Ameloblastoma is a benign but locally invasive neoplasm that arises from odontogenic epithelium of the dental lamina. It is classified into the conventional, unicystic, extraosseous/peripheral and metastasizing variants. It is the most common odontogenic tumour in Nigeria and other developing countries. It affects individuals of all ages, has a peak of occurrence in the fourth and fifth decades with no sex predilection. The Mandible is the most commonly affected site and the conventional variant is predominant. The aim of this study is to document the demographics and Pathomorphology of ameloblastoma diagnosed at the Jos University Teaching Hospital over the past nine years. There is no previous documentation of the pattern of this tumour in the North-central region of Nigeria making this study relevant. This is a retrospective observational review of all cases of ameloblastoma diagnosed histologically at the Jos University Teaching Hospital between January 1st 2015 to December 31st 2023. Materials utilized consisted of patient clinical case files, electronic histopathology result records, histopathology glass slides and formalin fixed paraffin embedded tissue blocks. The patient age, sex, anatomic location of tumour in the Jaw/face and pathomorphological features were recorded for all cases. The data obtained was analysed using Epi-info 7 (version 3.5.4) and Microsoft-Excel. Results were presented in tables and charts. Fifty one cases of ameloblastoma were diagnosed during the 9 years of review. Their ages ranged between 6 and 65 years with a mean age of 30.9±13.8 years and a peak of occurrence in the third decade. There were 29 males and 22 females with a male to female ratio (M:F) of 1.3:1. Ninety-two percent of cases occurred in the mandible and 8% in the maxilla. The conventional variant accounted for 72.5% of cases and the unicystic variant 27.5%. The follicular type accounted for 64.8% of cases of conventional ameloblastoma. Ameloblastoma occurred more commonly in males with a peak in the third decade. A vast majority of cases involved the mandible and the conventional type was predominant. This demographic pattern supports existing evidence that ameloblastoma occurs more commonly in males and in relatively younger patients in Africa.
| Published in | Biomedical Sciences (Volume 10, Issue 2) |
| DOI | 10.11648/j.bs.20241002.12 |
| Page(s) | 23-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Ameloblastoma, Jos, North-Central, Nigeria, Conventional, Mandible
0-10 | 11-20 | 21-30 | 31-40 | 41-50 | 51-60 | 61-70 | Total | |
|---|---|---|---|---|---|---|---|---|
Unicystic | 0 | 3 | 4 | 4 | 2 | 1 | 0 | 14 |
Follicular | 1 | 5 | 9 | 4 | 3 | 0 | 2 | 24 |
Plexiform | 0 | 1 | 0 | 0 | 0 | 2 | 0 | 3 |
Acanthomatous | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
Follicular-Acanthomatous | 0 | 2 | 3 | 1 | 0 | 1 | 0 | 7 |
Follicular-plexiform | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 2 |
Total | 1 | 12 | 17 | 11 | 6 | 4 | 2 | 51 |
Male | Female | Total | |
|---|---|---|---|
Unicystic | 8 | 6 | 14 |
Follicular | 15 | 9 | 24 |
Plexiform | 1 | 2 | 3 |
Acanthomatous | 0 | 1 | 1 |
Follicular-Acanthomatous | 4 | 3 | 7 |
