reduces the duration of empirical antibiotic therapy, decreasing from over 48 hours (pending culture results) to less than 24 hours in tested patients
| [12] | Messacar K, Breazeale G, Robinson CC, Dominguez SR. Potential clinical impact of the film array meningitis encephalitis panel in children with suspected central nervous system infections. Diagn Microbiol Infect Dis. 2016; 86(1): 118-120.
https://doi.org/10.1016/j.diagmicrobio.2016.05.020 |
[12]
.
In our context, which is comparable to that described by Cresswell et al. in Uganda where the majority of children receive antibiotics even before lumbar puncture, multiplex PCR offers the opportunity to discontinue these unnecessary treatments within the very first hour.
However, the real-world impact depends on the clinician's confidence in the result. As highlighted by Rasti et al., maintaining antibiotics despite a negative PCR and sterile culture remains a common practice ("fear of missing out"), which can only be corrected by a strict antimicrobial stewardship protocol
| [14] | Rasti R, Kumbakumba E, Nanjebe D, et al. Clinical utility of the FilmArray® meningitis/encephalitis panel in children with suspected central nervous system infection in a low-resource setting - a prospective study in Southwestern Uganda. BMC Infect Dis. 2025; 25(1).
https://doi.org/10.1186/s12879-025-10732-w |
[14]
.
The detection of HSV-2 in 6% of positive cases, and the complete absence of HSV-1 and VZV, contrast with the often-systematic use of empiric acyclovir.
The utilization of the ME panel as a safe "Stop rule" for acyclovir is now well documented. A recent multicenter study showed that rapid result reporting allowed for a mean reduction of 29 to 39 hours in the duration of acyclovir treatment for HSV-negative patients
| [15] | Leber AL, Everhart K, Balada-Llasat JM, et al. Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. 2016; 54(9): 2251-2261.
https://doi.org/10.1128/JCM.00730-16 |
[15]
.
For our patients (94% of the cohort were HSV-negative), the PCR result obtained in 1 hour avoids potential nephrotoxicity and the cost of unnecessary antiviral treatment, validating the approach described by Leber et al
| [15] | Leber AL, Everhart K, Balada-Llasat JM, et al. Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. 2016; 54(9): 2251-2261.
https://doi.org/10.1128/JCM.00730-16 |
[15]
.
4.3. Reduction of Hospitalization Duration
The predominance of Enteroviruses (65% of detected viruses) in our series suggests a direct benefit on bed turnover. The rapid positive diagnosis of Enteroviral meningitis classically allows for early discharge once the clinical status has stabilized, without awaiting the normalization of biological parameters. Comparative data show that patients benefiting from rapid molecular diagnosis have a significantly reduced Length of Stay (LOS). Duff et al. report a decrease of 0.5 to 2 days for viral meningitis diagnosed by multiplex PCR compared to conventional methods
| [22] | Duff S, Hasbun R, Balada-Llasat JM, Zimmer L, Bozzette SamuelA, Ginocchio CC. Economic analysis of rapid multiplex polymerase chain reaction testing for meningitis/encephalitis in adult patients. Infection. 2019; 47(6): 945-953.
https://doi.org/10.1007/s15010-019-01320-7 |
[22]
.
5. Conclusion
This study aligns with the objective of improving the early diagnosis of infectious meningitis in children. Our results objectively demonstrate an ecology dominated at 85% by viral etiologies (primarily Enterovirus and HHV-6), relegating invasive bacteria to the background (15%), likely due to the combined effect of vaccine coverage and pre-hospital antibiotic therapy.
The major contribution of this work lies in the identification of a significant "diagnostic gap": 55.5% of molecularly confirmed infections presented with strictly normal cytology, and a substantial proportion progressed without a frank biological inflammatory syndrome. This clinico-biological dissociation invalidates restrictive triage strategies based on pleocytosis or CRP, which expose clinicians to the risk of missing more than half of viral meningitis cases.
Therapeutically, the high NPV of the panel offers a safe opportunity for antimicrobial de-escalation. The speed of result reporting (1 hour) constitutes a decisive lever for rationalizing empiric antibiotic therapy and the early discontinuation of acyclovir, thus responding to current Antimicrobial Stewardship imperatives.
