Abstract
Teenage pregnancies are a global problem mainly in marginalised communities resulting in complications, societal rejection and deaths. In Zimbabwe, 48% of the teenage pregnancies occurred between 13-19 years. Mutasa District, one of the Districts in Zimbabwe has high rate of teenage pregnancies. Teenage abortions rose from 3/1000 in 2018 to 5/1000 in 2019. We conducted a study on the factors associated with teenage pregnancies in Mutasa District in the year 2018 and 2019. The specific objectives were to determine the prevalence of teenage pregnancies, to determine the sociocultural, economic and religious factors influencing teenage pregnancies and to assess the availability and utilisation of Adolescent Sexual and Reproductive Health Services. A multi-methods+ study design was used with a sample size of 80 cases and 80 controls from four hospitals in Mutasa. Systematic sampling was employed where every 3rd subject was systematically selected upon satisfaction of the inclusion criteria, with sampling interval observed. A quantitative survey and Focus Group Discussions (FGDs) were used to collect data. The results showed that 72 (90%) of the cases only had primary school education. Being single orphans 60 (75%), having information and education gaps 77 (96.3%), being chased off home to go to the male partner 49 (61.3%) were the prevalent factors linked to teenage pregnancies. Having been disciplined when found with contraceptives led to 41 (51.3%) of the pregnancies. Having the boyfriend as a source of livelihood allowances contributed to 59 (73.8%) of teenage pregnancies while being a member of an Apostolic Sect contributed 65 (82.3%) of the cases. The FGDs revealed that the Youth Friendly Centres were inadequate for the community, poorly resourced having no comprehensive preventive services and therefore poorly utilised. In addition, teenage pregnancy preventions were stereotyped to females only with current interventions being predominantly reactionary than preventive. The findings of this study suggest the need for reproductive health information, gender inclusive programming, and provision of a sundry of well-resourced Youth Friendly Centres in the District and a focus on tailor-made preventive interventions rather than punitive ones.
Keywords
Teenage Pregnancy, Low Self-Esteem, Culture
1. Introduction
Teenage pregnancy is pregnancy in human females under the age of 20 at the time that the pregnancy ends
| [1] | United Nations Population Fund. (2013). Girlhood, not motherhood: Preventing adolescent pregnancy. New York. |
[1]
. Teenage pregnancy remains a major challenge in both developed and developing countries. Each year an estimated 21 million pregnancies occur among adolescent girls of age 15–19 years in developing countries, almost half of which are unintended
| [2] | World Health Organisation. (2018). Adolescent pregnancy fact sheet. Geneva. |
[2]
. This results in an estimated 16 million births and more than 3.2 million abortions annually. In Sub-Saharan Africa (SSA), an estimated 45% of the pregnancies among young women aged 15–19 are unintended resulting in unintended births, unsafe abortions and miscarriages
. Nearly half of the unsafe abortion cases in SSA also occur among adolescent girls and young women under the age of 25 years. In Kenya, for instance, adolescent girls make up nearly 17% of post abortion cases and account for 45% of severe abortion related complications treated in health facilities
.
Unmarried pregnant adolescents face stigma or rejection by parents, peers and society and sometimes have threats of violence. Similarly, girls who become pregnant before age of 18years are more likely to experience violence within marriage or their partnership
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Teenage pregnancy can lead to dropping out of school resultantly perpetuating cycles of poverty thus child marriage reduces future earnings of girls by an estimated 9%. The WHO reports that, of the total pregnancies among female adolescents aged 15-19 years in Zimbabwe, 48% were unplanned
.
Sub-Saharan Africa has the highest rate of adolescent pregnancy in the world. While pregnancy during adolescence poses higher risks for the mother and the baby, the utilisation of maternity care to mitigate the effects is low
| [4] | World Bank. (2017). Economic impacts of child marriage: Global synthesis report. Washington. |
[4]
.
1.1. Demographic Factors Affecting Teenage Pregnancy
Demographic factors do play an important role in determining adolescent pregnancies and marriages. The place of residence, lifestyle practices, parenthood and age specifics issues have bearing on childhood pregnancies. Internationally, unintended births among unmarried adolescent girls are a major contributor to maternal and childhood mortality perpetuating the vicious cycle of ill-health, poverty and truncated educational opportunities
. An estimated 14 million young women aged 15–19 years gave birth each year between 1995 and 2000, with 12.8 million births occurring to adolescents in the developing countries. Teenage pregnancy is a serious public health and social problem, with 95% occurring in developing countries, Zimbabwe included. Adolescent pregnancy and childbearing entail a high risk of maternal death for the adolescent, and the children of young mothers have higher levels of morbidity and mortality
.
Regionally, most teenage pregnancies and childbirths take place in west and central Africa, east and southern Africa, South Asia, Latin America, and the Caribbean
| [6] | Neal, S. E., Chandra-M, V., & Chou, D., (2015). Adolescent first births in East Africa: disaggregating characteristics, trends and determinants. Reproductive Health Center, Dar es Salaam. |
[6]
. As a Southern Africa country, Zimbabwe is not an exception therefore the study investigated teenage pregnancies in Mutasa District. The environments in which adolescents reside also play a significant role in adolescent pregnancy. Striking differences in adolescent pregnancies were observed between urban and rural areas. Adolescents from rural areas were at greater risk of pregnancy (20%) compared to their urban counterparts (9%). The high rates of adolescent pregnancy observed in the rural areas could be due to poverty which is more prevalent in rural areas than urban areas (Zimbabwe National Statistics Agency
| [7] | Zimbabwe National Statistics Agency. (2015). Zimbabwe multiple indicator cluster survey 2014, Final Report. Harare. |
[7]
.
1.2. Knowledge Factors Affecting Teenage Pregnancy
Knowledge is quite critical in determining the susceptibility to teenage pregnancies. Highly knowledgeable and empowered teenagers are not prone to manipulation to fall prey to teenage pregnancies. In Kenya it was reported that females with no education had their first sexual intercourse three years earlier than their counterparts with at least a secondary school education. Marriages and pregnancies were delayed if teenagers furthered their education to secondary and post- secondary levels
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Most teenage girls fall pregnant at the age of fifteen, with girls as young as eleven found to have conceived, suggesting a strong relationship between HIV/AIDS and high risk of teenage pregnancy due to permissive attitudes inadvertent of consequences
.
In Zimbabwe, low levels of education amongst parents and children could be the reason behind early motherhood and drop out from school
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
.
1.3. Social Factors Affecting Teenage Pregnancy
Females exposed to abuse, domestic violence, and family strife in childhood are more likely to become pregnant as teenagers, and the risk of becoming pregnant as a teenager increases with the number of adverse childhood experiences
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. One-third of teenage pregnancies could be prevented by eliminating exposure to abuse, violence, and family strife since a girl is also more likely to become a teenage parent if her mother or older sister gave birth in her teens
| [2] | World Health Organisation. (2018). Adolescent pregnancy fact sheet. Geneva. |
[2]
.
Teen pregnancy and motherhood can influence younger siblings. A study by Neal and colleagues reported that the younger sisters of teen mothers were less likely to emphasize the importance of education and employment but more likely to accept sexual behaviour, parenting, and marriage at younger ages
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[10]
. If the younger sisters of teenage parents babysit the children, they have an increased probability of getting pregnant themselves. A study from Norway in 2011 found that the probability of a younger sister having a teenage pregnancy went from 1:5 to 2:5 if the elder sister had a baby as a teenager
.
The major cause of teenage pregnancy is the lack of guidance by guardians and parents who are reluctant or do not understand the need to educate teenagers about the sexual reproductive behaviour. This leaves the teenagers not properly guided during their adolescent stage of development yet this is the critical stage in which their cognitive, emotional, psychological and social skills mature
| [12] | Anda, R. F., Felitti, V. J., Chapman, D. P., Croft J. B., Williamson, D. F., Santelli J., Dietz, P. M., Marks, J. S., (2001). Abused boys, battered mothers, and male Involvement in teen pregnancy. USA: Paediatrics Atlanta Georgia. https://doi.org/10.1542/peds.107.2.e19 |
[12]
. There is also a significant contribution of early marriages in increasing the rate of teenage pregnancy as it was found out that 15% of the young women aged between 20-29 years old were married at the age of 15, while 49% were married by the age of 18
| [4] | World Bank. (2017). Economic impacts of child marriage: Global synthesis report. Washington. |
[4]
.
