Abstract
Infant oral mutilation (IOM) is a harmful traditional practice of gouging out the unerupted developing infant primary teeth, usually the canine bud. It exposes immediate and long-term direct health effects, including bleeding-led anemia, septicemia, tetanus, osteomyelitis, meningitis, or even HIV as a result of unsterile tools. Given that, the general objective of the study was to assess infant oral mutilation in Garowe, Somalia. The research employed an analytical cross-sectional design that utilized both qualitative and quantitative approaches. Both probability and non-probability sampling techniques were simultaneously used. Initially, the Garowe district was purposively selected as the study area. Subsequently, a cluster sampling method was applied to identify seven of the most frequently visited health centers out of the twelve registered in the district. Then, a convenience sampling technique was used to recruit 140 children and infants who visited the facilities earliest, along with their mothers, for oral health examinations and interviews, respectively. Additionally, non-probability purposive sampling was utilized to select two dental doctors practicing in Garowe and two traditional practitioner healers practicing in IOM. Furthermore, a gender-representative focus group discussion (FGD) was conducted with community members to gather qualitative insights and cross-check the information. The study found that only 45 (32.1%) children were not gauged out, while 95 of the studied 140 participants were orally mutilated, making up an IOM prevalence of 67.9%, with the majority of them (62.2%) mutilated at the lower canine and 5% at the upper canine, whereas the mutilation features at both canines were found only in 0.7% of the studied children and infants. The study identified that various tools, often unsterilized, are used for the practice, such as an awl, alongside scissors and knives, while some traditional healers have medical surgical kits. In terms of risk factors associated with IOM, the study reveals that the primary motivation for IOM practice stems from linking tooth extraction to alleviating common childhood illnesses, especially diarrhea and fever. There was no significant association between IOM prevalence and factors such as age or gender of the children, maternal age, family income, or parental education. However, a significant association was found between IOM and abnormal dental conditions like missing or malformed teeth. The findings indicate that the prevalence of IOM in Garowe is alarmingly high, suggesting the urgent need for awareness and educational interventions to address the misconceptions surrounding IOM and its health implications.
|
Published in
|
Central African Journal of Public Health (Volume 11, Issue 3)
|
|
DOI
|
10.11648/j.cajph.20251103.14
|
|
Page(s)
|
135-144 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Prevalence, Infant, Oral, Mutilation, Garowe, Somalia
1. Introduction
1.1. Background of the Study
Infant oral mutilation (IOM) is harmful traditional practice of gouging out the un-erupted developing infant primary teeth usually canine bud
. It is commonly practiced in East African countries as remedy for infantile illness
| [2] | Amare, T. (2019). The Dental complications of canine tooth bud removal in 2-12 years old children in north west Ethiopia. Research square, 4 (1-17). https://doi.org/10.21203/rs.2.13352/v4 |
[2]
There is an accepted myth that extracting infant tooth bud is a cure for undefined febrile, and diarhealdisease
| [3] | Arthur, M. K. (2015). Raising the awareness of infant oral mutilation - myths and facts. Contemp Clin Dent. |
[3]
.
As the toothing primary dentition projection is more paler than the other areas, the triditional healers percieve as maggot in the jaw ridge predisposing ilness, the traidtional healers use extracted teeth bud appearnce of milk like to justify their skill and show the parent to convince the worthiness of the practice
.
This process of teeth extermination is always carried out by un trained individual with unsterilized tools i.e. knives and blades. Hence, it increases the risk of infection and damage to adjucent areas
| [5] | Global Child Dental Fund. (2018, February). End infant oral mutilation. Retrieved Noverber 20, 2019, from https://www.endiom.org/ |
[5]
The worst complications predisposed by this produre to unconsented infants can be categorized to an immediate impacts such as profuse bleeding, infection i.e. HIV&Meningitis as well as the likleyhood worsening of the pre-existing ilness and long terms side effects including missing teeth, teeth deragement, malformation, odontom along many others
| [6] | Hassanali J and Kibet P. (2014, September). Complex Factors Associated with Illnesses and Oral Mutilation in a “Vulnerable” African Infant. Austin Journal of Anatomy, 1-2. |
| [1] | Margaret N. W and Betsy. K.. (2017, juley). “Ebinyo”—The Practice of Infant Oral in Uganda. (T. Tiwari, Ed.) Frontiers in Public Health. https://doi.org/10.3389/fpubh.2017.00167 |
[6, 1]
.
Based on the geography, the identification of this practice has been used for many terms inlcluding IOM, canaine bud removal, tooth extirpation, dental mutilation, killer canine extraction as well as ibniyo and ilkow in Uganda and Somalia respectively
| [2] | Amare, T. (2019). The Dental complications of canine tooth bud removal in 2-12 years old children in north west Ethiopia. Research square, 4 (1-17). https://doi.org/10.21203/rs.2.13352/v4 |
| [3] | Arthur, M. K. (2015). Raising the awareness of infant oral mutilation - myths and facts. Contemp Clin Dent. |
| [4] | Jonathan, G. (2017). Dentaid impact document for IOM. www.Dentaid.org |
[2-4]
.
Historically, the first documented case related to IOM has been reported in 1932 in pagan tribes of the Nilotic Sudan as linked to cultural practice
| [7] | Seligman CG, Seligman BZ. Pagan Tribes of the Nilotic Sudan. Published by George Routledge & Sons Ltd. 1932. |
[7]
.