In conclusion, the integration of syndromic diagnosis as a first-line test in symptomatic children, regardless of CSF parameters, appears justified. It allows not only for the refinement of local epidemiology but, above all, for the optimization of the care pathway through a reduction in hospitalization duration and unnecessary treatments.
Abbreviations
CSF | Cerebrospinal Fluid |
PCR | Polymerase Chain Reaction |
LIS | Laboratory Information System |
CRP | C-reactive Protein |
HHV-6 | Human Herpesvirus 6 |
ME | Meningitis/Encephalitis |
HMIMV | Mohammed V Military Teaching Hospital |
NPV | Negative Predictive Value |
LOS | Length of Stay |
Author Contributions
Anouar Akhssas: Conceptualization, Investigation, Visualization, Writing – original draft, Writing – review & editing
Rachid Abi: Writing – review & editing, Supervision, Validation
Qamar Zaza: Conceptualization, Investigation, Visualization, Validation
Fadwa Bouhajban: Conceptualization, Investigation, Visualization, Validation
Kawtar Qadiri: Conceptualization, Investigation, Visualization, Validation
Souhail Bibih: Conceptualization, Investigation, Visualization, Validation
Oumayma Elbouni: Conceptualization, Investigation, Visualization, Validation
Soukaina Akradi: Conceptualization, Investigation, Visualization, Validation
Fatima Zahra Lyaagoubi: Conceptualization, Investigation, Visualization, Validation
Chaimaa Nouibi: Conceptualization, Investigation, Visualization, Validation
Safae Elkochri: Project Administration, Validation
Younes Aouni: Conceptualization, Investigation, Visualization, Validation
Fadwa Elamraoui: Conceptualization, Investigation, Visualization, Validation
Yousra Elhabti: Conceptualization, Investigation, Visualization, Validation
Mohamed-Rida Tagajdid: Project Administration, Validation
Hicham Elannaz: Project Administration, Validation
Salma Hassine: Project Administration, Validation
Abdelilah Laraqui: Project Administration, Validation
Soukaina Ouannass: Project Administration, Validation
Elarbi Bouaiti: Project Administration, Validation
Yassine Benaissi: Project Administration, Validation
Ahmad Reggad: Project Administration, Validation
Mohamed Elqatni: Project Administration, Validation
Abdelilah Radi: Project Administration, Validation
Abdelhakim Ourrai: Project Administration, Validation
Rachid Abilkassem: Supervision, Project Administration, Validation
Mostafa Elouennass: Supervision, Project Administration, Validation
Khalid Ennibi: Supervision, Project Administration, Validation
Idriss Lahlou Amine: Supervision, Project Administration, Validation
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
WHO Guidelines on Meningitis Diagnosis, Treatment and Care. World Health Organization; 2025.
https://doi.org/10.2471/B09452
|
| [2] |
Meningitis (Bacterial) and Meningococcal Disease: Recognition, Diagnosis and Management [D1] Evidence Reviews for Antibiotics for Bacterial Meningitis before or in the Absence of Identifying Causative Infecting Organism in Younger Infants. 2024.
|
| [3] |
Hueth KD, Thompson-Leduc P, Totev TI, et al. Assessment of the Impact of a Meningitis/Encephalitis Panel on Hospital Length of Stay: A Systematic Review and Meta-Analysis. Antibiotics. MDPI. 2022; 11(8).
https://doi.org/10.3390/antibiotics11081028
|
| [4] |
Biswal, D., Gautam, H., Kumar, V., Tyagi, S., Kumar, Y., Mohapatra, S., Sood, S., Dhawan, B., & Das, B. (2025). Utility of Multiplex PCR for Rapid Diagnosis of Acute Bacterial Meningitis: A North Indian Tertiary Care Experience.. Indian journal of medical microbiology, 100915.
https://doi.org/10.1016/j.ijmmb.2025.100915.
|
| [5] |
Sharma, N., Gautam, H., Tyagi, S., Raza, S., Mohapatra, S., Sood, S., Dhawan, B., Kapil, A., & Das, B. (2022). Clinical use of multiplex-PCR for the diagnosis of acute bacterial meningitis. Journal of Family Medicine and Primary Care, 11, 593 - 598.