Children not staying with both parents have been reported in several studies to be vulnerable to adolescent pregnancy. Children staying on their own and orphans were more likely to be at risk of adolescent pregnancy because of social economic reasons
| [13] | World Health Organization. (2011). Guidelines for preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. Geneva. |
[13]
. Circumstances of non-activity and idleness like COVID 19 lockdown in Zimbabwe have had teenage girls elope as they execute their energies towards silent sexual engagements. The lock down which helped to prevent the spread of the coronavirus has impacted negatively on young girls. A lot of them had become victims of defilement and teenage pregnancy. Refugee families are many times idle, which predisposes them to sexual activity
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[10]
.
1.4. Cultural and Religious Factors Affecting Teenage Pregnancy
Cultural and religious factors are renowned factors that propel and anchor teenage pregnancies in hosts of settings. Cultural and religious factors can be both risks and protective factors to teenage marriages in a myriad of ramifications. Religion and culture do facilitate teenage pregnancies in different means. A study found that teenage marriages and pregnancies were rife and culturally acceptable in some communities like in South Asian culture
| [14] | Acharya, D. R., Bhattaria, R., Poobalan, A. S., Van Teijlingen, E., & Chapman, G. N., (2007). Factors associated with teenage pregnancy in South Asia: A systemic review. United Kingdom: E-prints Bournemouth. http://www.hsj.gr/volume4/issue1/402.pdf |
[14]
.
Some religious sects do perpetuate childhood marriages and pregnancies
. In Malawi many societies expect teenagers to behave like adults with the importance of child bearing being communicated to girls at early age. Cultural challenges in Zimbabwe expose teenagers to unwanted pregnancies by hindering access to services. Of the pregnancies among female adolescents aged 15-19 years in Zimbabwe, 48% of them were unplanned
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Difficulties in accessing contraceptives caused adolescent girls to be exposed to unplanned pregnancy complications and deaths as a result of illegal abortions. Unlike the Zimbabwe cultural position, prohibiting the adolescents’ access to contraceptives, some countries in Africa like Nigeria allow access to Sexual Reproductive Health (SRH) services to protect themselves
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
.
In Zimbabwe, there have been reported high teenage pregnancies among children belonging to the Apostolic Sects as they are often married off to older members of the church. However, adolescents who did not belong to any religion had greater odds of getting pregnant
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[10]
.
1.5. Economic Factors Affecting Teenage Pregnancy
Economics of an institution both at micro and macro levels is a cause of concern in teenage pregnancies. Robust sound economics are protective while the flimsy and frail ones bear untold consequences for teenage pregnancies. Amnesty International (2008) found that a staggering 92% of school girls indicated that they were enslaved for sex in exchange for gifts and money for survival. It has been revealed that girls may indulge in sexual activities in exchange for goods, money and livelihoods
| [13] | World Health Organization. (2011). Guidelines for preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. Geneva. |
[13]
.
A study in Malawi reported that 66% of adolescents had accepted money or gifts in exchange for sex
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Adolescents from affluent families were protected from pregnancy compared to their peers from impoverished families. Poverty and socio-economic deprivation expose adolescent girls to early sexual debut and intergenerational sex
| [7] | Zimbabwe National Statistics Agency. (2015). Zimbabwe multiple indicator cluster survey 2014, Final Report. Harare. |
[7]
.
Poverty and child-headed households were identified as the major contributors to teenage pregnancy
. As a result of poor or no parental guidance and control, children engage in sexual activities at a very young age. There was a definite link between teenage pregnancy and poverty and high rate of teenage pregnancy among black poor teenagers in South Africa
. Economically poor countries have more teenage mothers as compared with economically rich countries and poverty has a role in perpetuating teenage pregnancy
| [16] | Anthony, M. O., Primus, C. C., & Stephen, L., (2019). Predictors of teenage Pregnancy among girls aged 13–19 years in Uganda: A community based-case control study, Uganda, Makerere University. Kampala. https://doi.org/10.1186/s12884-019-2347-y |
[16]
.
1.6. Media and Exposures Affecting Teenage Pregnancy
Media has both a risk and protective facet in teenage pregnancies. Teenagers are most likely to get pressure from the family and their peers by either enhancing early pregnancy or opposing girls’ accessing sexual and reproductive education and other information about pregnancy prevention. A similar study, lack of access to sex education predisposes adolescent females to pregnancies as the teenagers tend to do trial and error
A study conducted in 2006 found that adolescents who were more exposed to sexuality in the media were also more likely to engage in early sexual activities themselves than those who were not exposed. Teens exposed to the most sexual content on TV were twice as likely as teens watching less of this material to become pregnant before they reach age 20
. Movies and television shows often glamorize pregnancy, and make it seem as though sex is a necessary to gain social acceptance
. Watching lots of sexual content on TV can influence teens to have sex at earlier ages and television shows that highlight the positive aspects of sexual behaviour without the risks can also lead teens to have unprotected sex before they are ready to make responsible and informed decisions
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
.
Alcohol and drugs may encourage unintended sexual activities. Alcohol and drug exposures and abuse do prompt teenage pregnancy in a greater way. Some teenagers experiment with alcohol and drugs, which can lead to a lack of impulse control and loss of the ability to make coherent decisions
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
, underage drinking leads to 75% of teenage pregnancies with 91% of pregnant teenagers that drank not having planned to engage in sexual activity when they conceived. Young people need education on drugs and alcohol in order to make the best decisions for themselves and to have full awareness of the effects alcohol and drugs can have if not controlled safely
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
.
Inadequate knowledge about the harms enshrined in teenage pregnancy render the teenage susceptible to pregnancy. Undesirable attitudes and practices like drug and alcohol abuse is a factor that could propel teenage pregnancy. Thus adolescents and teenagers require information to remain alert and avoid attitudes and practices that enhance pregnancy
| [4] | World Bank. (2017). Economic impacts of child marriage: Global synthesis report. Washington. |
[4]
.
1.7. Sexual and Reproductive Health Delivery Systems and Facilities Affecting Teenage Pregnancy
Health system and health staff attitudes could hinder teenagers from seeking contraceptive protection contributing to teenage pregnancy. A study carried by
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
showed that most nurses feel uncomfortable to provide teenagers with contraception because of their belief systems; they behold that adolescent and teenagers should not engage in sexual intercourse at an early age. The nurses’ attitude to the contraceptive requests was highly judgmental and they were perceived as indifferent and unhelpful to teenage girls and mothers
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
.
In 2011, the WHO set guidelines on preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. The guidelines advocate for adolescent pregnancy prevention among all stakeholders through interventions such as information provision, sexuality and health education, life skills building, contraceptive counselling and service provision, and creation of supportive environment
| [13] | World Health Organization. (2011). Guidelines for preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. Geneva. |
[13]
.
Inadequate teenage reproductive and sexual health services and lower decision making do significantly affect teenage pregnancy. A wide range of factors contribute to the high rates of unintended pregnancy and unplanned births among adolescents. Poor knowledge of sexual and reproductive health services, legal barriers to accessing services, provider bias, stigma around premarital sex and lower decision making autonomy of married adolescents are among the factors contributing to unintended pregnancies
. Zimbabwe has no well laid down policies that permit adolescents to access family planning services
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
.
