Anomalous coronary arteries (ACA) represent a heterogeneous group of anatomical variants with a wide range of clinical implications. While many are benign, specific courses may predispose to ischemia, myocardial infarction, heart failure, or sudden cardiac death. We present a rare case of a 62-year-old man with an anomalous left main (LM) coronary artery originating from a shared right coronary ostium, demonstrating a mixed interarterial and transseptal course. Multimodality imaging with cardiac CT angiography (CTA), cardiac magnetic resonance imaging (CMR), and invasive coronary angiography with intravascular ultrasound (IVUS) and physiologic assessment revealed dynamic systolic compression of a prominent first septal perforator, associated with mid-myocardial fibrofatty infiltration and fibrosis. Resting hemodynamics were normal; however, provocative maneuvers elicited significant ischemia as evidenced by abnormal instantaneous wave-free ratio (iFR) changes. Despite the anatomical complexity and hemodynamic findings, the patient opted for conservative management following a detailed discussion of surgical revascularization options. This case highlights the nuanced spectrum of clinical significance in anomalous LM coronary arteries, challenging the traditional benign versus malignant classification. Comprehensive anatomical and physiological evaluation is critical, especially in mixed-course anomalies. Our findings underscore the role of multimodal imaging modalities and functional testing in guiding individualized patient management in rare coronary anomalies.
| Published in | Cardiology and Cardiovascular Research (Volume 9, Issue 2) |
| DOI | 10.11648/j.ccr.20250902.15 |
| Page(s) | 69-74 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Anomalous Coronary Artery, Transeptal Course, Coronary Computed Tomographic Angiography, Exertional Chest Pain, Instantaneous Wave-free Ratio
ACA | Anomalous Coronary Arteries (ACA) |
MI | Myocardial Infarction |
HF | Heart Failure |
SCD | Sudden Cardiac Death |
TIA | Transient Ischemic Attack |
LMCA | Left Main Coronary Artery |
LAD | Left Anterior Descending |
RCA | Right Coronary Artery |
EF | Ejection Fraction |
LV | Left Ventricle |
CMR | Cardiac Magnetic Resonance |
iFR | Instantaneous Wave-free Ratio |
| [1] | Joanna C. E. Lim, Andy Beale & Steve Ramcharitar: Anomalous origination of a coronary artery from the opposite sinus. Nature Reviews Cardiology. 2011, 8: 706-719. |
| [2] | RM Reul, DA Cooley, GL Hallman, et al.: Clinical articles: surgical treatment of coronary artery anomalies: report of a 37½-year experience at the Texas Heart Institute. Texas Heart Institute Journal. 2002, 29: 299. |
| [3] | Allen J. Taylor, John P. Byers, Melvin D. Cheitlin, et al.: Anomalous right or left coronary artery from the contralateral coronary sinus: "high-risk" abnormalities in the initial coronary artery course and heterogeneous clinical outcomes. American Heart Journal. 1997, 133: 428-435. |
| [4] | Michael B. Selig and Nercy Jafari: Anomalous origin of the left main coronary artery from the right coronary artery ostium-interarterial subtype: Angiographic definition and surgical treatment. Catheterization and cardiovascular diagnosis. 1994, 31: 41-47. |
| [5] | Paolo Angelini: Coronary artery anomalies: an entity in search of an identity. Circulation. 2007, 115: 1296-1305. |