https://doi.org/10.4103/jfmpc.jfmpc_1162_21
|
| [6] |
Naeem, A., Murtaza, M., Ayub, M., Bhatti, S., Khan, F., & Ayub, M. (2025). DIAGNOSTIC VALUE OF MULTIPLEX PCR IN DIFFERENTIATING BACTERIAL VS VIRAL MENINGITIS. Insights-Journal of Life and Social Sciences.
https://doi.org/10.71000/1fwnpg52
|
| [7] |
Ahmed, M., Askar, G., Farghaly, H., Ahmed, A., Kamal, D., Ahmed, S., & Mohamad, I. (2022). Evaluation of the accuracy of multiplex polymerase chain reaction in differentiation between bacterial and viral meningitis. Irish Journal of Medical Science, 192, 403 - 407.
https://doi.org/10.1007/s11845-022-02983-2
|
| [8] |
Goktug A, Gundogdu IA, Duyu M, Besli E. Clinical Impact of Cerebrospinal Fluid Multiplex Polymerase Chain Reaction (PCR) Testing in Children with Suspected Central Nervous System Infection. Medeni Med J. 2025; 40(3): 128-135.
https://doi.org/10.4274/MMJ.galenos.2025.43895
|
| [9] |
Acuña M, Benadof D, Yohannessen K, Leiva Y, Clement P. FilmArray® Meningoencephalitis panel in the diagnosis of central nervous system infections: stewardship and cost analysis in a paediatric hospital in Chile. BMC Pediatr. 2022; 22(1).
https://doi.org/10.1186/s12887-022-03241-1
|
| [10] |
Phi DL, Tran XD, To MM, et al. Outbreak of central nervous system infections among children in Thai Binh, Viet Nam. Emerg Microbes Infect. 2022; 11(1): 1683-1692.
https://doi.org/10.1080/22221751.2022.2088405
|
| [11] |
Aldriweesh MA, Shafaay EA, Alwatban SM, et al. Viruses Causing Aseptic Meningitis: A Tertiary Medical Center Experience With a Multiplex PCR Assay. Front Neurol. 2020; 11.
https://doi.org/10.3389/fneur.2020.602267
|
| [12] |
Messacar K, Breazeale G, Robinson CC, Dominguez SR. Potential clinical impact of the film array meningitis encephalitis panel in children with suspected central nervous system infections. Diagn Microbiol Infect Dis. 2016; 86(1): 118-120.
https://doi.org/10.1016/j.diagmicrobio.2016.05.020
|
| [13] |
Du B, Hua C, Xia Y, et al. Evaluation of the BioFire FilmArray meningitis/encephalitis panel for the detection of bacteria and yeast in Chinese children. Ann Transl Med. 2019; 7(18): 437-437.
https://doi.org/10.21037/atm.2019.08.103
|
| [14] |
Rasti R, Kumbakumba E, Nanjebe D, et al. Clinical utility of the FilmArray® meningitis/encephalitis panel in children with suspected central nervous system infection in a low-resource setting - a prospective study in Southwestern Uganda. BMC Infect Dis. 2025; 25(1).
https://doi.org/10.1186/s12879-025-10732-w
|
| [15] |
Leber AL, Everhart K, Balada-Llasat JM, et al. Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol. 2016; 54(9): 2251-2261.
https://doi.org/10.1128/JCM.00730-16
|
| [16] |
Domingues RB, Santos MV dos, Leite FBV de M, Senne C. FilmArray Meningitis/Encephalitis (ME) panel in the diagnosis of bacterial meningitis. Brazilian Journal of Infectious Diseases. 2019; 23(6): 468-470.
https://doi.org/10.1016/j.bjid.2019.10.008
|
| [17] |
Hara M, Ishihara M, Nakajima H. Use of the FilmArray® Meningitis/Encephalitis panel to detect pathogenic microorganisms in cerebrospinal fluid specimens: a single-center retrospective study. Journal of International Medical Research. 2022; 50(10).