In Mutasa district cases of teenage pregnancies have been on the increase since 2018 and 2019. Transfers to Mutare Provincial Hospital for further management of teenage pregnancies increased drastically from 18 cases in 2018 to 31 cases in 2019. Cases of abortion increased from 3 per 1000 in 2018 to 11 per 1000 in 2019 with the number of deaths rising from four in 2018 to seven in 2019. This study sought to establish factors associated with teenage pregnancies in Mutasa District, Manicaland Province for the period 2018 to 2019. The study sought specifically to:
(i) determine the prevalence of teenage pregnancies in Mutasa District for the period 2018 to 2019.
(ii) determine the cultural, socio-economic and religious factors influencing teenage pregnancies in Mutasa District for the period 2018 to 2019.
(iii) assess the availability and utilisation of Adolescent Sexual and Reproductive Health Services for the period 2018 to 2019.
2. Methods
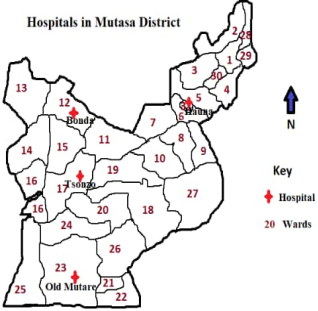
The study was conducted in Mutasa District, in Zimbabwe at conveniently selected study sites, that is, Hauna Hospital, Old Mutare Hospital, Bonda Hospital and Tsonzo Rural Hospital. Mutasa District has a total area of 2774 square km and shares boundaries with Mutare District to the south, Nyanga District to the north, Makoni District to the west and Mozambique to the East. The district has a very rugged terrain and has five ecological regions. On the Economic dimension the district thrives on subsistence and commercial farming as well as mining activities in the southern part of the district. The district has 31 administrative wards with 46 health facilities, 10 falling under government, 30 under Mutasa Rural District Council, and 6 under private. Pregnant adolescents/teenagers come for antenatal and post-natal care to these centers and some with are referred from the lower facilities.
Figure 1. Map of Mutasa highlighting the Study Four Hospitals.
A multi-methods comparative study design was used for this study. Qualitative (FGDs) and quantitative (Case-control) approaches were used to identify factors that are contributing to the rise in teenage pregnancies in Mutasa district.
Study Population
The study population were teenagers in Mutasa District who were attending Hauna, Bonda, Old Mutare and Tsonzo hospitals and also resided in the catchment areas of the four hospitals.
2.2.1. Definition of Cases and Controls
A case of teenage pregnancy was defined as a teenager aged 13-19 years who had given birth or was pregnant in the period 2018-2019 in Mutasa District and was booked for Antenatal Care (ANC), Postnatal Care (PNC) at any of the 4 hospitals. A control was defined as a teenager aged 13-19 years who resided within the same catchment area with the cases who had not yet had pregnancy in the period 2018-2019 in Mutasa District.
2.2.2. Inclusion Criteria
All 13-19 year-old pregnant females who resided in Mutasa district as from January 2018 to December 2019, attended ANC, delivered, or attending PNC at 4 hospitals who gave assent/consent and were willing to be included in the study were interviewed. All 13–19-year-old females who were not pregnant and resident in the catchment areas of the 4 hospitals under study were eligible as controls for the study. Traditional leadership (Headman/Kraal Head or their representatives), school heads, sister-in-charge and Non-Governmental Organisations (NGOs) officers dealing with teenagers from PLAN International and FACT found on duty during the days of data collection were interviewed.
2.2.3. Exclusion Criteria
Female teenagers aged 13-19 years old attending ANC or PNC and or delivered before January 2018 or after December 2019 and /or were not a resident of Mutasa District or not in the catchment of the 4 hospitals were excluded from the study. All registers with incomplete information were also left out of the study.
Sample Size and Sampling Procedure
The study sample was calculated using the formula
where
n = sample size
N = total population of teenagers who got pregnant in 2018-2019 in Mutasa district and
e = margin of error (10%).
Therefore the minimum sample size was
n = = 72.6 = 73 cases. Since we had an unmatched 1:1 case control study, 73 controls were also enrolled giving a total of 146 participants. We anticipated a refusal rate of 10%, so the maximum sample size was = 81.1 = 82 cases. Therefore, the study enrolled a maximum of 164 participants.
Sampling Procedure
There were four (4) out of 6 hospitals in Mutasa district which recorded teenage pregnancies or where the teenagers were referred to and admitted in the period 2018-2019. All the four hospitals were included in the study. The cases and controls were selected proportionally according to the number of teenage pregnancies recorded at each hospital as indicated in the table below:
Table 1. Distribution of Sampled Cases and Controls by Hospital.
Facility/Hospital | Teenage pregnancies | Cases | Controls |
Hauna | 96 | 30 | 30 |
Old Mutare | 49 | 15 | 15 |
Tsonzo | 57 | 18 | 18 |
Bonda | 63 | 19 | 19 |
Total | 265 | 82 | 82 |
Systematic random sampling was used to select participants at each and every hospital. Records of participants who fell pregnant in the period 2018-2019 at the four hospitals were arranged sequentially according to the dates admitted at the hospital. The sampling interval was calculated for each hospital by dividing the number of teenage pregnancies (N) by the sample size (n). The first participant was selected by rolling a die once and the number that appeared at the top was considered. Subsequent participants were selected by adding the sampling interval to the first and continued adding until reaching the required sample size. If the selected teenager refused to take part in the study, the next teenager in the line was selected and the sampling interval was added as usual. The controls were selected from the same area as the cases and the researcher went to the areas where the cases came from and looked for teenager in that area. Two FGDs with 10-12 cases and another with 10-12 controls were done to get a deeper understanding of the causes of teenage pregnancies in Mutasa district.
2.4. Data Collection Instruments
Interviewer administered questionnaires with both open and close ended questions were used to collect data from the teenagers including the Focus Group Discussion guide. The questionnaire had five sections: Section A covering the Demographic characteristics of the participants, Section B covered Knowledge factors, Section C covered cultural and religious factors, section D covered Socio-Economic factors while Sections E and F covered Sexual and Reproductive Health and Mass Media Exposures respectively. Another self-administered questionnaire for the Key Informants was used to collect data on factors causing teenage pregnancies in Mutasa district.
2.4.1. Dependent Variable
The outcome variable for the study was teenage pregnancy.
2.4.2. Independent Variables
Socio-demographic variables like age, sex, marital status, knowledge, education, occupation, and income were considered. History of sexual and reproductive health, like age at first sexual intercourse, early marriage, and contraceptive use, perception on teenage pregnancy, family income, family education, peer pressure, and casual sex were assessed.
2.5. Data Collection Procedure
Interviewer administered questionnaires were administered to the selected participants. After selecting the cases that would have come to the hospital for ANC services, the researcher travelled to their areas of residence and identified teenagers to interview. About 10-12 cases and controls were identified from the same registers and areas of residence of the cases to participate in the FGD at Mutasa Rural District Service Centre on a particular given date. The key informants were given the questionnaires to complete and other stake holders around the hospitals were identified and invited to take part in the FGDs. The questionnaires for both teenagers and key informants were checked for completeness and kept under lock and key accessible to the investigator only.
Pretesting of the instruments was carried out at Triashill and St Barbara’s Mission hospitals to check for validity and reliability of the tools. At least 16 participants were selected that is 10% of the sample size to take part in the pre-test. All the errors identified were corrected before the start of the actual study.
2.5.2. Validity and Reliability
Content validity was assessed through the use of literature on teenage pregnancy. Questionnaires were translated into the local language Shona and back translated them to English to check if they still had the same meaning. The researcher also had time to review the tools before and after pretesting. Reliability is the degree of consistence with which an instrument measures the variables of interest. This includes dependability, consistency, accuracy and comparability. In the study reliability was checked through the pretest. Consequently, the principal investigator administered all the questionnaires and avoided problems associated with interpreter reliability.
2.6. Data Organization and Analysis
Data was captured, and analyzed using Epi Info version 7. Univariate and bivariate analysis was performed to come up with factors that were statistically significantly associated with teenage pregnancies in Mutasa District. Content analysis was used for manual qualitative data analysis to develop themes.