Since that time, this barbaric practice has been unveiled and reported in africa maily the eastern countries affecting about 2.5 million per yearr with prevalence rates of 22% in Sudan, 17.2% in Uganda, 37.4% in Tanzania and 30% in Ethiopia
Notwithstanding, the health importance of IOM was largely ignored as most governmental and health institution are unware to this selint menace.
As result of migration in recent years, the number of children presenting post IOM signs increased in western world and even other continents which tridationally had not known this practice. Hence, IOM emerged as global issue and the need for urgent action to end IOM become inevetable (Ibid).
Regarding Somalia, given the international calls to end IOM, the issue is grossly missed lacally and the IOM practice has not been adressed yet in the country. However, limited studies has revaled high prevalnece in Somali imigrants in USA and UK
| [9] | Rodd HD and Davidson LE. (2000). 'Ilko dacowo:' canine enucleation and dental sequelae in Somali children. Int J Paediatr Dent, (4): 290-7. |
[9]
but similarly to other countries, there is assumtion that IOM is as rampant as Female Genital Mutilation
. Therfeore, this study will address IOM first time in the country.
1.2. Statement of the Problem
Infant oral mutilation is one of bad traditional health practices that expose health hazard to incocent infants and children. IOM has immediate and long term direct effects, the victim infants which udergone this procedure eventually face serious complication including bleeding led anemia as well as septicemia, tetanus, osteomyelitis, meningitisor even HIV as a result of unsterile tools
| [3] | Arthur, M. K. (2015). Raising the awareness of infant oral mutilation - myths and facts. Contemp Clin Dent. |
[3]
. Additionally, malformation, non-eruption, hypoplasia, dysplasia, missing teeth may appear lately, it also worsens the pre-existing illness
.
The IOM is among the most challenging harmful health practice that young children face in African, it is mainly practiced in east Afrcan countries
. It has also become a major concern in the other world as a result of the movement of people from areas where the practice is rampant to areas where this is unheard
| [3] | Arthur, M. K. (2015). Raising the awareness of infant oral mutilation - myths and facts. Contemp Clin Dent. |
[3]
. In Somalia, the practiced of IOM have not been researched yet in the country but 31% of surveyed 260 somali children in Sheffield, UK exhibited features suggestive of a previous history of IOM, among them 5% were missing the lower permanent incisors
| [9] | Rodd HD and Davidson LE. (2000). 'Ilko dacowo:' canine enucleation and dental sequelae in Somali children. Int J Paediatr Dent, (4): 290-7. |
[9]
. another three somali children in USA was found they undergone this practice before moving from their home country
| [10] | Egbert, E. A. (2000). Dental injuries due to African traditional therapies for diarrhea. Western Journal of medicine, 135–137. |
[10]
.
Apart from these sugestive findings, there is no single research conducted in the country thus it is not sure whether the above prevalence similarly exists in the country or the pracice is more ominous than reported ouside the country. The reason behind the practice in Somali community and the ways they carry out are not yet scientifically addressed. Hence this research will serve as pioneering study to undcover the practice of IMO in the country.
Albiet, the IOM data is limited in all Somali regions, as Garowe is peaceful capital city hosting multi bacground community plus the time and const contrains, this city was used to serve as litmus paper for other Somalia’s regions in this research.
1.2.1. General Objectives of the Study
The general objective of the study is to assess the Infant Oral Mutilation in Garowe, Somalia.
1.2.2. Specific Objectives
The specific objectives of the study are:
1. To examine the prevalence of infant oral mutilation in Garowe district.
2. To describe how Gauging out canine teeth buds is carried out in Garowe.
3. To identify the risk factors behind IOM in Somali society.
4. To assess the impact of IOM on children and infants.
Research Questions
1. What is prevalence of Infant oral mutilation in Garowe?
2. How gauging out of teeth buds is carried out in Garowe?
3. What are the risk factors behind IOM in Somali society?
4. What is the impact of IOM on children and infants?
2. Methodology
2.1. Study Design and Setting
Cross-sectional study design was meticulously conducted both qualitative and quantitative approach at the Garowe health centers in Garowe, Somalia, Garowe, capital city of Puntland Somalia, is located in the northeast Somalia 785 Km distance away from the Mogadishu capital city of Somalia.
2.2. Participants Selection and Sample Size
This study focused on infants and children aged between 4 months up to 7 years, acknowledging this critical period of oral mutilation practices.
The sample is the subset of the population being studied; from which actual data is collected. On the other hand, sample size denotes the number of study participants for those particularly is considered for selection. The sample size is influenced by many different factors, including but not limited to the purpose of the study, population size, time, cost, the risk of selecting a bad sample, and the allowable sampling error
| [11] | Israel, G. D. (1992). Determining the sample size. Orlando: Florida University. |
[11]
. In addition to that,
recommended that if the target population is unknown but is assumed that it is more than 10,000 the Cochran’s standard formula is applied to increase representativeness.
Therefore, since the total infant and children in Garowe are not known, by considering all of these factors the above-mentioned Cochran’s formula was used to determine the sample size of this research which is
Which is
Where n= the desired sample,
Z= the standard normal variable at the required level of confidence,
P= the proportion in the target population assumed to have a specific characteristic,
e= the margin of error.
To calculate the sample size, one indicator of the previous survey was extracted from the Somalia children in Sheilf UK which 31% of children have experienced OIM. Thus, P=31% and 1-p =0.69 in this study 93% of confidence level was considered and corresponding normal standard value will be 1.81 hence Z=1.81 and margin of error was 0.5 thus the sample size of this study will be given by n=Z2 p(1-P) ∕e2 which is 1.812 (0.31) (0.69) ∕0.072 = 143. The sample size was allocated to target areas.