Follicular-plexiform | 1 | 1 | 2 |
Total | 29 | 22 | 51 |
Mandible | Maxilla | Total | |
|---|---|---|---|
Unicystic | 12 | 2 | 14 |
Follicular | 23 | 1 | 24 |
Plexiform | 2 | 1 | 3 |
Acanthomatous | 1 | 0 | 1 |
Follicular-Acanthomatous | 7 | 0 | 7 |
Follicular-plexiform | 2 | 0 | 2 |
Total | 47 | 4 | 51 |
| [1] | Vered M, Muller S, Heikinheimo K. Benign epithelial odontogenic tumours. In: El-Nagger AK, Chan JKC, Grandis JR, Takata T, Slootweg PG, eds. WHO Classification of head and neck tumours. Lyon: IARC; 2017. p. 215-19. |
| [2] | Agbaje OJ, Adisa AO, Petrova MI et al. Biological profile of ameloblastoma and its location in the jaw in 1246 Nigerians. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2018; 126(5): 424-31. |
| [3] | Effiom OA, Ogundana OM, Akinshipo AO, Akintoye SO. Ameloblastoma: current etiopathological concepts and management. Oral Dis. 2018; 24(3): 307–16. |
| [4] | Masthan KM, Anitha N, Krupaa J, Manikkam S. Ameloblastoma. J Pharm Bioallied Sci. 2015; 7(Suppl 1): S167-70. |
| [5] | Oginni FO, Stoelinga PJ, Ajike SA et al. A prospective epidemiological study on odontogenic tumours in a black African population, with emphasis on the relative frequency of ameloblastoma. Int J Oral Maxillofac Surg.2015; 44(9): 1099-105. |
| [6] | Lasisi TJ, Adisa AO, Olusanya AA. Appraisal of jaw swellings in a Nigerian tertiary healthcare facility. J Clin Exp Dentist. 2013; 5(1): e42–e47. |
| [7] | Iyogun CA, Omitola OG, Ukegheson GE. Odontogenic tumors in Port Harcourt: south-south geopolitical zone of Nigeria. J Oral Maxillofac Pathol. 2016; 20(2): 190–3. |
| [8] | Bassey GO, Osunde OD, Anyanechi CE. Maxillofacial tumors and tumor-like lesions in a Nigerian teaching hospital: an eleven year retrospective analysis. Afr Health Sci. 2014; 14(1): 56–63. |
| [9] | Iyogun C, Sule AA, Omitola OG. Relative prevalence of odontogenic cysts and tumours in Kano, Northern Nigeria. J Dent Oral Health. 2017; 3(4): 071. |
| [10] | Lawal AO, Adisa AO, Olusanya AA. Odontogenic tumours: a review of 266 cases. J Clin Exp Dentist. 2013; 5(1): e13–e17. |
| [11] | Mansour M, El-Mofty SK. Tumours and cysts of the Jaws. In: Pfeifer JD, Humphrey PA, Ritter JH, Dehner LP, editors. The Washington manual of surgical pathology. Philadelphia: Wolters Kluwer, 2020; p. 170-206. |
| [12] | Castano BO, Oluwakuyide RT, Ayodele AO et al. Pattern of histologic variants of ameloblastoma in a secondary healthcare facility in Lagos state: a 5-year retrospective study. Niger Dent J. 2023; 31(1): 19-26. |
| [13] | Ladeinde Al, Ogunlewe MO, Bamgbose BO, Adeyemo WL, Ajayi OF, Arotiba GT et al. Ameloblastoma: analysis of 207 cases in a Nigerian Teaching Hospital. Quintessence Int. 2006; 37(7): 69-74. |
| [14] | Ibikunle AA, Taiwo AO, Braimah RO, Adeyemi M, Abdullahi K, Sahabi SM. Ameloblastoma: Clinicopathologic and therapeutic analysis of 67 cases seen at Usmanu Danfodiyo University Teaching Hospital Sokoto, Nigeria. IJHAS. 2018; 7(4): 240-45. |
| [15] | Soyele OO, Akinshipo AO, Effiom OA et al. A multi-centre evaluation of 566 cases of ameloblastoma in Nigeria by the African Oral Pathology Research Consortium. Oral Cancer. 2019; 3: 9-15. |