2.7. Ethical Consideration
Permission to carry out the study was sought from the District Health Executive (DHE) Mutasa District, the Provincial Medial Directorate (PMD) Manicaland and Africa University Research Ethics Committee (AUREC). Respondents were assured that information they availed to the researcher was not divulged to anybody. Throughout the study the raw data was kept locked up to ensure confidentiality was retained. Codes were used to maintain anonymity. Participants were permitted to withdraw from the study any time they so wished without punishment or forfeiture of benefits.
3. Analysis and Results
Distribution of Participants According to Demographic Characteristics
Table 2. Distribution by Age Group, hobbies, marital status and level of education.
Age group | Case N=80 n (%) | Control N=80 n (%) |
13-15 | 35 (43.8) | 14 (17.5) |
16-18 | 45 (56.2) | 66 (82.5) |
Hobbies | | |
Reading books | 7 (8.8) | 32 (40.0) |
Socialising with friends | 46 (57.5) | 42 (52.5) |
Watching movies and pornographic materials | 27 (33.7) | 6 (7.5) |
Marital Status | | |
Single | 20 (25.0) | 3 (3.75) |
Married | 35 (43.75) | 65 (81.25) |
Divorced | 25 (25.0) | 12 (15.0) |
Level of Education | | |
None | 0 (0.0) | 0 (0.0) |
Primary | 72 (90.0) | 2 (2.5) |
Secondary | 8 (10.0) | 73 (92.4) |
Tertiary | 0 (0.0) | 4 (5.1) |
The majority of the participants were 16-18 years old for both the cases and controls. A good sizeable proportion 35 (43.8%) who participated in the cases was in the range 13-15 years. Contrary to the cases scenario a relatively fair proportion 45 (82.5%) of the controls participated in the study in the age group of 16-18 years.
The hobbies outlined were reading books, socialising with friends, watching movies and pornographic materials. More of the controls 32 (40.0%) than cases 7 (8.8%) had interests in reading books that would help fill up their time thus prevented them from activities like sexual intercourse that would render into teenage pregnancy. Socialising with friends received the greatest proportion from both the cases 46 (57.5%) and controls 42 (52.5%) purporting that it could have detrimental impact but with the controls potential parental/guardian moderation could be effected unlike to the cases. A good proportion of the cases 27 (33.7%) had their hobbies as watching pornographic materials with a meagre 6 (7.5%) in controls coming in.
The marital status variables included being single, married and divorced for the cases and controls who participated. More singles 20 (25%) were cases compared to 3 (3.8%) controls. Unlike the cases that had 35 (43.8%) parents as married, the controls were relatively more with 65 (81.3%). Divorce proportion was more in the cases 25 (25 %) than the controls 12 (15%).
The enrolled eighty cases and eighty controls participated to show their levels of education as none, primary, secondary and tertiary. The majority of the controls had reached secondary education 73 (92.4%) whereas most cases had only reached primary education 72 (90%).
Table 3. Distribution by parental education, parent status, and religion.
Mother’s Level of Education | Case N=80 n (%) | Control N=80 n (%) |
None | 8 (10.0) | 0 (0.0) |
Primary | 65 (81.3) | 4 (5.1) |
Secondary | 6 (7.5) | 27 (34.6) |
Tertiary | 1 (1.2) | 47 (60.3) |
Father’s Level of Education | | |
None | 3 (3.8) | 0 (0.0) |
Primary | 60 (75.0) | 0 (0.0) |
Secondary | 13 (16.2) | 50 (62.5) |
Tertiary | 4 (5.0) | 30 (37.5) |
Parent Status | | |
Child headed | 3 (3.8) | 0 (0.0) |
Live with both parents | 7 (8.8) | 44 (55.0) |
Live with one parent | 10 (12.5) | 35 (43.8) |
Single orphan | 60 (75) | 1 (1.2) |
Religion | | |
African Tradition | 4 (3.8) | 11 (13.9) |
Apostolic sects | 65 (82.3) | 0 (0.0) |
Orthodox | 11 (13.9) | 66 (83.5) |
Other | 0 (0.0) | 3 (2.5) |
Eight of the cases had mothers who had never gone to school whilst not even one control had a mother who had been to school. The majority 65 (81.3%) of the cases had mother who had gone as far as primary school level while 47 (60%) of the control’s’ mothers had tertiary level education. Only one case had a mother with the parental level of education has remarkable influence on the time one’s child can marry and who to marry.
All the eighty controls had their fathers in secondary and tertiary levels of education. Unlike the controls, the cases had their fathers having a normal distribution from being never at school and reaching tertiary level of education.
Availability of parent or both parents have a critical role in the rearing up of the teenager girl who remains target for sexual abuse. Of the cases enrolled in the study, their parental status indicated that the bulk 60 (75.0) were single orphans, child headed 3 (3.8), lived with both parents 7 (8.8) and lived with one parent 10 (12.5). Being child headed and single orphan constituted the greatest proportion of the cases who participated, overwhelmingly revealing how the group were rendered vulnerable by being ensued exposed by the unavailability of parents who both would help model the teenagers and ensure the provisions of the critical girl child prerequisites like sanitary pads. Having both parents available and around is an established protective factor as the teenager would be regulated and moderated against depraving.
Apostolic Sects were the greatest proportion as shown on the table that 65 (82.3% of all the cases were of the Apostolic Sects. Equally to the converse of the Apostolic Sect, the greatest proportion was also noted from the Orthodox Churches with 66 (83.5%) with the cases 11 (13.9%) under the same dimension. The Africa Tradition and Other Religion had the least contribution.
3.1. Economic Status of Participants and Exposure to Health Education
Table 4. Economic status of participants and exposure to health education.
Variable | Cases N=80 n (%) | Controls N=80 n (%) |
Receive Health education | | |
Always | 3 (3.8) | 39 (48.8) |
Sometimes | 16 (20.0) | 26 (32.5) |
Never | 61 (76.3) | 15 (18.8) |
Source of income | | |
Formal employment | 0 (0.0) | 0 (0.0) |
Informal employment | 10 (12.5) | 4 (5.0) |
Monthly allowances from parents/s | 11 (13.75) | 74 (92.5) |
Allowances from boyfriends | 59 (73.75) | 2 (2.5) |
The distribution of the response from the cases indicated that they did not always receive sex and reproductive health education, with the bulk never receiving. Over half of the controls indicated that they usually received some information of sex and reproductive health with 15 (18.8%) revealing that they had never received any. Relatively fair, as contrary to the cases the control received some information on sex and reproductive health that could help protect them from pregnancy vulnerability. Generally, the response indicated that they were unfilled gaps in the impartation of the critical information on sexual and reproductive health in Mutasa District.
Economic ambiences in which the girl child resides has strong bearing on the propensity for manipulation. The cases who participated reflected that there hosts of economic challenges that befell the teenage girls who obtained the critical monthly allowances mostly from boyfriends 59 (73.8%), with other allowances from parents 11 (13.8%) and informal employment 10 (12.5%). Favourably, the greatest proportions of the controls 74 (92.5%) received monthly allowances from their parents purporting the resource protection they got; unfavourably sizeable proportion pointed to informal employment 5 (5.0%) and allowances from boyfriends 2 (2.5%) amongst the controls.
Social Factors affecting Teenage Pregnancy in Mutasa District 2018-2019.
Social factors that affect the girl child into pregnancy were looked into. The
table 5 below reflects on the social dimension of age.
Table 5. Distribution According to Age of First Pregnancy by Religion.
Variable | Religion |
Age of first pregnant? | Orthodox | African Tradition | Apostolic |
| N=14 n (%) | N=3 n (%) | N=63 n (%) |
11-13 | 3 (21.4) | 1 (33.3) | 18 (28.6) |
14-16 | 6 (42.9) | 2 (66.7) | 43 (68.2) |
18+ | 5 (35.7) | 0 (0.0) | 2 (3.2) |
Of the enrolled cases and controls, the teenagers from the Apostolic Sects revealed that they had had their first pregnancy between 11-13 (28.6%) and 14-16 (68.2%) years and scarcely after 18 years. Although the Orthodox and African Tradition were affected in the same fashion, their proportions were relatively less.