2.3. Sampling Procedure
The study employed a mixed-methods sampling approach, utilizing both probability and non-probability sampling techniques. Initially, the Garowe district was purposively selected as the study area. Subsequently, a cluster sampling method was applied to identify seven of the most frequently visited health centers out of the twelve HCs registered in the district. From these selected health centers, a convenience sampling technique was used to recruit 143 children and infants who visited the facilities earliest, along with their caregivers or mothers, for interviews and oral health examinations respectively. However, 140 respondents were successfully attained.
Additionally, non-probability purposive sampling was utilized to select two dental doctors practicing in Garowe and two traditional practitioner healer practicing IOM. Furthermore, gender-representative focus group discussion (FGD) was conducted with community members to gather qualitative insights and cross check the information. This multi-stage sampling strategy ensured a comprehensive and representative data collection process.
The list of Selected Health Centers
Health center name Number of visitors attained
Gambool Health: 20
Waabari: 21
Barwaaqo: 20
Gargaar: 22
Jillab: 20
Baxnaano: 19
Daryeel: 18
Total: 140
2.4. Data Collection Tool and Procedure
English questionnaires version was developed and data was collected through an interviewer administered questionnaires by data collectors. It was translated in to Somali language and after collection and translated back to English to check for consistency by experts. In addition, the main data collection, pre-test was conducted on thirty-five children from Garowe households that had no chance to participate in the main study on children who was characteristically similar to the participant ones. Pre-test was used to improve the precision, reliability, and validity of data. Following the analysis of the pretest outcome, ambiguous or unimportant questions was removed and unclear statements were rephrased based on identified problems and omissions. The time required for data collection was also determined and used for further data collection planning.
2.5. Data Quality Assurance
The data will be collected by trained data collectors which was provided the best opportunities to ensure the quality of data. After data collection, each questionnaire coded with a unique code by the principal investigator. The principal investigator was prepared the template and directly entered data in to SPSS version 21. Data was explored to check for missed values and outliers. Any errors identified at this time was corrected after revision of the original data using the code numbers.
2.6. Data Analysis
Data was cleaned for inconsistencies and missing values and was analyzed used SPSS version 21 statistical software. Frequencies and cross tabulations were computed for description of the study population in relation to socio-demographic and other relevant variables. The results will be presented in the form of tables, figures and summary statistics. Furthermore, logistic regression model was used in order to identify the most significant explanatory variables related to the dependent variables.
2.7. Ethical Consideration
Prior to beginning the study, the research ethics review committee of the Admas University provided ethical approval with reference number AUEA-109. All methods were carried out in accordance with relevant guidelines and regulations. Furthermore, the study was conducted with the principle of anonym and informed consent was obtained from all subjects and/or their legal guardian(s). To preserve the participants’ privacy, the confidentiality of the information acquired from them was strictly maintained throughout the study. Furthermore, participants were told of the future implication of their individual results at the start of the study to assure the transparency and adherence to ethical guidelines.
3. Data Presentation, Analysis and Discussion
3.1. Response Rate
140 respondents have been achieved out of 143 expected participants that means 98% of the expected participants were successfully studied. The rest 3 participants have not been reached. The 98% response rate indicated successfully engagement of the participants and appropriateness of the data collection methods. additionally, as it is the first research of its kind established in any area in Somalia, it is expected to serve as bench mark for future data studies.
3.2. Demographic Characteristics of the Respondents
As shown in the above table, 15.6% of the studied participants were less than six-month-old, the largest proportion of about 76.6% were between 6 to 59 moth of age meaning less than five years of age and greater than 6 month of infancy age while small portion of 7.1% of the research subjects were greater than five years age. This indicates that 6 to 59 months aged children are most commonly brought once for Health center service. The age of mutilation is mainly reported in the first 6 months for all age brackets. However, all age brackets were studied as main focus of the research was to establish the prevalence of the mutilation in the whole life time of the infants and children.
On the other hand, the majority of the infants 98.6% born in urban areas whereas only 1.42% of them equaling 2 persons born in rural areas meaning they are recently brought in the urban site of the study.
The possible relationship between the age and prevalence was cross-tabulated and tested using a Pearson Chi – square to assess whether the age has an effect on prevalence level of the participants. Hence, as shown in
table 1, the has not found significant difference as the P- value 0.683 in the Chi-Square is greater than the established margin of error of 0.07. For this reason, the age has no effect on the IOM prevalence in the studied participants. Meaning that the young and quite older once were mutilated similarly in their infancy stage.
3.2.1. Gender of Surveyed Infants and Children
Table 1. Demographic characteristics.
| Category | Frequency | Percentage | P- Value |
Age of the children &infants | <6 Month | 22 | 15.6% | 0.683 |
6 -59 Month | 108 | 76.6% |
>59 month | 10 | 7.1% |
Total | 140 | 100% |
Place of birth of child/infant | Urban | 138 | 98.6% | - |
Rural | 2 | 1.42% |
Total | 140 | 100% |
Gender | Female | 70 | 50% | - |
Male | 70 | 50% |
Total | 140 | 10% |
Age of the mothers/ care givers | <20 years | 12 | 8.6% | 0.145 |
20-30 years | 85 | 60.7% |
>30 years | 43 | 30.7% |
Total | 140 | 100% |
Family Income | < $200 | 81 | 58% | 0.462 |
> $200 | 59 | 42% |
Total | 140 | 100% |
Education level of mothers | Illiterate | 57 | 40.71% | 0.814 |
Primary | 52 | 37.1% |
Secondary and above | 31 | 22.1% |
Total | 140 | 100% |
Source: Field Survey, 2024 |
The gender of the studied infant and children was in balance, each gender represented half of the studied participants corresponding to 50% in both sexes (see
table 1). This equal number of male and female admissions in the health centers might suggest that factors influencing access to healthcare (e.g. cultural preferences on specific gender) are not significantly skewed towards one gender. Additionally, no significant association was found between the gender identity and IOM prevalence in the studied infants and children meaning that gender categories are similarly mutilated in the community.
