1. Context
The healthcare system in Côte d'Ivoire has several shortcomings in terms of healthcare services, such as insufficient implementation of the healthcare organization master plan and standards and procedures for healthcare organization, a lack of harmonization of treatment protocols, and the virtual absence of advanced and mobile activities covering populations beyond the geographical access perimeter, which severely hamper universal access to essential health services, as well as shortcomings in the organization of referrals, counter-referrals, and emergencies. In terms of human resources, the doctor-to-population ratio was 1.4 doctors per 10,000 inhabitants in 2019, revealing disparities in human resources between districts, with only 43.0% of health districts meeting the WHO standard.
The National Health Development Plan (PNDS) aims to provide solutions to improve the health system and has made digital health one of the pillars of this plan. Indeed, the PNDS stated that “In terms of technological innovation, emphasis will be placed on the use of technology and digitalization to increase efficiency and quality in the delivery of health services, as well as accountability and transparency in the use of financial and human resources”
| [1] | Ministry of Health and Public Hygiene of Côte d'Ivoire. National Health Development Plan (PNDS) 2012-2015. |
[1]
(PNDS 2021-2025, 100).
In 1997, the World Health Organization (WHO) defined telemedicine as “the part of medicine that uses telecommunications to transmit medical information for the purpose of obtaining a remote diagnosis, specialist opinion, continuous monitoring of a patient, or therapeutic decision.”
As early as 2005, the WHO encouraged member states to develop a long-term strategy for the development of eHealth services with the aim of promoting equitable and universal access to its benefits. To this end, in 2012, the WHO published the National eHealth Strategy Toolkit, a technical and practical tool to help countries implement their eHealth policies according to their needs and capacities, which obviously differ depending on whether the country is rich or poor. In 2013, the WHO proposed a resolution on the standardization and interoperability of eHealth. It is therefore no surprise that in 2018, the WHO embarked on a broad consultation process to propose the Global Digital Health Strategy 2020-2025. This was adopted by the World Health Assembly of all WHO member states in 2020
| [2] | WHO. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening. Geneva: World Health Organization. 2019. |
[2]
.
In Côte d'Ivoire, a strategic plan for 2012-2015 was developed in 2011. To this end, e-health supports the priorities of Côte d'Ivoire's national development plan (2012-2015), which aims to provide the highest level of healthcare to the population by harmonizing material resources, pooling resources, and finding solutions to the country's health problems. To ensure the success of this plan, which aims to significantly improve the quality of health system management and care for the Ivorian population by developing and supporting integrated health policy and program reform initiatives, eight strategic guidelines have been identified.
It should be noted that it was in 2005-2006 that Côte d'Ivoire began the digital transformation of its health system through Indo-African cooperation via the “E-panafrican network” project. Furthermore, taking into account the recommendations of the World Health Organization (WHO) and the 2005 World Summits on the Information Society (WSIS), Côte d'Ivoire included e-health in its 2012-2015 national development plan. All of this is supported by a vast digital transformation project, initiated by the government of Côte d'Ivoire across its entire administration, with major sectoral challenges starting in 2011. According to data from the Telecommunications/ICT Regulatory Authority of Côte d'Ivoire
| [3] | Ministry of Digital Economy, Telecommunications, and Innovation (MENTI). (2021) “National Cybersecurity Strategy of Côte d'Ivoire 2021-2025.” Abidjan, Côte d'Ivoire. |
[3]
, the internet penetration rate was 98.90% (covering 22,421,447 out of 22,671,331 people) in 2023, and the network coverage rate was 95.52% (8,136 out of 8,518 localities were covered) in Côte d'Ivoire in 2025. Information and communication technologies (ICT) are a key factor in improving the performance of our healthcare system, which has led to the implementation of several digital health projects. Furthermore, the Covid-19 pandemic that occurred in 2020 has accelerated the implementation of digital health around the world, particularly in Côte d'Ivoire. In his publication.
Digital health therefore presents an opportunity to address the many challenges facing the healthcare system. The aim of the study was to understand the impact of digital health on service delivery in Côte d'Ivoire, the barriers to implementing digital health, and to provide a critical analysis of the impact and recommendations of digital health on healthcare delivery.