Table 6. Number of girls in family married <18 years & age at first love affair.
Variable | Case N=80 n (%) | Control N=80 n (%) |
Number of girls in family married <18 | | |
0 | 8 (10) | 62 (77.5) |
1 | 13 (16.3) | 15 (18.7) |
2+ | 59 (73.8) | 3 (3.8) |
Age of first love affair | | |
<=10 | 0 (0.0) | 0 (0.0) |
11-13 | 40 (50.0) | 17 (26.6) |
14-16 | 38 (47.5) | 50 (62.5) |
17-18 | 2 (2.5) | 13 (28.8) |
18+ | 0 (0.0) | 0 (0.0) |
The bulk 40 (50%) of the cases unlike the controls 17 (26.6%) started love affairs between 11-13 years. Unlike the cases, the bulk of the controls 50 (62.5%) started love affairs between 14-16 years with the cases 38 (47.5%) in the same age. A few cases and controls started affairs between 17-18 years.
The sampled case teenage girls indicated that most of the girls 59 (73.75%) in their families married before the age of 18, purportedly due to early drop out from school compounded by the parental illiteracy or being materially handicapped or being exposed as double orphans.
Table 7. History of Domestic Violence and Age of Marriage in Mutasa 2018-2019.
Variable | Cases (N=80) n (%) | Controls (N=80) n (%) |
Age of Marriage | | |
Around 14-15 years | 42 (52.5) | 34 (42.5) |
Around 16-17 years | 23 (28.8) | 6 (7.5) |
Around 18 and over | 15 (18.8) | 40 (50.0) |
Exposure to Domestic Violence | | |
Always | 67 (83.8) | 3 (3.8) |
Regularly | 9 (11.2) | 6 (7.5) |
Never | 4 (5.0) | 71 (88.7) |
The participating case teenage girls revealed that they normally marry between the age of 14-15 years (52.5%) with the other spread between 16-17 years (28.8%) and over 18 years (18.8%). Half of the controls indicated that they married above 18 years.
The results of this study indicated that the majority 67 (83.8%) of cases experienced domestic violence within families whilst only 3 (3.8%) controls had always experienced domestic violence.
3.2. Sexual and Reproductive Health Services Affecting Teenage Pregnancy
Table 8. Family reaction to contraception use by adolescents and SRH service friendliness.
Variable | Case N=80 n (%) | Control N=80 n (%) |
What will be your family reaction when found with or using contraceptives | | |
Beaten | 27 (33.8) | 9 (11.3) |
Advised to use wisely | 12 (15.0) | 63 (78.8) |
Chased off home | 41 (51.3) | 8 (10.0) |
Services at the Youth Friendly Centres | | |
Youth games | 80 (100) | 51 (63.8) |
Testing and Counselling | 0 (0.0) | 21 (26.3) |
Pregnancy prevention education | 0 (0.0) | 8 (10.0) |
Abortion services | 0 (0.0) | 0 (0.0) |
Being beaten when found with or using contraceptives like condoms constituted 16 (20%) in cases and 9 (11.3%) in controls; advised to use wisely the contraceptives was noteworthy in controls with 63 (78.8%) while in cases was 12 (15.0%). More than half of the cases 41 (51.3%) than controls 8 (10.0%) who were found using contraceptives could be chased off home.
The Youth Friendly Centres play a variety of functions in sprucing the adolescents. The enrolled participants revealed the type of services they received at the scarce centres in the District 2018-2019. The cases who participated in the study indicated that they only received youth games at the centres and nothing else. The controls who participated indicated that they received youth games, testing and counselling sessions and pregnant prevention sessions.
Family reaction when delayed by a boyfriend
The eighty cases and eighty controls engaged in the study gave responses on family reaction when delayed by boyfriend or found with one.
Table 9 below gave the responses.
Table 9. Family Reaction When Delayed By a Boyfriend in Mutasa District 2018-2019.
Variable | Case N=80 n (%) | Control N=80 n (%) |
What will be your family reaction when delayed by boyfriend or found with one? | | |
Beaten | 16 (20.0) | 9 (11.3) |
Advised to be responsible | 15 (18.8) | 68 (83.8) |
Chased off home to the boyfriend | 49 (61.3) | 4 (5.0) |
Both the cases and the controls indicated that they would be beaten when delayed by boyfriend or found with one with the cases 16 (20%) and the controls 9 (11.3%). The greater percentage 68 (83.8%) being the controls highlighted that they would be advised wisely when delayed by boyfriend or found with one, quite smaller fraction 15 (18.8%) of the cases also mentioned the same.
3.3. Qualitative Findings
We conducted 3 FGDs, one with 12 cases, another with 12 controls and one with civil society members. We also had 8 Key Informant interviews (5 parents and 3 community leaders). The following themes came out of the study findings.
3.4. Family Structure and Dynamics Influence Prevalence of Teenage Pregnancies
Results from the FGD with cases revealed that child headed families facilitated teen pregnancy. One third of the cases in the FGD were from child headed families. They reported entering into transactional sex for survival due to extreme economic hardships. Teenagers who were sexually exploited were often dumped with babies and at times STIs. Similarly, belonging to an abusive family with high prevalence of gender-based violence predisposed teenagers to sexual violence. Such families forced teen girls to elope if found with a man in lone places or delay coming home. Some families were reported to facilitate teenage marriages with the elder sisters and mothers who married as teenagers encouraging their siblings to follow suit. Male predators were exploiting teens for small favours like providing money for sanitary pads. On the contrary, an FGD with control teenagers revealed that their families were quite supportive and nurturing. The families encouraged the teenagers to go to Youth Friendly centres and monitored the learning. It was discussed that the parents bore reservations that exposure of the teenager girls to contraceptive would increase promiscuity without bearing the conviction that it was a form of empowerment and fortification and only required periodic guidance. The focus group discussion revealed that as parents there was the need to cherish intimate dialogue with adolescent girls to help note their reproductive health concerns and work to resolve. It was highlighted that they was need to appreciate new realities like the controlled use of contraceptives. Male involvement was highlighted as critically fundamental other than just engage the teenager girls and rest of the females who were mere recipient of the undesirable fate of the uncensored male.
3.5. Lack of Comprehensive Sexuality Education for Teenagers
Knowledge gaps were noted as drivers of teenage pregnancies. Family members who periodically convened with the adolescents to articulate their sexual reproductive concerns had very slim chances of reporting teenage pregnancies. The control group indicated that routinely some of the adolescents were seconded to special reproductive health advisors. They indicated that in some churches, teenagers were talked to comprehensively and offered periodic sessions on reproductive health and the challenges emanating thereto. The control group acknowledged exposures to risk environments that could be detrimental, but they reported that knowledge aided them to navigate through without meeting much challenges. The civil society members FGD highlighted that teenage girls required persistent knowledge and empowerment with reproductive health knowledge and specialised institutions erected and sustainably managed. In schools, teenagers received scarce information and naïve attention on matters of pregnancy and reproductive health. A sizeable proportion of learners end school at primary level thus not well schooled in matters of reproductive health.
3.6. Access to Youth Friendly Centres and SRH Services is Protective Against Teenage Pregnancies
The control teenagers reported that teenagers were periodically made to visit Youth Friendly centres. It was noted that only ward 24 in Manica Bridge had the Youth Friendly Centres where the youth would meet and be empowered with essential sexual reproductive health services and all critical reproductive fundamentals. Failure of access to family planning services due to unfriendliness of service providers was highlighted as a big constraint. The seeker of the service would be labelled as promiscuous, thus resorting to unprotected sex. It was highlighted that teenagers were experimental in nature and the provision of contraceptives would help a great deal in mitigating teenage pregnancies.