3.2.2. Age of Mothers
The study has interviewed the mothers of infants and children in Health centers, a 60.7% of these participants were between 20 to 30 years of age, 30.7% were greater than 30 years and only 8.6% were less than 20 years of age. Therefore, the majority of Health attendants were 30 to 40 years age brackets. On the other hand, no association was found between the age and the prevalence of IOM among their children and infants as shown by the chi-square test 0.145 in
table 1 compared with the assumed 0.07% of marginal error. The absence of association, implies that the young mothers and old mothers have no different awareness revealing no new knowledge and awareness gaining by the community generations to challenge the old traditional practice of infant mutilation.
3.2.3. Family Income
To assess the possibility of economic challenge that may force parent to opt to traditional treatment or information gap in social classes related to access to resources the study assessed the income level of 140 families, the majority of the studied parents, 58%, were economically earning less than two hundred per month while the remaining portion of 42% were receiving greater than 200 USA dollar per month. This indicates, that majority of the community lives in precarious economic condition. However, no association was found between income level and IOM practice in the Pearson Chi-Square test (0.462) shown in
table 1.
In generally, thought, the economic conditions of families significantly differ, with a majority earning below $200 per month, this economic factor does not appear to be related to the prevalence of infant oral mutilation practices, implying that rampant prevalence of the practice regard less of the economic status of the parents.
3.2.4. Education of Mothers
The below data set reflects the educational attainment levels of the studied respondents and the individual categories are listed alongside their corresponding frequencies and percentages as following.
The education of mothers has shown substantial level of illiteracy and limited higher education attainment, the largest portion of the participants, 40.7% was illiterate. The second largest group of 37.1% were primary levels. Edgingly, 22.1% out of the 140 participants reached in secondary level or above. The overall data indicated an education gap. However, whether the education difference has association with the prevalence was cross tabulated as following and discussed below.
As shown in
table 1, there were no association between the education level and the practice of IOM. No difference was found between the highest indicated group and lowest illiterate group indicating; how prevalent the IOM is in the community and; how the common sense of the society is vastly tolerant to this practice irrespective of the education level.
3.3. Prevalence of Infant Oral Mutilation in Garowe District
The prevalence of infant oral mutilation is meant to address and count down the total number of children that have been removed their teeth for the purpose of ilkow and this has been measured through counting the mutilated children and infants then the type and scope of mutilation was also studied to enrich the prevalence information.
As the
table 2 data reveals, only 45 (32.1%) children were not gauged out while 95 of the studied 140 participants were orally mutilated, making up an IOM prevalence of 67.9%. comparatively, this prevalence is more than twice over the findings of previous research in Sheffield, UK which reported 32% out of 260 somali children survyed in there
| [9] | Rodd HD and Davidson LE. (2000). 'Ilko dacowo:' canine enucleation and dental sequelae in Somali children. Int J Paediatr Dent, (4): 290-7. |
[9]
. This is propabably due to their distance from the concentrated caltural area. Additionally, as per the available reports, it is the highest prevalence ever reported in the world approximated by a 60% prevenlence of ethiopian immigrants in Israel
| [13] | Esti Davidovich, E. K. (2013). The traditional practice of canine bud removal in the offspring of Ethiopian immigrants. BMC Oral Health. |
[13]
.
Table 2. Prevalence of IOM practice.
| Category | Frequency | Percentage |
Response to the practice of IOM | Mutilated | 95 | 67.9% |
Not mutilated | 45 | 32.1% |
Total | 140 | 100% |
Number of teeth Gouged out | 2 | 91 | 2.1% |
1 | 3 | 65% |
4 | 1 | 0.7% |
Total | 95 | 67.9% |
Extracted Teeth Type | Lower Canine | 87 | 62.2% |
upper canine | 7 | 5% |
Lower and upper canine | 1 | 0.7% |
Total | 95 | 67.9% |
Mutilation of another Child | Yes | 58 | 41.4% |
No | 82 | 58.6% |
Total | | 100% |
Source: Field Survey, 2024
Additionally, an overwhelming majority of the studied subjects (62.2%) were multilated at lower canine, 5% at the upper canine whereas the multation features at both canines was found only in 1 infant corresponding to 0.7% of the studied children and infants. This is comparable with the result of aformentioned research which revealed canine as the main enucleation site (Ibid), though, falled short to classify and examine the most multilated particular canine unlike this study. Among them 5% were missing the lower permanent incisors.
As the
table 2 shows, the surveyed mothers who had a second child other the admitted one were assessed whether they have mutilated the other children. Among 140 surveyed mothers only 82 of them had had mutilated another child corresponding to 58.6%. Out of these 58.6% mothers the majority of their children neatly 40% have survived and only 2 mothers reported death case due the oral mutilation. The data suggests that while mutilation is a significant concern, it does not frequently lead to death, indicating that interventions might be more focused on preventing mutilation in the first place rather than addressing fatal outcomes post-mutilation.