| [6] | Felipe S. Torres, Elsie T. Nguyen, Carole J. Dennie, et al.: Role of MDCT coronary angiography in the evaluation of septal vs interarterial course of anomalous left coronary arteries. Journal of Cardiovascular Computed Tomography. 2010, 4: 246-254. |
| [7] | WC Roberts, BS Dicicco, BF Waller, et al.: Origin of the left main from the right coronary artery or from the right aortic sinus with intramyocardial tunneling to the left side of the heart via the ventricular septum. The case against clinical significance of myocardial bridge or coronary tunnel. American Heart Journal. 1982, 104: 303-305. |
| [8] | Tetiana Glushko, Richard Seifert, Fraser Brown, et al.: Transseptal course of anomalous left main coronary artery originating from single right coronary orifice presenting as unstable angina. Radiology case reports. 2018, 13: 549-554. |
| [9] | Adam H Jacobi, Arash Gohari, Benjamin Zalta, et al.: Ventricular myocardial fat: CT findings and clinical correlates. Journal of Thoracic Imaging. 2007, 22: 130-135. |
| [10] | Aidan R. Raney, Farhood Saremi, Satish Kenchaiah, et al.: Multidetector computed tomography shows intramyocardial fat deposition. Journal of Cardiovascular Computed Tomography. 2008, 2: 152-163. |
| [11] | James W. Goldfarb, Sheeba Arnold, Marguerite Roth, et al.: T1-weighted magnetic resonance imaging shows fatty deposition after myocardial infarction. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2007, 57: 828-834. |
| [12] | Yasutaka Ichikawa, Kakuya Kitagawa, Shuji Chino, et al.: Adipose tissue detected by multislice computed tomography in patients after myocardial infarction. JACC: Cardiovascular Imaging. 2009, 2: 548-555. |
| [13] | Maurice B. Bizino, Qian Tao, Jacob Amersfoort, et al.: High spatial resolution free-breathing 3D late gadolinium enhancement cardiac magnetic resonance imaging in ischaemic and non-ischaemic cardiomyopathy: quantitative assessment of scar mass and image quality. European radiology. 2018, 28: 4027-4035. |
| [14] | Goldfarb, J. W., M. Roth, and J. Han: Myocardial fat deposition after left ventricular myocardial infarction: assessment by using MR water-fat separation imaging. Radiology. 2009, 253: 65-73. |
| [15] | Steffen Bohl, Ralf Wassmuth, Hassan Abdel-Aty, et al.: Delayed enhancement cardiac magnetic resonance imaging reveals typical patterns of myocardial injury in patients with various forms of nonischemic heart disease. The international. Journal of cardiovascular imaging. 2008, 24: 597-607. |
| [16] | Kassi, M. and F. Nabi: Role of cardiac MRI in the assessment of nonischemic cardiomyopathies. Methodist DeBakey Cardiovascular Journal. 2013, 9: 149. |
| [17] | Lerin C McCray, Delvise T Fogwe, Kul Aggarwal, et al.: Novel Assessment of Ischemia in Patients With Anomalous Right Coronary Artery. JACC: Case Reports. 2019, 1: 819-822. |
| [18] | Giuseppe Tarantini, Alberto Barioli, Luca Nai Fovino, et al.: Unmasking myocardial bridge-related ischemia by intracoronary functional evaluation. Circulation: Cardiovascular Interventions. 2018, 11: 006247. |
| [19] | Sherif E. Moustafa, Kenton Zehr, Martina Mookadam, et al.: Anomalous interarterial left coronary artery: an evidence based systematic overview. International journal of cardiology. 2008, 126: 13-20. |
| [20] | Peter C. Frommelt, Michele A. Frommelt, MD, James S. Tweddell, et al.: Prospective echocardiographic diagnosis and surgical repair of anomalous origin of a coronary artery from the opposite sinus with an interarterial course. Journal of the American College of Cardiology. 2003, 42: 148-154. |