| [16] | Arotiba GT, Ladeinde AL, Ajike SO, Ugboko VI, Ajayi OF. Ameloblastoma in Nigerian Children and Adolescents: A Review of 79 Cases. J Oral Maxillofac Surg. 2005; 63(6): 747-51. |
| [17] | Adebiyi KE, Ugboko VI, Omoniyi-Esan GO, Ndukwe KC, Oginni FO. Clinicopathological analysis of histological variants of ameloblastoma in a suburban Nigerian population. HEAD FACE MED. 2006; 2: 1-8. |
| [18] | Okechi UC, Akpeh JO, Chukwuneke FN et al. Ameloblastoma of the jaws in children: an evaluation of cases seen in a tertiary hospital in South-Eastern Nigeria. Ghana Med J 2020; 54(1): 36-41 |
| [19] | Fomete B, Adebayo ET, Ogbeifun JO. Ameloblastoma: Our clinical experience with 68 cases. J Orofac Sci. 2014; 6(1): 7-24. |
| [20] | Younis M, Baig N, Haq AU et al. Unicystic ameloblastoma: A distinct clinicopathologic entity. Pakistan Oral and Dent J 2009; 29(1): 9-12. |
| [21] | Patsa S, Jadav RB, Halder GC, Ray JG, Datta S, Deb T. Demographic and histopathological variation of ameloblastoma: a hospital-based study. J Oral Maxillofac Pathol 2016; 20(2) 230-33. |
| [22] | Jing W, Xuan M, Lin Y et al. Odontogenic tumours: a retrospective study of 1642 cases in a Chinese population. Int J Oral Maxillofac Surg. 2007; 36(1): 20-5. |
| [23] | Singh T, Wiesenfeld D, Clement J, Chandu A, Nastri. Ameloblastoma: demographic data and treatment outcomes from Melbourne, Australia. Austral Dent J. 2015; 60(1): 24-9. |
| [24] | Milman T, Ying GS, Pan W, LiVolsi V (2016) Ameloblastoma: 25 year experience at a single institution. Head Neck Pathol 10: 513-20. |
| [25] | Olaitan AA, Adekeye EO: Clinical features and management of ameloblastoma of the mandible in children and adolescents. Br J Oral Maxillofac Surg.1996; 34(3): 248-51. |
| [26] | Blackwood HJJ. Odontogenic tumours in the child. Br Dent J 1965; 119(10): 431-38. |
| [27] | Ord RA, Blanchaert RH. Jr, Nikitakis NG and Sauk JJ. Ameloblastoma in children. J Oral Maxillofac. Surg. 2002; 60(7): 762-70. |
| [28] | Olaitan AA, Adeola DS, Adekeye EO. Ameloblastoma: clinical features and management of 315 cases from Kaduna, Nigeria. J Cranio-maxillofac Surg. 1993; 21(8): 351-5. |
| [29] | Omitola O, Fakuade BO, Aliyu IL. Ameloblastoma: a clinicopathologic review of cases seen in a tertiary health centre in Gombe, North Eastern Nigeria. Afr J of Oral Maxillofac Path Med. 2017; 3: 19–23. |
| [30] | Tatapudi R, Samad SA, Reddy RS, Boddu NK. Prevalence of ameloblastoma: A three-year retrospective study. J Indian Acad Oral Med Radiol. 2014; 26(2): 145-51. |
| [31] | Oomens MA, van der Waal I. Epidemiology of ameloblastomas of the jaws; a report from the Netherlands. Med Oral Patol Oral Cir Bucal. 2014; 19(6): e581-3. |
APA Style
Akpa, P. O., Emmanuel, I., Kwaghe, B. V., Okwudire-Ejeh, I. A., Dauda, A. M., et al. (2024). Demographics and Pathomorphology of Ameloblastoma: A 9 Year Retrospective Review at a Tertiary Health Care Centre in North-Central Nigeria. Biomedical Sciences, 10(2), 23-29. https://doi.org/10.11648/j.bs.20241002.12
ACS Style
Akpa, P. O.; Emmanuel, I.; Kwaghe, B. V.; Okwudire-Ejeh, I. A.; Dauda, A. M., et al. Demographics and Pathomorphology of Ameloblastoma: A 9 Year Retrospective Review at a Tertiary Health Care Centre in North-Central Nigeria. Biomed. Sci. 2024, 10(2), 23-29. doi: 10.11648/j.bs.20241002.12