3.4. Equipment of Mutilation
During the operation of the mutilation among children different societies use different techniques and equipment for the teeth. The procedures and equipment used can have variety impacts on children and infant with differ intensities. In this we have looked for the procedures and equipment used by Somali society to assume its impacts.
As shown in
table 3, the largest portion of the victim infants, 23% out of 95 mutilated infants were used for an awl to gouge out the teeth. More specifically, some of participants has also reported that the awl was hot as few traditional mutilators use to burn the teeth instead of removing it. Additionally, 5% of the participants said that the awl was coupled with razor blade making the awl the most used tool for teeth extraction either alone or with razor blade in an average of 28% out of the total 67.9% of infants and children that are mutilated.
Table 3. Equipment for Infant oral mutilation.
Mutilation equipment | Frequency | Percentage |
Metals | 24 | 17% |
I don’t know | 1 | 0.71% |
Scissor | 13 | 9.3% |
Knife | 5 | 3.6% |
Awl | 32 | 23% |
Awl & razor blade | 7 | 5% |
Scissor & razor blade | 9 | 6.4 |
Knife & razor blade | 4 | 2.85 |
Total | 95 | 67.9 |
The second largest portion of 17% were used for unrecognized metals while the third largest group of about 9.3% were used for scissor to remove their teeth with 6.4% report of scissor coupled with razor blade making the scissors the second most recognized tool for the extraction in 15.7% out of 95 cases. A 3.6% of victims were also used for knifes followed by 2.85% report of knife with razor blade while only person was not knowing what instrument was used for the infant. However, though, all traditional healers use different tools of metals or metal origin materials, few of them have normal surgery kits and sterilization material for the infant mutilation.
In generally, the data shows, the awl stands out as the most significant equipment, accounting for 23.55% of the total 95 orally mutilated infants while un classified metals may mutually include awls, scissors, razor blade, knife or other instruments and individual equipment has varied significance, the equipment combinations (e.g., with razor) generally have lower percentages, suggesting these combinations are less commonly utilized.
3.5. The Risk Factors of Infant Oral Mutilation
Table 4. The Risk Factors of infant oral Mutilation.
Reason for Oral Mutilation | Frequency | Percentage |
Illness | 53 | 38% |
Diarrhea, Vomit & Fever | 16 | 11.4% |
Diarrhea | 14 | 10% |
Fever, mouth Scratching, sleep regression & unable to latch | 4 | 2.85% |
Diarrhea, Fever & Crying | 4 | 2.85% |
Diarrhea, Vomit & mouth Scratching | 4 | 2.85% |
Total | 95 | 67.9% |
Source: Field Survey, 2024
As
table 4 shows, the most frequently reported reason for mutilation was "Illness, comprising 38% of the cases. This suggests that a majority of mutilated infants could have a general illness that may or may not include specific symptoms like diarrhea or fever.
Diarrhea alone accounted for 10% of cases and is reported in multiple combinations i.e. Diarrhea, Vomiting & Fever (11.4%) indicating a significant combination.
"Diarrhea, Vomiting & Mouth Scratching as well as Diarrhea, Fever & Crying" have lower frequencies of 2.85% each, additional conditions involving "Fever" together with other symptoms (like mouth scratching and sleep regression) was reported as reason for mutilation. However, the occurrence of these symptoms together is notably rare compared to those that include diarrhea.
The other cases of multiple symptoms (e.g., Fever, mouth scratching, sleep regression & inability to latch the breast) were at 2.85%, which means they are less common though could be a reason in some cases.
In generally, the data set indicates that general illness was significant reason for mutilation, often presenting with diarrhea. Alike this, many researches have previously reported febrile illness and diarrhea as considerable risk factor for infant oral mutilation and the assumption of a connection between these common symptoms with the eruption of deciduous teeth has been made over many centuries
. Again, this data justified that many parents perform oral mutilation due to their assumption that it is remedy for childhood febrile illness. The research found that there was significant correlation between infant mutilation and above list risk factors (given the Pearson chi square result of 0.04 and the assumed marginal error of 0.07).
Apart from that, the FGDs and interview with doctors and Oral health practitioners also confirmed the above listed condition as the main reason that community removes infants’ canine buds.
In line with this, the FGD and KII stated that this assumption is main reason for the practice. For instance, (14) told:
“Normally infants get fever during teething and people believe that this will cause death if the tooth are not removed which is totally null and false, it is bacteria that causing the problem they see, we meet young and old people that were operated” (Key informant interview with Dentist, 2024).
Similarly, traditional healers believe that doing this procedure is essential for the wellbeing of the children and can provide remedy quicker than the normal antibacterial treatments for instant one respondent quoted:
| [15] | Mohamoud Hassan (Sheeko xariir) Interview with traditional healer Dec, 2024. |
[15]
“The procedure helps infant get quick recovery, it is bacterial infection but treatment cannot solve the problem though they get health as soon we remove the teeth” (Key informant interview with Dentist, 2024).
In generally, the data reveals that illness, particularly diarrhea, is the primary risk factor parents resort to this practice. Other symptoms such as vomiting, fever, and mouth scratching appear in various combinations but are less frequent. The reason is that many community members, including traditional healers, believe that this practice provides a quicker recovery than modern antibacterial treatments for the illness, although it has no scientific basis.