APA Style
Rodriguez, A. P., Dyal, M., Schob, A., Vicenty-Rivera, S., Jr, J. C. I. (2025). Beyond Benign or Malignant: A Complex Case of Anomalous Left Main Coronary Artery with Transseptal Course. Cardiology and Cardiovascular Research, 9(2), 69-74. https://doi.org/10.11648/j.ccr.20250902.15
ACS Style
Rodriguez, A. P.; Dyal, M.; Schob, A.; Vicenty-Rivera, S.; Jr, J. C. I. Beyond Benign or Malignant: A Complex Case of Anomalous Left Main Coronary Artery with Transseptal Course. Cardiol. Cardiovasc. Res. 2025, 9(2), 69-74. doi: 10.11648/j.ccr.20250902.15
@article{10.11648/j.ccr.20250902.15,
author = {Alex Philip Rodriguez and Michael Dyal and Alan Schob and Sonia Vicenty-Rivera and Juan Carlos Infante Jr},
title = {Beyond Benign or Malignant: A Complex Case of Anomalous Left Main Coronary Artery with Transseptal Course
},
journal = {Cardiology and Cardiovascular Research},
volume = {9},
number = {2},
pages = {69-74},
doi = {10.11648/j.ccr.20250902.15},
url = {https://doi.org/10.11648/j.ccr.20250902.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20250902.15},
abstract = {Anomalous coronary arteries (ACA) represent a heterogeneous group of anatomical variants with a wide range of clinical implications. While many are benign, specific courses may predispose to ischemia, myocardial infarction, heart failure, or sudden cardiac death. We present a rare case of a 62-year-old man with an anomalous left main (LM) coronary artery originating from a shared right coronary ostium, demonstrating a mixed interarterial and transseptal course. Multimodality imaging with cardiac CT angiography (CTA), cardiac magnetic resonance imaging (CMR), and invasive coronary angiography with intravascular ultrasound (IVUS) and physiologic assessment revealed dynamic systolic compression of a prominent first septal perforator, associated with mid-myocardial fibrofatty infiltration and fibrosis. Resting hemodynamics were normal; however, provocative maneuvers elicited significant ischemia as evidenced by abnormal instantaneous wave-free ratio (iFR) changes. Despite the anatomical complexity and hemodynamic findings, the patient opted for conservative management following a detailed discussion of surgical revascularization options. This case highlights the nuanced spectrum of clinical significance in anomalous LM coronary arteries, challenging the traditional benign versus malignant classification. Comprehensive anatomical and physiological evaluation is critical, especially in mixed-course anomalies. Our findings underscore the role of multimodal imaging modalities and functional testing in guiding individualized patient management in rare coronary anomalies.
},
year = {2025}
}
TY - JOUR T1 - Beyond Benign or Malignant: A Complex Case of Anomalous Left Main Coronary Artery with Transseptal Course AU - Alex Philip Rodriguez AU - Michael Dyal AU - Alan Schob AU - Sonia Vicenty-Rivera AU - Juan Carlos Infante Jr Y1 - 2025/06/23 PY - 2025 N1 - https://doi.org/10.11648/j.ccr.20250902.15 DO - 10.11648/j.ccr.20250902.15 T2 - Cardiology and Cardiovascular Research JF - Cardiology and Cardiovascular Research JO - Cardiology and Cardiovascular Research SP - 69 EP - 74 PB - Science Publishing Group SN - 2578-8914 UR - https://doi.org/10.11648/j.ccr.20250902.15 AB - Anomalous coronary arteries (ACA) represent a heterogeneous