https://doi.org/10.1177/03000605221129561
|
| [18] |
Zakariya Mohammed M, Ramadan M, Abdelhalim M, Elarab HE, Wahab Garrad A. The Results of Meningitis/Encephalitis Panel in Children with Suspected Central Nervous System Infections. Vol 90. 2023.
|
| [19] |
Park SE, Lim TJ, Nam SO, et al. Clinical utility of the FilmArray meningitis/encephalitis panel in children at a tertiary center in South Korea. Brain Dev. 2021; 43(2): 234-243.
https://doi.org/10.1016/j.braindev.2020.08.010
|
| [20] |
Bridge S, Hullsiek KH, Nerima C, et al. Evaluation of the BioFire® FilmArray® Meningitis/Encephalitis panel in an adult and pediatric Ugandan population. Journal of Medical Mycology. 2021; 31(3).
https://doi.org/10.1016/j.mycmed.2021.101170
|
| [21] |
Precit MR, Yee R, Pandey U, et al. Cerebrospinal fluid findings are poor predictors of appropriate filmarray meningitis/encephalitis panel utilization in pediatric patients. J Clin Microbiol. 2020; 58(3).
https://doi.org/10.1128/JCM.01592-19
|
| [22] |
Duff S, Hasbun R, Balada-Llasat JM, Zimmer L, Bozzette SamuelA, Ginocchio CC. Economic analysis of rapid multiplex polymerase chain reaction testing for meningitis/encephalitis in adult patients. Infection. 2019; 47(6): 945-953.
https://doi.org/10.1007/s15010-019-01320-7
|
Cite This Article
-
APA Style
Akhssas, A., Abi, R., Zaza, Q., Bouhajban, F., Qadiri, K., et al. (2026). Multiplex Real Time PCR Versus Classical CSF Analysis Study Conducted on a Moroccan Pediatric Population. American Journal of Pediatrics, 12(1), 39-47. https://doi.org/10.11648/j.ajp.20261201.16
 Copy
|
Copy
|
 Download
Download
ACS Style
Akhssas, A.; Abi, R.; Zaza, Q.; Bouhajban, F.; Qadiri, K., et al. Multiplex Real Time PCR Versus Classical CSF Analysis Study Conducted on a Moroccan Pediatric Population. Am. J. Pediatr. 2026, 12(1), 39-47. doi: 10.11648/j.ajp.20261201.16
Copy
|
Download
AMA Style
Akhssas A, Abi R, Zaza Q, Bouhajban F, Qadiri K, et al. Multiplex Real Time PCR Versus Classical CSF Analysis Study Conducted on a Moroccan Pediatric Population. Am J Pediatr. 2026;12(1):39-47. doi: 10.11648/j.ajp.20261201.16
Copy
|
Download
-
@article{10.11648/j.ajp.20261201.16,
author = {Anouar Akhssas and Rachid Abi and Qamar Zaza and Fadwa Bouhajban and Kawtar Qadiri and Souhail Bibih and Oumayma Elbouni and Soukaina Akradi and Fatima Zahra Lyaagoubi and Chaimaa Nouibi and Safae Elkochri and Younes Aouni and Fadwa Elamraoui and Yousra Elhabti and Mohamed-Rida Tagajdid and Hicham Elannaz and Salma Hassine and Abdelilah Laraqui and Bouchra Elmchichi and Nadia Touil and Soukaina Ouannass and Elarbi Bouaiti and Yassine Benaissi and Ahmad Reggad and Mohamed Elqatni and Abdelilah Radi and Abdelhakim Ourrai and Rachid Abilkassem and Mostafa Elouennass and Khalid Ennibi and Idriss Lahlou Amine},
title = {Multiplex Real Time PCR Versus Classical CSF Analysis Study Conducted on a Moroccan Pediatric Population},
journal = {American Journal of Pediatrics},
volume = {12},
number = {1},
pages = {39-47},
doi = {10.11648/j.ajp.20261201.16},
url = {https://doi.org/10.11648/j.ajp.20261201.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261201.16},