3.6. The Impact of Oral Mutilation on Infants
The fact given that that majority of the assessed kids were below five years of age and yet to reach the second teething age to develop consequent signs, 54.3% of infants have normal teeth conditions indicating that the majority are not affected by abnormal conditions, which could suggest a relative resilience to the effects of oral mutilation or that other factors may also play a role in dental health such that some of them were in pre-teeth development stage (see
table 5).
Table 5. The Impact of Oral mutilation.
| Category | Frequency | Percentage |
Infant teeth condition | Not mutilated | 45 | 32.1% |
Abnormal | 19 | 13.6% |
Normal | 76 | 54.3% |
Total | 140 | 100% |
Attitude of abnormality cause by mothers | Equipment | 2 | 1.42% |
Mutilation | 17 | 12.12% |
Total | 19 | 13.6% |
However, as
table 5 shows, a notable 13.6% of infants have abnormal teeth conditions of either missing teeth, hypodontia or dark stained (probably due to death of tooth as result of blood supply loss). This group, while less than the percentage of those with normal teeth, still highlighted a significant portion of infants affected potentially.
In addition to this, the practice results many complications later, that can result future oral problem or contraction of infectious disease due to the unhygienic tools that traditional practical use.
Teeth deformity, bleeding, risk of communicable disease infection i.e. HIV and Hepatis, damage to other adjustment oral cavity organs such as tongue and lips and effect on the other permanent teeth in the future as secondary teeth may be missing, supernumerary, become rudimentary or becomes painful and infected. more importantly, the most removed canine designs facial structure and if that is removed earlier the person face becomes ugly”
| [14] | Dr Mohamed Hamid (Gacal) Key Informant interview with Dentist, 10, Novermber, 2024. |
[14]
.
He also added:
Even today before you come to me, I met one case resulted by infant oral mutilation that has affected the permanent canine I removed the permanent canine as result of damage from previous traditional teeth extraction”
| [16] | Dr Ayub Said Key Informant interview with Dentist, 10, November, 2024. |
[16]
.
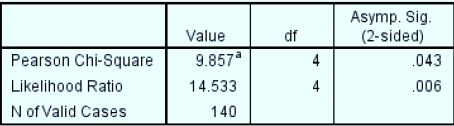
On the other hand, since there may be other important factors i.e. environmental, genetic, or nutritional factors that could affect dental health and may or may not be linked to oral mutilation and the presence of abnormal conditions could be influenced by various factors beyond infant oral mutilation, a crosstabulation was used to assess whether there is a significant connection between oral mutilation and the existence of abnormal teeth. The result indicated that the abnormal conditions are linked to practices of infant oral mutilation (given the below Pearson chi square result of 0.04 and the assumed marginal error of 0.07). This raises public health concerns that necessities intervention such as community’s education and awareness on the implication of oral mutilation practice.
Figure 1. Association of infant oral mutilation and existence of abnormal of teeth.
Attitude of Mothers Toward Cause of the Abnormal Teeth
The study assessed the attitude of mothers of the infant with abnormal teeth toward the cause of their infant teeth abnormality. The majority mothers perceive the practice of mutilation as a main cause of the abnormal infant teeth conditions, while a small portion of them perceive the mutilation equipment as the significant cause. Overall, the analysis indicates that mothers of affected children demonstrate a stronger concern regarding the risk of mutilation rather than equipment when considering the causes of abnormal infant teeth conditions in their children.
4. Conclusion
The prevalence of Infant Oral Mutilation (IOM) in Garowe, Somalia, is alarmingly high, with findings indicating that approximately 67.9% of surveyed infants have undergone the procedure. This harmful practice, often performed by untrained individuals using non-sterilized tools, poses severe health risks including immediate complications like bleeding and infections, as well as long-term dental issues. Factors driving this practice predominantly stem from traditional beliefs linking tooth extraction to illness prevention, particularly during teething episodes.
The study showed no significant association between offspring age and gender, maternal age, income level of families and parent education with the prevalence of IOM, which suggested that IOM is a deeply ingrained cultural practice in the community, uniformly affecting infants regardless of their demographic differences.
Contrastingly, the study revealed significant association between infant oral mutilation and abnormal teeth conditions. The findings underscore the urgent need for awareness and educational interventions to address the misconceptions surrounding IOM and its health implications.
5. Recommendations
To combat the harmful practice of Infant Oral Mutilation in Somalia, it is essential to implement a comprehensive multi-faceted approach. First, public health education campaigns should be launched to raise awareness about the dangers associated with IOM, targeting mothers and caregivers directly. The campaign against IOM needs to be integrated to primary health care components. Additionally, collaboration with local healthcare professionals and community leaders can facilitate the dissemination of information regarding safe infant care practices. Furthermore, establishing a regulatory framework to discourage the practice and promote the benefits of informed medical intervention is crucial.
More specifically, there is pressing need of Government to play role in creating legal mechanism prohibiting to publicly mutilate infants and before that it has to create transition period of notice and help those their life depends on this skill to transform in to other business with assistance of government. Lastly, continued research should be encouraged to monitor the prevalence and impact of IOM in various regions of Somalia, ensuring an ongoing understanding of this critical public health issue.