group of anatomical variants with a wide range of clinical implications. While many are benign, specific courses may predispose to ischemia, myocardial infarction, heart failure, or sudden cardiac death. We present a rare case of a 62-year-old man with an anomalous left main (LM) coronary artery originating from a shared right coronary ostium, demonstrating a mixed interarterial and transseptal course. Multimodality imaging with cardiac CT angiography (CTA), cardiac magnetic resonance imaging (CMR), and invasive coronary angiography with intravascular ultrasound (IVUS) and physiologic assessment revealed dynamic systolic compression of a prominent first septal perforator, associated with mid-myocardial fibrofatty infiltration and fibrosis. Resting hemodynamics were normal; however, provocative maneuvers elicited significant ischemia as evidenced by abnormal instantaneous wave-free ratio (iFR) changes. Despite the anatomical complexity and hemodynamic findings, the patient opted for conservative management following a detailed discussion of surgical revascularization options. This case highlights the nuanced spectrum of clinical significance in anomalous LM coronary arteries, challenging the traditional benign versus malignant classification. Comprehensive anatomical and physiological evaluation is critical, especially in mixed-course anomalies. Our findings underscore the role of multimodal imaging modalities and functional testing in guiding individualized patient management in rare coronary anomalies. VL - 9 IS - 2 ER -
Specialty Medicine Department, Cardiology Section, Bruce W. Carter, VA Healthcare System Department of Veterans Affairs, Miami, Florida, USA
Specialty Medicine Department, Cardiology Section, Bruce W. Carter, VA Healthcare System Department of Veterans Affairs, Miami, Florida, USA
Specialty Medicine Department, Cardiology Section, Bruce W. Carter, VA Healthcare System Department of Veterans Affairs, Miami, Florida, USA
Specialty Medicine Department, Cardiology Section, Bruce W. Carter, VA Healthcare System Department of Veterans Affairs, Miami, Florida, USA
Radiology Department, Pediatric Specialty, Nicklaus Children’s Hospital, University of Miami, Miami, Florida, USA
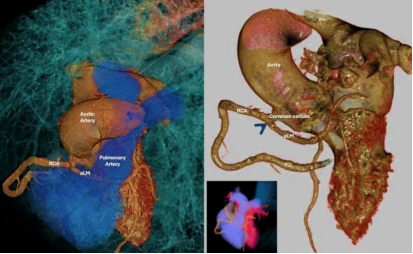
Figure 1. Coronary CTA 3D reconstruction. The blue arrow shows the left main coronary artery has a common ostium with right coronary artery with a transeptal course running in between the aortic and pulmonary arteries.
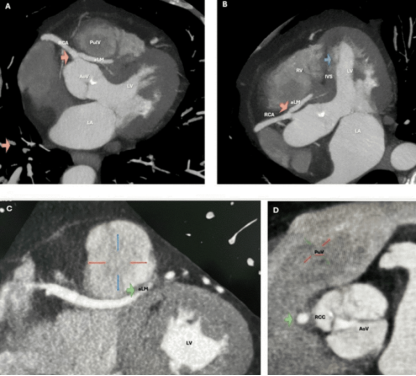
Figure 2. Cardiac CTA performed to exclude intracardiac embolic. On figure 1A, 1C, and 1D the LM and RCA share a common ostium (orange arrow) with LM running through a caudal course towards the pulmonary valve. On figure 1B, demonstrates a focus of fat-equivalent hypoattenuation in the interventricular septum, most consistent with intramyocardial fat (blue arrow).
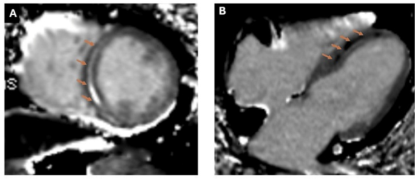
Figure 3. Cardiac magnetic resonance. 3A LGE-SAX (orange arrows) demonstrating fat saturation and 2B Four-chamber-LGE (orange arrows) disclosing areas of fibrofatty infiltration of the interventricular septum.
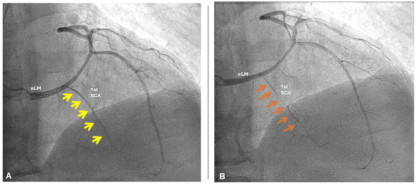
Figure 4. A. Coronary angiography with aLM giving LAD with patent S1 artery during diastole (yellow arrows) and systolic occlusion (orange arrows).
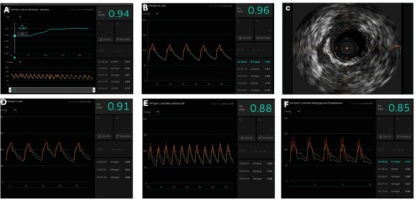
Figure 5. Flow reserve study with IFR/FFR run.
Information