3.7. Peer Influence Is a Key Determinant of SRH Outcomes Among Teenagers
The participants in the FGD for cases highlighted that peer influence was of great concern. Peers always need to mimic each other with little contemplation on consequences thus blindly follow one another. Friends had quite huge influence in matters of sex and sexuality. Full time engagement in school was protective against sexual engagements. It was stressed that peer friendship called for proper regulation to avoid bandwagon into moral debasement. Friends who had the sex and reproductive orientation protected one another and the converse applied to those who were ignorant.
3.8. Social Norms and Beliefs Expose Teenagers to Teen Pregnancies
It was reported that religious sects of the white garment did not observe majority age in marrying their girls. Girls are not prioritised for school and were married off to males normally in polygamous institutions. It was told that due to religious institutional indoctrination teenage girls cherished marriages and appreciated marriage as noteworthy achievement despite all forms of criticisms from fellow contemporaries. The type of church one went was a key determinant of the propensity to teenage pregnancy. Sects had the greatest challenges in teenage pregnancy episodes compared to orthodox churches that appreciated teenage sexual challenges and reality. Some orthodox churches were strict with matters of abstinence from premarital sex with full condemnation of contraceptives use like condoms which in turn rendered the teenagers prey to pregnancy whenever exposed. Teenager mothers were reported to deliver in secret spiritual maternity places. NGOs had established systems to facilitate the reporting of childhood marriage and sexual exploitation by the Community Case Workers (CCWs) but it was still hard for the community to take the matter on board due to cultural and tie issues. Challenges were noted with regards to how the Sect teenagers would be engaged as they had their firmly established and fortified Church doctrine that did not permit general interactions and any form of penetration into their doctrine.
3.9. Media Influence and Exposure Is Fuelling Teen Pregnancies
The discussion revealed that media exposures were pretty instrumental in prompting teenagers to engage in teenage fornication normally without protection. Teenagers who got pregnant were exposed to pornographic materials. Media influence and exposures were highlighted as some of the contemporary enablers for teenage pregnancy where technological devices like computers and cell phones had become universally accessible to teenagers of all age groups. It discussed that many communities were going through high moral degeneration as pornographic information was accessible free of charge via devices such as computers and cell phones/WhatsApp. Free access to pornographic material on the internet was also likely to propel teenagers into sexual curiosity.
4. Discussion
This study sought to determine factors associated with an increase in teenage pregnancies in Mutasa district in Zimbabwe. The study findings revealed that multiple factors contribute to teenage pregnancies in Mutasa district. Economic challenges amongst the host of other challenges retained the greatest blame. The unsuspecting juveniles suffered resource manipulation to fall prey to the male sex predators and greatly the victims to such were the child headed households, the teenagers who stayed alone, and those who came from impoverished households. The economic challenges noted concurred with
| [15] | Amnesty International. (2008). Report on adolescent sexual practices in Zimbabwe. Harare. |
[15]
who indicated that economic burdens well enablers to teenage pregnancies and marriages.
The levels of education do affect the propensity to fall into teenage pregnancy
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. When a teenager leaves school, the next likely encounter would be the aspiring teenage marriage. The cases engaged in the study indicated that 90% had just ended at primary level, with only 8 (10%) having reached secondary level with hardly anyone that reached tertiary level. Conversely, almost all the controls reached secondary level 73 (92.4%) and tertiary level 4 (5.1%) thus revealing how the level of education impact on teenage pregnancies and marriages. The portrayed scenario concurred with the findings under literature review
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
that empowering teenagers with education would enable reaping desirable dividends that excluded the vice of teenage pregnancies. Educated teenagers would remain circumspective against falling prey to manipulative tendencies of some male predators especially in some religious Sects.
The assertion of education as a protective factor was also revealed in the focus group discussions held in the District. It was highlighted in the focus group discussions that that some Sects let their especially girl child end school at primary level after which sooner than later would be exposed for teenage marriage. Preoccupation of the teenage girl with school would purport the desirable shift from mere costly idle moments that could be filled up by sexual encounters to self-empowerment. Unlearned mothers would ensue unlearned posterity who would rank sex and marriage ahead of self-development thus a vicious cycle. Educated mothers desire to have the teenage girl learn so that could be self-reliant in the future and to base livelihood on marriage the perspective of the unlearned mother, (Mfono, 2003).
Mother’s education is the form that firms or deforms the girl child’s future. An educated mother is a protective factor as she helps prevent teenage marriages and pregnancies. The table below reflect on the results given by the enrolled cases and controls on the level of education. Lack of continuity with education could be facilitating teenage marriages and pregnancies in Mutasa District. Father’s level of education like mother’s greatly influence the desire for immediate gratification and the zeal against strategic interests on the fate of the teenage girl. An uneducated parent treats the girls like an economic asset with dividends emanating from marriage which comes with the girl child’s uncontrolled self- intent or coerced to prematurely marry
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. World Vision also revealed that uneducated parent may cost the future of the girl child by rendering her to premature marriages and pregnancies
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[10]
.
Cultural and religious factors had remarkable bearing on teenage pregnancies and marriages
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[10]
. The findings from the study indicated that retrogressive religious practice of some Sects popular in the district like handpicking unsuspecting girl child to some men in the Apostolic Sects perpetuated teenage pregnancies and marriages in Mutasa District. Brown and colleagues also revealed that Apostolic Sects facilitated their daughters to marry early even to polygamous men due to religious beliefs orientation and affiliation
. Orthodox churches like Roman Catholic, Anglican, Methodist and Seventh Day Adventist seemed to be contributing less as most of the controls 66 (83.5%) came from the orthodox institutions. Retrogressive conservative cultural practices within some Sects retained some clandestine teenage girl marriages deals that would call for critical eye and probing to understand. Action for life and World Vision, 2020 were synoptic when they revealed that teenage marriages and pregnancies were rampant in the Apostolic Sects where attention for the girl child was minimal and most of the teenage girls ending school at primary level and wait to be married
| [19] | Action for Life. (2011). Zimbabwe key informants formative research report on young people engaging in sex and teen pregnancies. Institute for Environment, Health and Development Communication, Harare. |
[19]
. The findings also corresponded with echoed sentiments during the held focus group discussions, where it was highlighted that girl child hand picking was practiced with the church elders facilitating. Girl child rights were not retained and realised in some Sects unlike the Orthodox churches. World Bank and UNFPA noted that girl child in some Sects were treated as objects who only waited to be married and bear children
| [4] | World Bank. (2017). Economic impacts of child marriage: Global synthesis report. Washington. |
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[4, 8]
.
Media and exposures facilitated teenage pregnancies and marriages in a host of circumstances
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Exposure to pornographic materials, uncensored sex exhibitions, WhatsApp sex videos was implicated for sexual arousal which resulted in unplanned sexual encounters for teenage pregnancies and marriages. Some old females in communities were reputed for mediating and interceding for sexual relationships of the unsuspecting teenage girls where they received some dividends. Pornographic materials are precursor to sexual arousal which beget and enhance permissiveness
| [2] | World Health Organisation. (2018). Adolescent pregnancy fact sheet. Geneva. |
[2]
. UNFPA also concurred that exposure to sexual arousing materials prompt early sexual engagements that normal resulted in teenage pregnancies
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8].
Socialising with friends or peer influences and watching movies and pornographic materials could be influencing teenage pregnancies in Mutasa District as most of the cases indicated such the hobbies.
Social factors were implicated for the teen pregnancies and marriages challenges and ranged from family to community spectra
| [19] | Action for Life. (2011). Zimbabwe key informants formative research report on young people engaging in sex and teen pregnancies. Institute for Environment, Health and Development Communication, Harare. |
| [2] | World Health Organisation. (2018). Adolescent pregnancy fact sheet. Geneva. |
[19, 2]
. It was highlighted that teenage pregnancies and marriages could become a cyclic family or community practice, agenda and legacy. Females who would marry after 18 years would be treated as outlandish to the social and traditional practice in the locality thus coercing one to conform to marry as teenagers. Low parental level of education impacted negatively on the teenagers who were made to drop from school and thus pursue marriage young.
noted that parents who had some social handicaps were barriers and stumbling blocks to marital determination of the girl child where thus the teenage were made to marry in appreciation of others status quo. Families with legacy and practice of domestic violence were highlighted as on record of teenage pregnancies and marriages as the teenage would seek to evade the painful violence experience. Domestic violence and abuses were found to be prevalent in Mutasa District.
