Dentoalveolar fracture (DAF) is a common injury which comprises of alveolar fractures which include 2-8% of facial fractures. Traditional methods of management of these fractures may not be feasible all the time. The aim of this study is to evaluate the efficiency of transgingival lag screws (TGLS) in management of dentoalveolar fractures. 20 patients with dentoalveolar fractures, either isolated or concomitant with other facial fractures were included in the study. All patients were treated using transgingival lagscrews under local or general anaesthesia and were evaluated for stability, reduction, bone loss, periodontal health and functional rehabilitation with a follow up period of 3 months. All the subjects healed without any complications. The screws were retrieved by the end of 3rd month. A descriptive statistical analysis was done for the assessed parameters. Good fracture stability was noted in 90% of the cases in immediate post operative period. Anatomical reduction assessed radiographically was ideal. Sound periodontal health was maintained effortlessly, inversely reflecting on minimal bone loss. Rehabilitative period was minimal with preinjury average bite force establishment by the end of 3 months. The study concluded that TGLS is an effective alternative to achieve reduction and stabilization in management of dentoalveolar fractures without jeopardizing the blood supply.
| Published in | International Journal of Clinical Oral and Maxillofacial Surgery (Volume 11, Issue 1) |
| DOI | 10.11648/j.ijcoms.20251101.12 |
| Page(s) | 14-20 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Dentoalveolar Fractures, Facial Fractures, Lag Screw, Transgingival
DAF | Dentoalveolar Fracture |
TGLS | Transgingival Lag Screw |
MMF | Maxillo-Mandibular Fixation |
IMF | Intermaxillary Fixation |
Absent n (%) | Present n (%) | P value | |
|---|---|---|---|
Pre operative | 20 (100) | - | |
1 week | 2 (10) | 18 (90) | 0.001 |
1 month | - | 20 (100) | 0.001 |
3 months | - | 20 (100) | 0.001 |
Absent n (%) | Present n (%) | P value | |
|---|---|---|---|
Pre operative | 19 (95) | 1 (5) | |
1 week | 18 (90) | 2 (10) | 1.00 |
1 month | 20 (100) | - | 0.50 |
3 months | 20 (100) | - | 0.50 |
| [1] | Nyárády Z, Orsi E, Nagy K, Olasz L, Nyárády J. Transgingival lag-screw osteosynthesis of alveolar process fracture. International journal of oral and maxillofacial surgery. 2010 Aug 1; 39(8): 779-82. |
| [2] | Rahpeyma A, Khajehahmadi S. Apical Force Application in the Management of Dentoalveolar Fractures: Indications, Procedure and Limitations. Journal of Dental Materials and Techniques. 2015 Sep 1; 4(3): 115-6. |
| [3] | MacLeod SP, Rudd TC. Update on the management of dentoalveolar trauma. Current opinion in otolaryngology & head and neck surgery. 2012 Aug 1; 20(4): 318-24. |
| [4] | Sharma A, Rastogi S, Shukla M, Choudhury R, Tripathi S, Iqbal J. Use of transgingival lag screw osteosynthesis in the management of alveolar process fracture. Craniomaxillofacial Trauma & Reconstruction. 2019 Mar; 12(1): 27-33 |
| [5] | Glendor UL. Aetiology and risk factors related to traumatic dental injuries–a review of the literature. Dental traumatology. 2009 Feb; 25(1): 19-31. |
| [6] | Oikarinen K, Kassila D. Causes and types of traumatic tooth injuries treated in a public dental health clinic. Dental Traumatology. 1987 Aug; 3(4): 172-7. |
| [7] | RamosJorge ML, Peres MA, Traebert J, Ghisi CZ, De Paiva SM, Pordeus IA, Marques LS. Incidence of dental trauma among adolescents: a prospective cohort study. Dental Traumatology. 2008 Apr; 24(2): 159-63. |
| [8] | Purohit J, Kumar GJ, Datta A, Maiti S, Hinge A, Kapoor S, Tiwari RV. Recent advances & historical management in dentoalveolar fracture-A review. Journal of Advanced Medical and Dental Sciences Research. 2020; 8(1): 129-36. |
| [9] | Kasatwar JNA, Surana S, Rajanikanth K, Kala A, Dakshinkar P. Management of dento-alveolar fractures with trans-gingival lag screws: a novel technique. International Journal of Medical and Oral Research. 2017; 2(2): 1–6. |
| [10] | Gibbons AJ. Bone screw stabilization of a dentoalveolar fracture. Journal of oral and maxillofacial surgery. 2007 Jul 1; 65(7): 1439. |
| [11] | Qureshi AA, Reddy UK, Warad NM, Badal S, Jamadar AA, Qurishi N. Intermaxillary fixation screws versus Erich arch bars in mandibular fractures: A comparative study and review of literature. Annals of maxillofacial surgery. 2016 Jan 1; 6(1): 25-30. |
| [12] | Li Z, Hu TQ, Li ZB. Open reduction by vestibular approach in the treatment of segmental alveolar fracture. Dental Traumatology. 2012 Dec; 28(6): 470-3. |
| [13] | Brons R, Boering G. Fractures of the mandibular body treated by stable internal fixation: a preliminary report. Journal of oral surgery (American Dental Association: 1965). 1970 Jun; 28(6): 407-15. |
| [14] | Elsayed SA. Cortical lag screw fixation for the management of mandibular injuries. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2020 Dec 31; 46(6): 393-402. |
| [15] | Niederdellmann H, UHLIG G. Lag-screw osteosynthesis: a new procedure for treating fractures of the mandibular angle. |
| [16] | Chotkowski G, Eggleston TI, Buchbinder D. Lag screw fixation of a nonstable zygomatic complex fracture: case report. Journal of oral and maxillofacial surgery. 1997 Feb 1; 55(2): 183-5. |