2. Methodology
2.1. Part of the Study
The study was conducted in Côte d’Ivoire. Côte d’Ivoire is a country in West Africa, which has an area of 322 462 squares kilometers and had 33 millions habitants.
2.2. Type and Duration of the Study
This study took place from March to April 2025. This study was a narrative literature review.
2.3. Literature Review
2.3.1. Bibliographic Sources
Documents were retrieved from the following bibliographic sources:
1) Grey literature from websites of institutions active in digital health, and the Ministry of health of Cote d’Ivoire, among others.
2) Scientific articles via search engines such as Google Scholar and databases including PubMed/Medline.
Keywords and Search Strategies
The identified keywords and search strategies were:
1) In French: “santé digitale” AND “offre de soins” AND “Afrique subsaharienne”.
2) In English: “Digital Health Innovations” AND “Delivery of health care” AND “Sub-Saharan Africa”.
2.3.2. Inclusion Criteria
Documents were selected based on the following criteria:
1) Inclusion criteria: geographic focus (Sub-Saharan Africa), publication period (within the last 5 years, i.e., 2020–2025).
2) Exclusion criteria: documents not addressing digital health and those that were inaccessible.
2.3.3. Description of Research Results
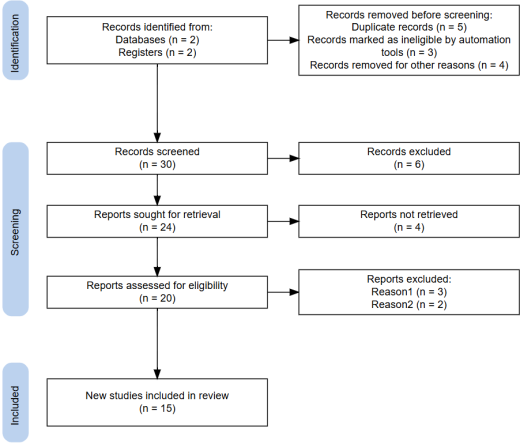
The initial search yielded 42 records from databases and institutional sources. After removal of 12 duplicate records, 30 documents remained for screening based on titles and abstracts. Following this screening, 15 records were excluded due to insufficient relevance to the study objectives. Finally, 15 documents were included in the narrative synthesis. The study selection process followed the PRISMA 2020 guidelines
| [4] | Haddaway, N. R., Page, M. J., Pritchard, C. C., & McGuinness, L. A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230.
https://doi.org/10.1002/cl2.1230 |
[4]
, and the flow diagram is presented (
Figure 1).
PRISMA chart flow demonstrated how studies were selected (PRISMA)
| [4] | Haddaway, N. R., Page, M. J., Pritchard, C. C., & McGuinness, L. A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis Campbell Systematic Reviews, 18, e1230.
https://doi.org/10.1002/cl2.1230 |
[4]
.
Figure 1. Description of documents selection steps via PRISMA chart flow.
2.3.4. Domains of Analysis
The review focused on three primary domains:
1) Digital health on healthcare delivery.
2) Barriers of digital health in sub-saharian Africa.
3) Recommendations of digital health.
This literature review provides a foundation for understanding the evolving landscape of digital health in Côte d’Ivoire and sub-Saharan Africa, aligning with global frameworks such as the WHO Global Strategy on Digital Health 2020–2025 and national policies including the Plan National de Développement Sanitaire (PNDS) 2021–2025.
2.4. Limitations
This study presented some limitations such as potential bias from reliance on gray literature and the short time frame.
3. Results
3.1. Characteristics of Projects
This chapter presented three projects of digital health innovations in Côte d’Ivoire, described below: national e-health project (national project), telemedicine project at Abobo Nord General Hospital (local project), and electronic vaccination record project (national project). Each of these projects had some particularities that are described in this paper.