Studies by
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[8, 10]
revealed that family organisation whether or not the parents are singles, married or divorced was noted to be fundamental in sprucing the teenager girl.
also noted that an organised married couple would help shape the teenage girl than the single or divorced where the girl may not receive balanced control. Studies by
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
revealed girls exposed to singles or divorcees who had reckless sexual life were promptly graduated into sexual activities thus the potential for teenage pregnancies.
Denno, D. M. et al.
highlighted that many parents had the challenge to accept the children as they grew in every dimension thus stereotyping the children to the world of their interest that failed to tally with their of reality. Conservativism in the use of contraceptives by the teenagers was still rampant and also conducted focus group discussions indicated that the parents in Mutasa district did not favour their children to be exposed to contraceptives.
The parental marital status and the general behaviour of the parent may encourage or discourage the teenager to indulge in sexual activities or not. Single parents who may be wild with sexual activities would equally incidentally engage the teenagers. Equally to the fate of teenage pregnancy, married rife promiscuous parent may impact detrimentally to the on looking teenager. With regards to girls in family, married <18, The finding concurred with the findings by Brown and others who indicated that early teenage marriage would remain a cyclic legacy in some families. Unlike the experiences with the cases, the controls did not marry below the age of 18 years due to possible reasons like being in schools and thus preoccupied and being fortified by educated parents. The finding also concurred with what came out of the focus group discussions that the time one married legacy within families, with marrying early or late was being routine within the family.
The time one started love affairs also mostly directly affected the frequency of sexual encounters that would also determine falling pregnancy. The greater proportion of the enrolled cases indicated that they had started having affairs when they were aged between 11-13 and 14-16 years. This is the time when they would have a sundry of sexual encounters that would result in pregnancy as at the mentioned ages decision making would not yet have become consummate. At the age, sexual manipulation and exploitation would be rife with the teenagers mostly being made an object of sexual gratification
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Therefore early engagement in love affairs could be purporting as early engagement in sexual debuts that cost the cases with teenage pregnancy in Mutasa District.
The history of domestic violence was noted as bearing detrimental effects on the girl child as she had to seek means to evade the daily encounter. Several authors implicated domestic violence to teenage girl pregnancies and early marriages
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
| [11] | L'Engle, K. L., Brown, J. D., & Kenneavy, K., (2006). The mass media are an important context for adolescents' sexual behaviour. Journal of Adolescent Health, 38, 186-192. https://doi.org/10.1016/jadohealth.2005.03.020 |
[10, 11]
. World Vision thus castigated domestic violence as one the cardinal impetus propelling teenage girl pregnancies and marriages as they tended to evade the emotional trauma and stress that came with it
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[10].
The authors
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[8, 10]
clarified that when parents were engaged in domestic violence they hardly spared opportunity to attend to but rather developed indifference to the girl child concerns. Consequently the teenage girl would seek solace and placation from externals in the form of boyfriends who would take virtue out of her handicapped circumstances. Sexual abuses and exploitation would be executed without any notice prompting in the costly unintended pregnancies and marriages.
Conversely to the girl child experiencing domestic feuds, the girl child who would not encounter domestic chaos would be at liberty to express concerns to parents or guardian on her prerequisites without any chagrin. The self- articulation and being heeded to would enable the teenager girl to remain under the protective auspices of the parent or guardian thus regularly regulated against depraving into teenage pregnancy and marriages.
The revealed scenario confirmed the observation
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
that child pregnancy and marriages were consistently sustained in Zimbabwean society. The cited implications included school drop outs when after dropping from school cannot have any engagement other than focussing on marriage. It was a fact appreciated that the longer one remained in school the further delay in marriage and pregnancy.
Comprehensive Sexual reproductive health services with peculiar adolescents’ packages manned by experts were noted be a gap in the study. The teenagers did not get the critical services in their communities thus remained with unanswered questions whose result included blind sexual engagements leading to teenage pregnancies and marriages. The finding confirmed the finding UNFPA that the unavailability and absence of a comprehensive Youth Friendly services would be catastrophic
| [8] | United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York. |
[8]
. Information is power and an empowered teenage girl can outwit adverse manipulative tendencies that would render her into teenage pregnancy
| [4] | World Bank. (2017). Economic impacts of child marriage: Global synthesis report. Washington. |
[4]
. The reception of scant sex and reproductive health to the adolescent girls purport a costly shortfall that could render the teenage exposed and therefore gullible to any form of manipulation leading to the event of teenage pregnancy
| [11] | L'Engle, K. L., Brown, J. D., & Kenneavy, K., (2006). The mass media are an important context for adolescents' sexual behaviour. Journal of Adolescent Health, 38, 186-192. https://doi.org/10.1016/jadohealth.2005.03.020 |
| [10] | World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala. |
[11, 10]
.
5. Conclusion
In conclusion, this study sheds light on the multifaceted factors contributing to teenage pregnancy in Zimbabwe. It underscores the importance of comprehensive interventions addressing socio-economic, educational, and cultural determinants to mitigate this complex issue. By understanding and addressing these factors, policymakers and stakeholders can work towards empowering Zimbabwean youth with the knowledge and resources necessary for making informed decisions about their reproductive health, thereby fostering a brighter future for the nation.
Abbreviations
ANC: Antenatal Care
AUREC: Africa University Research Ethics Committee
DHE: District Health Executive
FGD: Focus Group Discussion
PMD: Provincial Medical Director
PNC: Post-natal Care
SRH: Sexual and Reproductive Health
UNFPA: United Nations Fund for Population Activities
WHO: World Health Organisation
Author Contributions
Maxwell Joshua Moyoweshumba: Writing - original draft
Elliot Chikaka: Supervision
Maxwell Mhlanga: Formal Analysis, Methodology, Writing - review & editing
Munyaradzi Mukuzunga: Supervision
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
United Nations Population Fund. (2013). Girlhood, not motherhood: Preventing adolescent pregnancy. New York.
|
| [2] |
World Health Organisation. (2018). Adolescent pregnancy fact sheet. Geneva.
|
| [3] |
World Health Organization. (2014). Adolescent pregnancy fact sheet.
http://www.who.int/mediacentre/factsheets/fs364n
|
| [4] |
World Bank. (2017). Economic impacts of child marriage: Global synthesis report. Washington.
|
| [5] |
Aigbe, G. O., & Zannu, A. E., (2000). Differentials in infant and child mortality rates in Nigeria: Evidence from the six Geopolitical zones. International Journal of Human Social Sciences, 2(16), 206-214.
http://www.ijhssnet.com/journals/Vol_2_No_16_Special_Issue_August_2012/22.pdf
|
| [6] |
Neal, S. E., Chandra-M, V., & Chou, D., (2015). Adolescent first births in East Africa: disaggregating characteristics, trends and determinants. Reproductive Health Center, Dar es Salaam.
|
| [7] |
Zimbabwe National Statistics Agency. (2015). Zimbabwe multiple indicator cluster survey 2014, Final Report. Harare.
|
| [8] |
United Nations Populations Fund. (2013). Motherhood in childhood: Facing the challenge of adolescent pregnancy, New York.
|
| [9] |
Mfono, Z., (2003). Focus on women in development: Parents and the teenage pregnancy crisis in South Africa. University of Pretoria, Pretoria.
https://doi.org/10.1177/0907568203104003
|
| [10] |
World Vision (2020). COVID 19 aftershocks: Teenage pregnancy on the rise in refugee resettlements, Kampala.