AMA Style
Akpa PO, Emmanuel I, Kwaghe BV, Okwudire-Ejeh IA, Dauda AM, et al. Demographics and Pathomorphology of Ameloblastoma: A 9 Year Retrospective Review at a Tertiary Health Care Centre in North-Central Nigeria. Biomed Sci. 2024;10(2):23-29. doi: 10.11648/j.bs.20241002.12
@article{10.11648/j.bs.20241002.12,
author = {Philip Ojile Akpa and Innocent Emmanuel and Barka Vandi Kwaghe and Ijeoma Ahunna Okwudire-Ejeh and Ayuba Madachi Dauda and Olugbenga Akindele Silas},
title = {Demographics and Pathomorphology of Ameloblastoma: A 9 Year Retrospective Review at a Tertiary Health Care Centre in North-Central Nigeria
},
journal = {Biomedical Sciences},
volume = {10},
number = {2},
pages = {23-29},
doi = {10.11648/j.bs.20241002.12},
url = {https://doi.org/10.11648/j.bs.20241002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.bs.20241002.12},
abstract = {Ameloblastoma is a benign but locally invasive neoplasm that arises from odontogenic epithelium of the dental lamina. It is classified into the conventional, unicystic, extraosseous/peripheral and metastasizing variants. It is the most common odontogenic tumour in Nigeria and other developing countries. It affects individuals of all ages, has a peak of occurrence in the fourth and fifth decades with no sex predilection. The Mandible is the most commonly affected site and the conventional variant is predominant. The aim of this study is to document the demographics and Pathomorphology of ameloblastoma diagnosed at the Jos University Teaching Hospital over the past nine years. There is no previous documentation of the pattern of this tumour in the North-central region of Nigeria making this study relevant. This is a retrospective observational review of all cases of ameloblastoma diagnosed histologically at the Jos University Teaching Hospital between January 1st 2015 to December 31st 2023. Materials utilized consisted of patient clinical case files, electronic histopathology result records, histopathology glass slides and formalin fixed paraffin embedded tissue blocks. The patient age, sex, anatomic location of tumour in the Jaw/face and pathomorphological features were recorded for all cases. The data obtained was analysed using Epi-info 7 (version 3.5.4) and Microsoft-Excel. Results were presented in tables and charts. Fifty one cases of ameloblastoma were diagnosed during the 9 years of review. Their ages ranged between 6 and 65 years with a mean age of 30.9±13.8 years and a peak of occurrence in the third decade. There were 29 males and 22 females with a male to female ratio (M:F) of 1.3:1. Ninety-two percent of cases occurred in the mandible and 8% in the maxilla. The conventional variant accounted for 72.5% of cases and the unicystic variant 27.5%. The follicular type accounted for 64.8% of cases of conventional ameloblastoma. Ameloblastoma occurred more commonly in males with a peak in the third decade. A vast majority of cases involved the mandible and the conventional type was predominant. This demographic pattern supports existing evidence that ameloblastoma occurs more commonly in males and in relatively younger patients in Africa.