3.2. National e-Health Project
The project was a national project
| [5] | Ministry of Health and Public Hygiene of Côte d'Ivoire. 2018. Hospital information system (HIS) and telemedicine: overview of existing experiences in Côte d'Ivoire. Ministry of Health and Public Hygiene of Côte d'Ivoire. |
[5]
, launched in both rural and urban areas. The project targeted healthcare professionals, healthcare facilities, and patients. The Objectives of the project was:
1) To integrate ICTs into the management of healthcare facilities by implementing the necessary infrastructure,
2) To improve the efficiency of healthcare professionals through the introduction of telemedicine and distance learning systems,
3) To provide healthcare facilities with high-speed internet access,
4) To implement electronic patient records (EPRs).
This project also aimed to bridge the gaps between urban and rural areas, facilitate universal access to referral and specialized centers, and ensure greater health equity for all populations.
The national e-health project was initiated in two regions (Abidjan, and Agboville) distanct from 60 kilometers. The specificities of town targeted was following, Agboville was town based in rural area, and Abidjan concentrated the reference specialized health centers.
This project involved interconnecting 5 remote healthcare establishments, 2 university health centers (CHU) located in Abidjan, 1 regional health center (CHR) located in Agboville, and 2 urban health facilities, and deploying telemedicine solutions.
The main result was an augmentation of people teleconsulting per month between the CHR and the CHU. This project also permitted thousands of computerized patient records and regular training sessions between the national telemedicine center and the various connected sites
| [6] | Ministry of Health and Public Hygiene of Côte d'Ivoire. 2018. The medico-economic challenges of telemedicine and digital health in Côte d'Ivoire. 3rd International Digital Health Forum, Tunisia 2018. |
[6]
.
The project also enabled:
1) 20 people to be teleconsulted per week, or 80 people per month, between the regional hospital in Agboville and the university hospital in Yopougon, thus avoiding travel for a simple medical opinion.
2) For traceability, nearly 200,000 computerized patient files have been opened.
3) Regular tele-training sessions between the national telemedicine center and the various connected sites (health professionals).
4) Tele-expertise, sharing of clinical cases under the supervision of a mentor and an expert. To date, 30 clinical cases have been shared in this way.
5) The project reduced the mortality and ameliorated the follow-up of the patients leaving in rural areas.
6) The project reduced referrals of patients from rural to urban areas by improving local care and avoiding difficult patient transfers.
3.3. Telemedicine Project at Abobo Nord General Hospital
This project had part of a public-private partnership. This project was launched in 2014 and extended to nearly eight public health estab-lishments in the health district of Abobo. The project named E@voire, was a telemedicine and computerized patient record project. This project involved con-necting services, to systematize the patient pathway and establish a single computerized patient record for each patient. The main results of this project were described in the
Table 1.
Table 1. Distribution of medical-economic issues according to the level of intervention.
Level of intervention | Medical-economic issues |
Patient care | The doctor-patient relationship is improving thanks to the use of increasingly integrated information systems. Reduction in latency time, which has fallen from 40 to 20 minutes on average. More than fifty thousand (50,000) unique patient records have been created. Traceability of all medical procedures throughout the patient's life. Best follow-up of patient, ameliorated patients care and reduced mortality |
Healthcare professional and institution level | Efficiency: better use of purely medical time, decision-making and diagnostic tools. Quality: access to validated medical knowledge, opportunity for teamwork and networking, training resources for healthcare personnel, breaking down barriers between private practice, hospitals, and the medico-social sector with a view to providing a seamless care pathway. Better allocation of human and financial resources. To date, the structure's endogenous resources have quadrupled, from 40 million to 160 million CFA francs. |
State level | Better budget allocation taking into account the real needs of the General Hospital, which has increased from 80 million to 300 million |
sources: Minsitry of Health
| [6] | Ministry of Health and Public Hygiene of Côte d'Ivoire. 2018. The medico-economic challenges of telemedicine and digital health in Côte d'Ivoire. 3rd International Digital Health Forum, Tunisia 2018. |
[6]
3.4. Electronic Vaccination Record Project
This project was a model public-private partnership with an Ivorian start-up supported by the Ministry of Health and Public Hygiene (MSHP). The project included an electronic vaccination record, an SMS reminder service for vaccination dates, and the dissemination of awareness-raising information. The initiative began in 2011 with a pilot project and the registration of 20,304 users for the service
| [5] | Ministry of Health and Public Hygiene of Côte d'Ivoire. 2018. Hospital information system (HIS) and telemedicine: overview of existing experiences in Côte d'Ivoire. Ministry of Health and Public Hygiene of Côte d'Ivoire. |
[5]
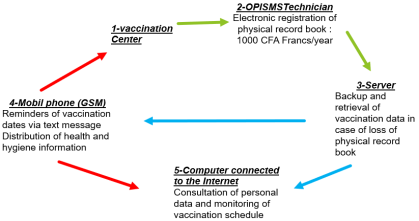
. The project named OPISMS, was a vaccination monitoring tool complementary of the ordinary vaccination booklet, based on a mechanism for sending grouped SMS messages.