Abbreviations
IOM | Infant Oral Mutilation |
FGD | Focus Group Discussion |
KII | Key Informant Interview |
SPSS | Statistical Package for Social Science |
UK | United Kingdom |
DOI | Digital Objective Identifier |
HC | Health Center |
Acknowledgments
First of all, thanks to almighty Allah for enabling us write this paper. After that, we are deeply indebted to the research participants who accepted to lend some of their time to participate in the study. We would also like to thank and gratefully acknowledge to data collection team in the health centers for their contribution and hard work namely:
Abdiaziz Kaysane Siraad, Abdikeir Ahmed Ali, Abdiwali Abdillahi Adan, Abdulkadir Jamac Ahmed, Amal Mohamud Ali, Anisa Mohamed Hassan, Ayan Mohamed Elmi, Bisharo Dahir Ahmed, Fahm Mohamed Du’ale, Fatima Abdihakiin, Halima Mohamed Hassan, Hamdi Abshir Farah, Hussein Hassan Aden, Ifrah Yusuf Elmi, Isak Ali Aden, Munazi Mukhtar Ibrahim, Naima Hussien Hirsi, Nim’o Ismael Hirsi, Saed Abdirisak Muse, Zado Saleiman Ahmed, Zamzam Jama Abdi.
Authors Contribution
Abdinur Abdirizaksofe, Abdirashid jama Gure and Abdulahi Abdiwali Mahamed.
All the above-named authors made a significant contribution to the work reported, Particularly, Abdinur contributed to main manuscript including the study design, execution, acquisition of data, analysis and interpretation, Abdirashid contributed in research design, review and data analyses, Abdullahi Contributed in research drafting, review and data quality assurance. Additionally, all of them have done critical review and gave final approval of the version to be published.
Availability of Data and Material
The datasets used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Consent for Publication
We, the authors, named below hereby grant our consent for the publication of our article titled "The prevalence and practice of Infant Oral Mutilation in Garowe, Puntland Somalia" in Maternal & Child Nutrition”. We affirm that all authors have contributed to the research and writing of this manuscript and have reviewed and approved the final version for submission. We confirm that this work has not been published elsewhere and is not under consideration by any other publication. Additionally, we declare that we have disclosed any potential conflicts of interest and have adhered to ethical standards in our research, including obtaining necessary approvals. By granting this consent, we acknowledge that our writing may be edited for clarity, style, and length, and we retain the right to use the content in future works with appropriate citation.
Funding
This research was conducted as part of the authors' academic program, with no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Margaret N. W and Betsy. K.. (2017, juley). “Ebinyo”—The Practice of Infant Oral in Uganda. (T. Tiwari, Ed.) Frontiers in Public Health.
https://doi.org/10.3389/fpubh.2017.00167
|
| [2] |
Amare, T. (2019). The Dental complications of canine tooth bud removal in 2-12 years old children in north west Ethiopia. Research square, 4 (1-17).
https://doi.org/10.21203/rs.2.13352/v4
|
| [3] |
Arthur, M. K. (2015). Raising the awareness of infant oral mutilation - myths and facts. Contemp Clin Dent.
|
| [4] |
Jonathan, G. (2017). Dentaid impact document for IOM.
www.Dentaid.org
|
| [5] |
Global Child Dental Fund. (2018, February). End infant oral mutilation. Retrieved Noverber 20, 2019, from
https://www.endiom.org/
|
| [6] |
Hassanali J and Kibet P. (2014, September). Complex Factors Associated with Illnesses and Oral Mutilation in a “Vulnerable” African Infant. Austin Journal of Anatomy, 1-2.
|
| [7] |
Seligman CG, Seligman BZ. Pagan Tribes of the Nilotic Sudan. Published by George Routledge & Sons Ltd. 1932.
|
| [8] |
Wordley, V., Bedi, R. Infant oral mutilation in East Africa: eradication within ten years. Br Dent J 226, 14–15 (2019).
https://doi.org/10.1038/sj.bdj.2019.1
|
| [9] |
Rodd HD and Davidson LE. (2000). 'Ilko dacowo:' canine enucleation and dental sequelae in Somali children. Int J Paediatr Dent, (4): 290-7.
|
| [10] |
Egbert, E. A. (2000). Dental injuries due to African traditional therapies for diarrhea. Western Journal of medicine, 135–137.
|
| [11] |
Israel, G. D. (1992). Determining the sample size. Orlando: Florida University.
|
| [12] |
Smith, S. M. (2013, April 8). Determining Sample Size. Retrieved January 13, 2017, from Qualtrics:
http://success.qualtrics.com/rs/qualtrics/images/Determining-Sample-Size.pdf
|
| [13] |
Esti Davidovich, E. K. (2013). The traditional practice of canine bud removal in the offspring of Ethiopian immigrants. BMC Oral Health.
|
| [14] |
Dr Mohamed Hamid (Gacal) Key Informant interview with Dentist, 10, Novermber, 2024.
|
| [15] |
Mohamoud Hassan (Sheeko xariir) Interview with traditional healer Dec, 2024.
|
| [16] |
Dr Ayub Said Key Informant interview with Dentist, 10, November, 2024.