abstract = {The aim of this study is to evaluate the contribution of neuromeningeal multiplex PCR in the diagnosis of infectious meningitis within a pediatric hospital population. The secondary objective is to compare the diagnostic performance of this technique compared with conventional methods in order to optimize the utilization of multiplex PCR. This work is a retrospective study of 112 children (1 month–17 years) investigated for suspected meningitis between 2020 and 2025. CSF samples were analyzed using conventional methods and the multiplex PCR panel, with demographic and biological data reviewed. The study included 67 boys (60%) and 45 girls (40%) (male-to-female ratio 1.49), with a mean age of 6.67 years; children aged 3–5 years were the most represented. Laboratory activity increased over time, reaching 37 multiplex PCR analyses in 2024–2025. Multiplex PCR was positive in 18 patients (16%). Viruses accounted for 85% of pathogens, mainly Enteroviruses (65%), followed by HHV-6 (29%) and HSV-2 (6%). Three bacterial cases and two co-infections (11.1%) were identified. Most patients had normal CSF cytology (71%); among PCR-positive cases, 33% showed elevated CSF protein, with normal glucose in all samples. CRP levels were elevated to very high in 55.6% of cases. In conclusion; the integration of multiplex PCR as a first-line test in symptomatic children, regardless of CSF parameters, appears justified. It allows for the optimization of the care pathway through a reduction in hospitalization duration and unnecessary treatments.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Multiplex Real Time PCR Versus Classical CSF Analysis Study Conducted on a Moroccan Pediatric Population
AU - Anouar Akhssas
AU - Rachid Abi
AU - Qamar Zaza
AU - Fadwa Bouhajban
AU - Kawtar Qadiri
AU - Souhail Bibih
AU - Oumayma Elbouni
AU - Soukaina Akradi
AU - Fatima Zahra Lyaagoubi
AU - Chaimaa Nouibi
AU - Safae Elkochri
AU - Younes Aouni
AU - Fadwa Elamraoui
AU - Yousra Elhabti
AU - Mohamed-Rida Tagajdid
AU - Hicham Elannaz
AU - Salma Hassine
AU - Abdelilah Laraqui
AU - Bouchra Elmchichi
AU - Nadia Touil
AU - Soukaina Ouannass
AU - Elarbi Bouaiti
AU - Yassine Benaissi
AU - Ahmad Reggad
AU - Mohamed Elqatni
AU - Abdelilah Radi
AU - Abdelhakim Ourrai
AU - Rachid Abilkassem
AU - Mostafa Elouennass
AU - Khalid Ennibi
AU - Idriss Lahlou Amine
Y1 - 2026/03/26
PY - 2026
N1 - https://doi.org/10.11648/j.ajp.20261201.16
DO - 10.11648/j.ajp.20261201.16
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 39
EP - 47
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20261201.16
AB - The aim of this study is to evaluate the contribution of neuromeningeal multiplex PCR in the diagnosis of infectious meningitis within a pediatric hospital population. The secondary objective is to compare the diagnostic performance of this technique compared with conventional methods in order to optimize the utilization of multiplex PCR. This work is a retrospective study of 112 children (1 month–17 years) investigated for suspected meningitis between 2020 and 2025. CSF samples were analyzed using conventional methods and the multiplex PCR panel, with demographic and biological data reviewed. The study included 67 boys (60%) and 45 girls (40%) (male-to-female ratio 1.49), with a mean age of 6.67 years; children aged 3–5 years were the most represented. Laboratory activity increased over time, reaching 37 multiplex PCR analyses in 2024–2025. Multiplex PCR was positive in 18 patients (16%). Viruses accounted for 85% of pathogens, mainly Enteroviruses (65%), followed by HHV-6 (29%) and HSV-2 (6%). Three bacterial cases and two co-infections (11.1%) were identified. Most patients had normal CSF cytology (71%); among PCR-positive cases, 33% showed elevated CSF protein, with normal glucose in all samples. CRP levels were elevated to very high in 55.6% of cases. In conclusion; the integration of multiplex PCR as a first-line test in symptomatic children, regardless of CSF parameters, appears justified. It allows for the optimization of the care pathway through a reduction in hospitalization duration and unnecessary treatments.
VL - 12
IS - 1
ER -
Copy
|
Download