The initiative aims to increase vaccination coverage by sending SMS reminders about vaccination dates and raising public awareness of the importance of this medical procedure. It also provides users with a virtual vaccination record (
Figure 2). The goal is to reduce mortality, decrease morbidity, and improve patient care.
However, the priority for follow-up remained Expanded Program of Immunization (EPI) targets (pregnant women and children aged 0 to 1) and travellers. Its main functions were to reminder of vaccination appointments by message, safeguarding and perpetuating individual vaccination data for faithful restitution in the event of loss of the physical booklet, facilitating justification of a vaccination act to issue a duplicate; informing about health hygiene rules, and reinforcing patient-health worker communication
| [6] | Ministry of Health and Public Hygiene of Côte d'Ivoire. 2018. The medico-economic challenges of telemedicine and digital health in Côte d'Ivoire. 3rd International Digital Health Forum, Tunisia 2018. |
[6]
.
Five steps were identified to implement this project.
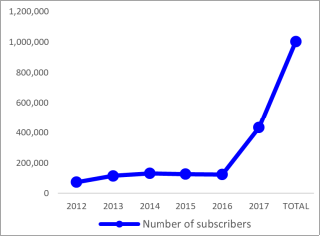
The electronic vaccination record project enrolled 1 001 678 subscribers during the 6 years (2012 to 2017).
The project also helped to reduce vaccination dropout rates and improve the prevention of vaccine-preventable diseases.
4. Discussion
4.1. Critical Evaluation of Digital Health Initiatives and Their Impact
The findings of this study highlight several key digital health initiatives in Côte d’Ivoire, integration efforts under the National Health Development Plan (Plan National de Développement Sanitaire, PNDS) 2021–2025. This section critically evaluated their impact on healthcare delivery across four criteria: accessibility, cost-effectiveness, quality of care, and health system efficiency. The analysis assessed strengths and weaknesses of each initiative, incorporating available outcome data, while addressing risks related to sustainability, equity (including the digital divide), and data privacy.
4.2. Critical Analysis: Evaluating the Achievement of Project Objectives
4.2.1. National e-Health Project
Through its various achievements, the project has successfully met its initial objectives. It has broken down barriers between rural and urban areas, notably by bridging the gap between healthcare professionals through digital solutions (e.g., patient records, teleconsultations, etc.).
4.2.2. Telemedicine Project at Abobo Nord General Hospital
The project has achieved its initial objectives. It has provided hospitals with equipment, created unified patient records, and contributed to improved budgets for the various healthcare facilities involved in the project.
4.2.3. Electronic Vaccination Record Project
The initial objectives of this project were to achieve vaccination reminders for a large proportion of the population and to contribute to reducing the vaccination dropout rate by 50%. In 2025, according to health system data, most of ten years after its implementation, the project increased the number of users from 25 000 to 1 001 678, and the dropout rate for vaccinations improved. Overall, the project met its objectives.
4.3. Critical Analysis by Criterion
1) Accessibility
a) Strengths: These initiatives have substantially bridged urban-rural disparities by enabling remote access to specialised care. Telemedicine services in Agboville provide specialised care (cardiology, gynaecology, obstetrics, and paediatrics) across facilities, enhancing equitable access in rural settings. offers a portable digital health record via wearable devices, while OPISMS supports nationwide immunization tracking.
b) Weaknesses and Equity Implications: Persistent digital divide issues, with low internet penetration around in rural areas as of 2025, excluded vulnerable populations, potentially exacerbated health inequities rather than alleviating them.
c) Outcomes: Improved specialist access for thousands; however, universal coverage remained unmet.