},
year = {2024}
}
TY - JOUR T1 - Demographics and Pathomorphology of Ameloblastoma: A 9 Year Retrospective Review at a Tertiary Health Care Centre in North-Central Nigeria AU - Philip Ojile Akpa AU - Innocent Emmanuel AU - Barka Vandi Kwaghe AU - Ijeoma Ahunna Okwudire-Ejeh AU - Ayuba Madachi Dauda AU - Olugbenga Akindele Silas Y1 - 2024/04/17 PY - 2024 N1 - https://doi.org/10.11648/j.bs.20241002.12 DO - 10.11648/j.bs.20241002.12 T2 - Biomedical Sciences JF - Biomedical Sciences JO - Biomedical Sciences SP - 23 EP - 29 PB - Science Publishing Group SN - 2575-3932 UR - https://doi.org/10.11648/j.bs.20241002.12 AB - Ameloblastoma is a benign but locally invasive neoplasm that arises from odontogenic epithelium of the dental lamina. It is classified into the conventional, unicystic, extraosseous/peripheral and metastasizing variants. It is the most common odontogenic tumour in Nigeria and other developing countries. It affects individuals of all ages, has a peak of occurrence in the fourth and fifth decades with no sex predilection. The Mandible is the most commonly affected site and the conventional variant is predominant. The aim of this study is to document the demographics and Pathomorphology of ameloblastoma diagnosed at the Jos University Teaching Hospital over the past nine years. There is no previous documentation of the pattern of this tumour in the North-central region of Nigeria making this study relevant. This is a retrospective observational review of all cases of ameloblastoma diagnosed histologically at the Jos University Teaching Hospital between January 1st 2015 to December 31st 2023. Materials utilized consisted of patient clinical case files, electronic histopathology result records, histopathology glass slides and formalin fixed paraffin embedded tissue blocks. The patient age, sex, anatomic location of tumour in the Jaw/face and pathomorphological features were recorded for all cases. The data obtained was analysed using Epi-info 7 (version 3.5.4) and Microsoft-Excel. Results were presented in tables and charts. Fifty one cases of ameloblastoma were diagnosed during the 9 years of review. Their ages ranged between 6 and 65 years with a mean age of 30.9±13.8 years and a peak of occurrence in the third decade. There were 29 males and 22 females with a male to female ratio (M:F) of 1.3:1. Ninety-two percent of cases occurred in the mandible and 8% in the maxilla. The conventional variant accounted for 72.5% of cases and the unicystic variant 27.5%. The follicular type accounted for 64.8% of cases of conventional ameloblastoma. Ameloblastoma occurred more commonly in males with a peak in the third decade. A vast majority of cases involved the mandible and the conventional type was predominant. This demographic pattern supports existing evidence that ameloblastoma occurs more commonly in males and in relatively younger patients in Africa. VL - 10 IS - 2 ER -
Department of Anatomic Pathology and Forensic Medicine, Jos University Teaching Hospital, Jos, Nigeria; Department of Pathology, University of Jos, Jos, Nigeria
Department of Anatomic Pathology and Forensic Medicine, Jos University Teaching Hospital, Jos, Nigeria; Department of Pathology, University of Jos, Jos, Nigeria
Department of Anatomic Pathology and Forensic Medicine, Jos University Teaching Hospital, Jos, Nigeria
Anatomic Pathology and Forensic Medicine Department, Asokoro District Hospital, Abuja, Nigeria
Department of Anatomic Pathology and Forensic Medicine, Jos University Teaching Hospital, Jos, Nigeria; Department of Pathology, University of Jos, Jos, Nigeria
Department of Anatomic Pathology and Forensic Medicine, Jos University Teaching Hospital, Jos, Nigeria; Department of Pathology, University of Jos, Jos, Nigeria
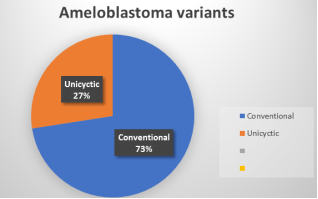
Figure 1. Chart showing the morphological variants of ameloblastoma.
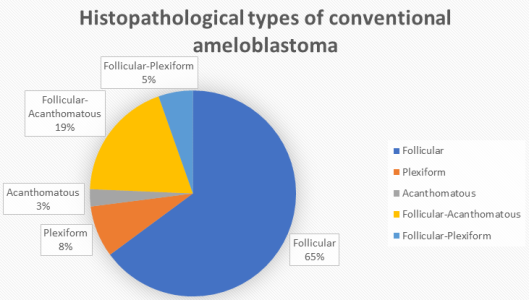
Figure 2. Chart showing the histopathological types of conventional ameloblastoma.

Figure 3. Photomicrographs x 100 magnification (Hematoxylin and Eosin stain) A. Follicular ameloblastoma with islands of odontogenic epithelium surrounded by fibrous stroma. B. Plexiform ameloblastoma showing cords of anastomosing odontogenic epithelial cells. C. Acanthomatous ameloblastoma showing squamous metaplasia and variable keratinization in stellate reticulum-like cells. D. Unicystic ameloblastoma showing a cyst lined by ameloblastic epithelium.
Information