|
Cite This Article
-
APA Style
Sofe, A. A., Gure, A. J., Mahamed, A. A. (2025). The Prevalence and Practice of Infant Oral Mutilation in Garowe, Puntland Somalia. Central African Journal of Public Health, 11(3), 135-144. https://doi.org/10.11648/j.cajph.20251103.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Sofe, A. A.; Gure, A. J.; Mahamed, A. A. The Prevalence and Practice of Infant Oral Mutilation in Garowe, Puntland Somalia. Cent. Afr. J. Public Health 2025, 11(3), 135-144. doi: 10.11648/j.cajph.20251103.14
Copy
|
Download
AMA Style
Sofe AA, Gure AJ, Mahamed AA. The Prevalence and Practice of Infant Oral Mutilation in Garowe, Puntland Somalia. Cent Afr J Public Health. 2025;11(3):135-144. doi: 10.11648/j.cajph.20251103.14
Copy
|
Download
-
@article{10.11648/j.cajph.20251103.14,
author = {Abdinur Abdirisak Sofe and Abdirashid Jama Gure and Abdulahi Abdiwali Mahamed},
title = {The Prevalence and Practice of Infant Oral Mutilation in Garowe, Puntland Somalia
},
journal = {Central African Journal of Public Health},
volume = {11},
number = {3},
pages = {135-144},
doi = {10.11648/j.cajph.20251103.14},
url = {https://doi.org/10.11648/j.cajph.20251103.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251103.14},
abstract = {Infant oral mutilation (IOM) is a harmful traditional practice of gouging out the unerupted developing infant primary teeth, usually the canine bud. It exposes immediate and long-term direct health effects, including bleeding-led anemia, septicemia, tetanus, osteomyelitis, meningitis, or even HIV as a result of unsterile tools. Given that, the general objective of the study was to assess infant oral mutilation in Garowe, Somalia. The research employed an analytical cross-sectional design that utilized both qualitative and quantitative approaches. Both probability and non-probability sampling techniques were simultaneously used. Initially, the Garowe district was purposively selected as the study area. Subsequently, a cluster sampling method was applied to identify seven of the most frequently visited health centers out of the twelve registered in the district. Then, a convenience sampling technique was used to recruit 140 children and infants who visited the facilities earliest, along with their mothers, for oral health examinations and interviews, respectively. Additionally, non-probability purposive sampling was utilized to select two dental doctors practicing in Garowe and two traditional practitioner healers practicing in IOM. Furthermore, a gender-representative focus group discussion (FGD) was conducted with community members to gather qualitative insights and cross-check the information. The study found that only 45 (32.1%) children were not gauged out, while 95 of the studied 140 participants were orally mutilated, making up an IOM prevalence of 67.9%, with the majority of them (62.2%) mutilated at the lower canine and 5% at the upper canine, whereas the mutilation features at both canines were found only in 0.7% of the studied children and infants. The study identified that various tools, often unsterilized, are used for the practice, such as an awl, alongside scissors and knives, while some traditional healers have medical surgical kits. In terms of risk factors associated with IOM, the study reveals that the primary motivation for IOM practice stems from linking tooth extraction to alleviating common childhood illnesses, especially diarrhea and fever. There was no significant association between IOM prevalence and factors such as age or gender of the children, maternal age, family income, or parental education. However, a significant association was found between IOM and abnormal dental conditions like missing or malformed teeth. The findings indicate that the prevalence of IOM in Garowe is alarmingly high, suggesting the urgent need for awareness and educational interventions to address the misconceptions surrounding IOM and its health implications.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - The Prevalence and Practice of Infant Oral Mutilation in Garowe, Puntland Somalia
AU - Abdinur Abdirisak Sofe
AU - Abdirashid Jama Gure
AU - Abdulahi Abdiwali Mahamed
Y1 - 2025/06/23
PY - 2025
N1 - https://doi.org/10.11648/j.cajph.20251103.14
DO - 10.11648/j.cajph.20251103.14
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 135
EP - 144
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20251103.14
AB - Infant oral mutilation (IOM) is a harmful traditional practice of gouging out the unerupted developing infant primary teeth, usually the canine bud. It exposes immediate and long-term direct health effects, including bleeding-led anemia, septicemia, tetanus, osteomyelitis, meningitis, or even HIV as a result of unsterile tools. Given that, the general objective of the study was to assess infant oral mutilation in Garowe, Somalia. The research employed an analytical cross-sectional design that utilized both qualitative and quantitative approaches. Both probability and non-probability sampling techniques were simultaneously used. Initially, the Garowe district was purposively selected as the study area. Subsequently, a cluster sampling method was applied to identify seven of the most frequently visited health centers out of the twelve registered in the district. Then, a convenience sampling technique was used to recruit 140 children and infants who visited the facilities earliest, along with their mothers, for oral health examinations and interviews, respectively. Additionally, non-probability purposive sampling was utilized to select two dental doctors practicing in Garowe and two traditional practitioner healers practicing in IOM. Furthermore, a gender-representative focus group discussion (FGD) was conducted with community members to gather qualitative insights and cross-check the information. The study found that only 45 (32.1%) children were not gauged out, while 95 of the studied 140 participants were orally mutilated, making up an IOM prevalence of 67.9%, with the majority of them (62.2%) mutilated at the lower canine and 5% at the upper canine, whereas the mutilation features at both canines were found only in 0.7% of the studied children and infants. The study identified that various tools, often unsterilized, are used for the practice, such as an awl, alongside scissors and knives, while some traditional healers have medical surgical kits. In terms of risk factors associated with IOM, the study reveals that the primary motivation for IOM practice stems from linking tooth extraction to alleviating common childhood illnesses, especially diarrhea and fever. There was no significant association between IOM prevalence and factors such as age or gender of the children, maternal age, family income, or parental education. However, a significant association was found between IOM and abnormal dental conditions like missing or malformed teeth. The findings indicate that the prevalence of IOM in Garowe is alarmingly high, suggesting the urgent need for awareness and educational interventions to address the misconceptions surrounding IOM and its health implications.
VL - 11
IS - 3
ER -
Copy
|
Download