|
| [11] |
L'Engle, K. L., Brown, J. D., & Kenneavy, K., (2006). The mass media are an important context for adolescents' sexual behaviour. Journal of Adolescent Health, 38, 186-192.
https://doi.org/10.1016/jadohealth.2005.03.020
|
| [12] |
Anda, R. F., Felitti, V. J., Chapman, D. P., Croft J. B., Williamson, D. F., Santelli J., Dietz, P. M., Marks, J. S., (2001). Abused boys, battered mothers, and male Involvement in teen pregnancy. USA: Paediatrics Atlanta Georgia.
https://doi.org/10.1542/peds.107.2.e19
|
| [13] |
World Health Organization. (2011). Guidelines for preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. Geneva.
|
| [14] |
Acharya, D. R., Bhattaria, R., Poobalan, A. S., Van Teijlingen, E., & Chapman, G. N., (2007). Factors associated with teenage pregnancy in South Asia: A systemic review. United Kingdom: E-prints Bournemouth.
http://www.hsj.gr/volume4/issue1/402.pdf
|
| [15] |
Amnesty International. (2008). Report on adolescent sexual practices in Zimbabwe. Harare.
|
| [16] |
Anthony, M. O., Primus, C. C., & Stephen, L., (2019). Predictors of teenage Pregnancy among girls aged 13–19 years in Uganda: A community based-case control study, Uganda, Makerere University. Kampala.
https://doi.org/10.1186/s12884-019-2347-y
|
| [17] |
Kearney, M., & Levine, P., (2012). Why is the teen birth rate in the United States so high and why does it matter? Maryland, New York.
https://doi.org/10.1257/jep.26.2.141
|
| [18] |
Denno, D. M., Hoopes, A. J., & Chandra-Mouli, V., (2015). Effective strategies to Edinburgh: Child and adolescent. London: Health Research, Unit University of Edinburgh, London.
https://doi.org/10.1016/j.jadohealth.2014.09.012
|
| [19] |
Action for Life. (2011). Zimbabwe key informants formative research report on young people engaging in sex and teen pregnancies. Institute for Environment, Health and Development Communication, Harare.
|
Cite This Article
-
APA Style
Moyoweshumba, M. J., Chikaka, E., Mhlanga, M., Mukuzunga, M. (2024). Factors Associated with Teenage Pregnancy in Mutasa District, Zimbabwe. Central African Journal of Public Health, 10(2), 130-144. https://doi.org/10.11648/j.cajph.20241002.18
 Copy
|
Copy
|
 Download
Download
ACS Style
Moyoweshumba, M. J.; Chikaka, E.; Mhlanga, M.; Mukuzunga, M. Factors Associated with Teenage Pregnancy in Mutasa District, Zimbabwe. Cent. Afr. J. Public Health 2024, 10(2), 130-144. doi: 10.11648/j.cajph.20241002.18
Copy
|
Download
AMA Style
Moyoweshumba MJ, Chikaka E, Mhlanga M, Mukuzunga M. Factors Associated with Teenage Pregnancy in Mutasa District, Zimbabwe. Cent Afr J Public Health. 2024;10(2):130-144. doi: 10.11648/j.cajph.20241002.18
Copy
|
Download
-
@article{10.11648/j.cajph.20241002.18,
author = {Maxwell Joshua Moyoweshumba and Elliot Chikaka and Maxwell Mhlanga and Munyaradzi Mukuzunga},
title = {Factors Associated with Teenage Pregnancy in Mutasa District, Zimbabwe
},
journal = {Central African Journal of Public Health},
volume = {10},
number = {2},
pages = {130-144},
doi = {10.11648/j.cajph.20241002.18},
url = {https://doi.org/10.11648/j.cajph.20241002.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20241002.18},
abstract = {Teenage pregnancies are a global problem mainly in marginalised communities resulting in complications, societal rejection and deaths. In Zimbabwe, 48% of the teenage pregnancies occurred between 13-19 years. Mutasa District, one of the Districts in Zimbabwe has high rate of teenage pregnancies. Teenage abortions rose from 3/1000 in 2018 to 5/1000 in 2019. We conducted a study on the factors associated with teenage pregnancies in Mutasa District in the year 2018 and 2019. The specific objectives were to determine the prevalence of teenage pregnancies, to determine the sociocultural, economic and religious factors influencing teenage pregnancies and to assess the availability and utilisation of Adolescent Sexual and Reproductive Health Services. A multi-methods+ study design was used with a sample size of 80 cases and 80 controls from four hospitals in Mutasa. Systematic sampling was employed where every 3rd subject was systematically selected upon satisfaction of the inclusion criteria, with sampling interval observed. A quantitative survey and Focus Group Discussions (FGDs) were used to collect data. The results showed that 72 (90%) of the cases only had primary school education. Being single orphans 60 (75%), having information and education gaps 77 (96.3%), being chased off home to go to the male partner 49 (61.3%) were the prevalent factors linked to teenage pregnancies. Having been disciplined when found with contraceptives led to 41 (51.3%) of the pregnancies. Having the boyfriend as a source of livelihood allowances contributed to 59 (73.8%) of teenage pregnancies while being a member of an Apostolic Sect contributed 65 (82.3%) of the cases. The FGDs revealed that the Youth Friendly Centres were inadequate for the community, poorly resourced having no comprehensive preventive services and therefore poorly utilised. In addition, teenage pregnancy preventions were stereotyped to females only with current interventions being predominantly reactionary than preventive. The findings of this study suggest the need for reproductive health information, gender inclusive programming, and provision of a sundry of well-resourced Youth Friendly Centres in the District and a focus on tailor-made preventive interventions rather than punitive ones.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Factors Associated with Teenage Pregnancy in Mutasa District, Zimbabwe
AU - Maxwell Joshua Moyoweshumba
AU - Elliot Chikaka
AU - Maxwell Mhlanga
AU - Munyaradzi Mukuzunga
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.cajph.20241002.18
DO - 10.11648/j.cajph.20241002.18
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 130
EP - 144
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20241002.18
AB - Teenage pregnancies are a global problem mainly in marginalised communities resulting in complications, societal rejection and deaths. In Zimbabwe, 48% of the teenage pregnancies occurred between 13-19 years. Mutasa District, one of the Districts in Zimbabwe has high rate of teenage pregnancies. Teenage abortions rose from 3/1000 in 2018 to 5/1000 in 2019. We conducted a study on the factors associated with teenage pregnancies in Mutasa District in the year 2018 and 2019. The specific objectives were to determine the prevalence of teenage pregnancies, to determine the sociocultural, economic and religious factors influencing teenage pregnancies and to assess the availability and utilisation of Adolescent Sexual and Reproductive Health Services. A multi-methods+ study design was used with a sample size of 80 cases and 80 controls from four hospitals in Mutasa. Systematic sampling was employed where every 3rd subject was systematically selected upon satisfaction of the inclusion criteria, with sampling interval observed. A quantitative survey and Focus Group Discussions (FGDs) were used to collect data. The results showed that 72 (90%) of the cases only had primary school education. Being single orphans 60 (75%), having information and education gaps 77 (96.3%), being chased off home to go to the male partner 49 (61.3%) were the prevalent factors linked to teenage pregnancies. Having been disciplined when found with contraceptives led to 41 (51.3%) of the pregnancies. Having the boyfriend as a source of livelihood allowances contributed to 59 (73.8%) of teenage pregnancies while being a member of an Apostolic Sect contributed 65 (82.3%) of the cases. The FGDs revealed that the Youth Friendly Centres were inadequate for the community, poorly resourced having no comprehensive preventive services and therefore poorly utilised. In addition, teenage pregnancy preventions were stereotyped to females only with current interventions being predominantly reactionary than preventive. The findings of this study suggest the need for reproductive health information, gender inclusive programming, and provision of a sundry of well-resourced Youth Friendly Centres in the District and a focus on tailor-made preventive interventions rather than punitive ones.
VL - 10
IS - 2
ER -
Copy
|
Download