2) Cost-Effectiveness
a) Strengths: Significant reductions in patient and provider expenses have been achieved. while M-Vaccin streamlines vaccination logistics via SMS reminders and digital registries.
b) Weaknesses and Sustainability Risks: High initial costs for equipment and training, coupled with reliance on external funding (e.g., donors and public-private partnerships), threaten long-term viability, as seen in pilot-to-scale transitions across African contexts. Indeed, in kenya a study showed that challenges include over-reliance of mobile apps on smart phones whereas majority of mobile subscribers own devices without internet-connection features
| [7] | Nyatuka, Danny Ronald and de la Harpe, Retha. Evaluating mHealth Interventions in an Underserved Context Using Service Design Strategy: A Case of Kenya. 2019. Association for Computing Machinery. New York, USA.
https://doi.org/10.1145/3340037.3340060 |
[7]
. Hinney results in a scoping review in sub saharian Africa, showed that poor internet connectivity also hindered the adoption of digital health tools in many ways. Almost all mHealth platforms rely on stable internet given that such applications use cellular networks
| [8] | Hinneh T, Mensah B, Kwanin C, Okonkwo C, Byiringiro S. Digital health tools in hypertension management in sub-Saharan Africa: a scoping review of barriers and facilitators of adoption into mainstream healthcare. BMJ Health Care Inform. 2025 Oct 10; 32(1): e101261.
https://doi.org/10.1136/bmjhci-2024-101261 |
[8]
.
c) Outcomes: Demonstrated savings in pilots, including reduced consultation delays (e.g., from 40 to 20 minutes in similar hospital informatisation projects, with over 50,000 unique patient records created locally).
3) Quality of Care
a) Strengths: Enhanced diagnostics, treatment adherence, and patient outcomes through decision-support tools and inter-sectoral collaboration. improving rural care quality via urban specialist input, consistent with broader evidence
| [9] | Riegelman, R. K., Kirkwood, B. Public health 101: improving community health. Third edition. Burlington, MA: Jones & Bartlett Learning. 2019. Available at:
https://lccn.loc.gov/2017044501 |
[9]
.
b) Weaknesses: Risks of diagnostic errors from unreliable connectivity or inadequate training, alongside limited interoperability between platforms.
c) Outcomes: increased patient satisfaction.
4) Health System Efficiency
a) Strengths: Streamlined operations and resource allocation via electronic records and offline functionalities, aligned with African contextual needs. The PNDS 2021–2025 integrates digital health for referral management and universal health coverage progression.
b) Weaknesses and Data Privacy Risks: Weak enforcement of the 2013 data protection law increases vulnerability to breaches, eroding trust, while non-interoperable data silos hinder system-wide gains.
c) Outcomes: Operational efficiencies in pilots, contributing to universal health coverage through digital integration.
4.4. Overall Critical Discussion: Strengths, Weaknesses, and Implications
Overall Strengths: These initiatives exhibit transformative potential, accelerated post-COVID-19, and align with the WHO Global Strategy on Digital Health. They promote local innovation (and targeted inclusion (e.g., women and children).
Overall Weaknesses: Fragmentation (pilots not nationally scaled), external funding dependency, and insufficient governance (interoperability and privacy).
Risks and implications :
1) Sustainability: Absent recurrent funding and PNDS integration, long-term failure is probable.
2) Equity: The digital divide risks widening disparities, excluding vulnerable groups despite inclusive intentions.
3) Data Privacy: Urgent reinforcement of legal frameworks is needed to prevent sensitive data leaks.
In conclusion, while promising, these initiatives necessitate strengthened governance, infrastructure investment, and inclusive approaches to maximise benefits and mitigate risks.
4.5. Best Practices in Digital Health in Côte d’Ivoire
Building on the foregoing critical analysis, best practices emerge from robust policy environments and context-adapted design. Identified Best Practices were:
1) Governance and Policy: Integration into the PNDS 2021–2025 for coordinated referral management and care proximity.
2) Telemedicine and Digital Records: Successes in hospital informatisation (e.g., Telemedecine project in Abobo Nord).
3) Local Adaptation: Hybrid (offline/online) solutions and portable tools for rural inclusion (e.g., national e-health project); multisectoral partnerships (e.g., Orange for OPISMS project).
To enhance sustainability, priorities include continuous training, interoperability, multisectoral partnerships, and reinforced regulation on privacy and equity. Scaled nationally, these practices could profoundly advance the health system towards effective universal health coverage.
4.6. Barriers to Implementation
The main barriers to implementing digital health innovation concerned essentially concerned infrastructure limitations, regulatory and policy challenges, financial constraints, and health workforce readiness. For each of these barriers, we identified details that merit particular attention to improve the implementation of digital health.
In terms of the infrastructure limitations, it concerned internet connectivity and power supply issues. The regulatory and policy challenges concern data privacy, licensing, and integration with existing health policies. The financial constraints is the high costs of adoption and maintenance. The health workforce readiness are concerning by training and resistance to technological change.
These obstacles were also noted in Chinenyenwa's research, who stated that digital health technology adoption is hindered by challenges such as inadequate training, limited infrastructure, and concerns over data privacy
| [10] | Chinenyenwa, O., Ongolo-Zogo, P., Olufunmilayo, I. F. Digital Health Information Technology Utilization for Enhanced Health Services Delivery in Africa: Unravelling Barriers to Adoption among Primary Healthcare Providers, South Eastern European Journal of Public Health, 2021. Available at:
https://www.biejournals.de/index.php/seejph/article/view/4381 |
[10]
.
For Novakowski study, high staff turnover and a lack of medical supplies at the hospital were the primary barriers to the feasibility of Smart Triage
| [11] | Novakowski, S. K., Kabajaasi, O., Kinshella, ML. W. et al. Health worker perspectives of Smart Triage, a digital triaging platform for quality improvement at a referral hospital in Uganda: a qualitative analysis. BMC Pediatr 22, 593 (2022).
https://doi.org/10.1186/s12887-022-03627-1 |
[11]
.
4.6.1. Barriers Analysis for Digital Health Innovation Implementation
Digital health innovations hold immense potential to improve healthcare access, efficiency, and outcomes, particularly in resource-constrained settings like those implied by infrastructure and connectivity challenges. However, the four primary barriers identified:
Infrastructure limitations (e.g., internet connectivity and power supply),
regulatory and policy challenges (e.g., data privacy, licensing, and policy integration),
financial constraints (e.g., high adoption and maintenance costs), and
health workforce readiness (e.g., inadequate training and resistance to change)) are deeply interconnected.
These align with broader evidence from low- and middle-income countries (LMICs), where similar obstacles hinder adoption, as noted in studies emphasizing inadequate infrastructure, privacy concerns, and training gaps
| [8] | Hinneh T, Mensah B, Kwanin C, Okonkwo C, Byiringiro S. Digital health tools in hypertension management in sub-Saharan Africa: a scoping review of barriers and facilitators of adoption into mainstream healthcare. BMJ Health Care Inform. 2025 Oct 10; 32(1): e101261.
https://doi.org/10.1136/bmjhci-2024-101261 |
[8]
.
4.6.2. Ranking by Severity
Ranking barriers requires considering their foundational impact: a barrier that blocks progress at the most basic level is more severe, as it prevents addressing others. In LMICs and low-resource settings, evidence consistently identifies infrastructure as the most critical impediment, followed by interconnected human and systemic factors
| [12] | Bajpai, N., & Wadhwa, M. (2021). India's Experience with ICT in the Health Sector: Lessons for sub-Saharan Africa (No. 51). ICT India Working Paper. |
[12]
:
1) Infrastructure Limitations (Highest Severity) This is the most severe barrier because digital health tools fundamentally require reliable internet, electricity, and hardware to function. Without these, no innovation can be deployed, used, or maintained. Systematic reviews and scoping studies in LMICs highlight unreliable power, poor connectivity, and lack of devices as primary roadblocks, often rendering other efforts futile.
2) Health Workforce Readiness (High Severity) Even with basic infrastructure, untrained or resistant staff cannot effectively adopt tools, leading to low utilization and failure. Inadequate training and change resistance exacerbate errors, reduce efficiency, and perpetuate skepticism.
3) Financial Constraints (Moderate-High Severity) High upfront and ongoing costs limit procurement, maintenance, and scaling. This barrier amplifies others, as limited budgets restrict investments in infrastructure upgrades or training programs.
4) Regulatory and Policy Challenges (Moderate Severity) Issues like unclear data privacy laws, licensing for telehealth, and poor integration with existing policies create uncertainty and legal risks. Interoperability issues persist in health systems because information systems are fragmented, standards are undefined or poorly enforced, and governance and human capacity are often insufficient. These problems prevent the smooth exchange of data, leading to duplication of work, inefficient use of resources, fragmentation of clinical care, and poor quality of health system information. As a result, data remains siloed, decision-making is based on incomplete evidence, investments in digital health offer limited returns, and informal data-sharing practices increase risks to data security and trust. Overall, poor interoperability is a systemic failure that undermines the efficiency, coordination, and effective sharing of health system data.
While critical for trust and scalability, these can often be navigated once core operational barriers are addressed.
In many African countries, «digital health regulations are often disorganized, with multiple bodies exerting control without clearly defined responsibilities. This fragmentation can hinder the effective use of digital health technologies, leading to potential health risks and market inefficiencies. These include disorganized regulation, regulatory complexity owing to the diversity of digital health tools, insufficient data protection laws, and lack of technical expertise among regulatory staff».
| [13] | Bataliack, S., Ebongue, M., Karamagi, H., & Janauschek, L. (2024). Health data digitalization in Africa: unlocking the potential. Brazzaville: WHO Regional Office for Africa; 2024. |
[13]
This ranking draws from patterns in LMIC-focused reviews, where infrastructure and workforce issues dominate as "foundational" blockers, while financial and regulatory challenges are systemic enablers/constraints.
Addressing one barrier often mitigates others; for instance, securing funding for infrastructure can enable better training and policy alignment.
4.6.3. Proposed Mitigation Strategies
Strategies should be prioritized (starting with foundational barriers), multi-level (involving government, donors, providers), and integrated to leverage interdependencies. Evidence-based approaches from LMIC reviews include:
Table 2. Distribution of mitigation strategies issues according to the type of barrier.
Barrier | Key Mitigation Strategies | Expected Impact |
Infrastructure Limitations | 1) Invest in hybrid solutions (e.g., offline-capable apps, SMS-based tools). 2) Public-private partnerships for rural connectivity and solar-powered devices. 3) National digital health strategies prioritizing power reliability. | Builds the foundation; enables training and tool deployment, reducing downstream costs and resistance. |
Health Workforce Readiness | 1) Mandatory, ongoing training programs tailored to local needs. 2) Change management initiatives addressing resistance. 3) Integrate digital literacy into health education curricula. | Increases acceptance and competence; mitigates regulatory risks through better data handling and improves cost-effectiveness via efficient use. |
Financial Constraints | 1) Seek donor/grant funding and cost-sharing models. 2) Government subsidies for adoption/maintenance in public facilities. | Frees resources for infrastructure and training; sustainable models address long-term costs. |
Regulatory and Policy Challenges | 1) Develop clear national guidelines on data privacy, licensing, and interoperability. 2) Harmonize with international standards. 3) Multi-stakeholder forums for policy co-creation. | Builds trust and attracts investment; facilitates integration, reducing financial and workforce burdens. |
A study realized in three country of Sub-saharian Africa showed that to adequately protect public interests and increaseaccess to healthcare for African citizens, especially for those most marginalized, digitalhealth innovation and regulatory frameworks should promote equitable access to digitalhealth technologies and to ensure they do not exacerbate existing health disparities
| [14] | Sharifah Sekalalaa, Belinda Rawsona and Pamela Andandaba. 2025. A socio-legal critique of the commercialization of digitalhealth in Sub-Saharan Affrica. School of Law, University of Warwick, Coventry, UK; b School of Law, University of Witwatersrand, Johannesburg, South Africa.
https://doi.org/10.1080/01442872.2025.2451966 |
[14]
.
A holistic approach can break interdependence cycles.