| [17] | Rao E, Naveen S, Rao RC, Kollabathula K, Srirambhatla M, Gandham S. Principle of lag-screw fixation in mandibular trauma. Journal of International Society of Preventive and Community Dentistry. 2019 May 1; 9(3): 282-9. |
| [18] | Zachariades N, Mezitis M, Papademetriou I. Use of lag screws for the management of mandibular trauma. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 1996 Feb 1; 81(2): 164-7. |
| [19] | Coburn DG, Kennedy DW, Hodder SC. Complications with intermaxillary fixation screws in the management of fractured mandibles. British Journal of Oral and Maxillofacial Surgery. 2002 Jun 1; 40(3): 241-3. |
| [20] | Nandini GD, Balakrishna R, Rao J. Self tapping screws v/s Erich arch bar for inter maxillary fixation: a comparative clinical study in the treatment of mandibular fractures. Journal of maxillofacial and oral surgery. 2011 Jun; 10: 127-31. |
| [21] | Jain A, Taneja S, Rai A. What is a better modality of maxillomandibular fixation: bone-supported arch bars or Erich arch bars? A systematic review and meta-analysis. British Journal of Oral and Maxillofacial Surgery. 2021 Oct 1; 59(8): 858-66. |
| [22] | Burman S, Lal B, Alagarsamy R, Kumar J, Ankush A, Rai AJ, Yunus M. Evidence-based management of isolated dentoalveolar fractures: a systematic review. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2024 Jun 1; 50(3): 123-33. |
| [23] | Majumdar A, Brook IM. Iatrogenic injury caused by intermaxillary fixation screws. The British Journal of Oral & Maxillofacial Surgery. 2002 Feb 1; 40(1): 84-5. |
APA Style
Patel, A., Gowda, G., Pushpa, S. S., Bhat, P., Shetty, S. (2025). A Prospective Clinical Study on Transgingival Lag Screws for Management of Dentoalveolar Fractures. International Journal of Clinical Oral and Maxillofacial Surgery, 11(1), 14-20. https://doi.org/10.11648/j.ijcoms.20251101.12
ACS Style
Patel, A.; Gowda, G.; Pushpa, S. S.; Bhat, P.; Shetty, S. A Prospective Clinical Study on Transgingival Lag Screws for Management of Dentoalveolar Fractures. Int. J. Clin. Oral Maxillofac. Surg. 2025, 11(1), 14-20. doi: 10.11648/j.ijcoms.20251101.12
@article{10.11648/j.ijcoms.20251101.12,
author = {Abhinandan Patel and Girish Gowda and Sirisha Sampangi Pushpa and Preethi Bhat and Siri Shetty},
title = {A Prospective Clinical Study on Transgingival Lag Screws for Management of Dentoalveolar Fractures
},
journal = {International Journal of Clinical Oral and Maxillofacial Surgery},
volume = {11},
number = {1},
pages = {14-20},
doi = {10.11648/j.ijcoms.20251101.12},
url = {https://doi.org/10.11648/j.ijcoms.20251101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcoms.20251101.12},
abstract = {Dentoalveolar fracture (DAF) is a common injury which comprises of alveolar fractures which include 2-8% of facial fractures. Traditional methods of management of these fractures may not be feasible all the time. The aim of this study is to evaluate the efficiency of transgingival lag screws (TGLS) in management of dentoalveolar fractures. 20 patients with dentoalveolar fractures, either isolated or concomitant with other facial fractures were included in the study. All patients were treated using transgingival lagscrews under local or general anaesthesia and were evaluated for stability, reduction, bone loss, periodontal health and functional rehabilitation with a follow up period of 3 months. All the subjects healed without any complications. The screws were retrieved by the end of 3rd month. A descriptive statistical analysis was done for the assessed parameters. Good fracture stability was noted in 90% of the cases in immediate post operative period. Anatomical reduction assessed radiographically was ideal. Sound periodontal health was maintained effortlessly, inversely reflecting on minimal bone loss. Rehabilitative period was minimal with preinjury average bite force establishment by the end of 3 months. The study concluded that TGLS is an effective alternative to achieve reduction and stabilization in management of dentoalveolar fractures without jeopardizing the blood supply.
},
year = {2025}
}
TY - JOUR T1 - A Prospective Clinical Study on Transgingival Lag Screws for Management of Dentoalveolar Fractures AU - Abhinandan Patel AU - Girish Gowda AU - Sirisha Sampangi Pushpa AU - Preethi Bhat AU - Siri Shetty Y1 - 2025/04/14 PY - 2025 N1 - https://doi.org/10.11648/j.ijcoms.20251101.12 DO - 10.11648/j.ijcoms.20251101.12 T2 - International Journal of Clinical Oral and Maxillofacial Surgery JF - International Journal of Clinical Oral and Maxillofacial Surgery JO - International Journal of Clinical Oral and Maxillofacial Surgery SP - 14 EP - 20 PB - Science Publishing Group SN - 2472-1344 UR - https://doi.org/10.11648/j.ijcoms.20251101.12 AB - Dentoalveolar fracture (DAF) is a common injury which comprises of alveolar fractures which include 2-8% of facial fractures. Traditional methods of management of these fractures may not be feasible all the time. The aim of this study is to evaluate the efficiency of transgingival lag screws (TGLS) in management of dentoalveolar fractures. 20 patients with dentoalveolar fractures, either isolated or concomitant with other facial fractures were included in the study. All patients were treated using transgingival lagscrews under local or general anaesthesia and were evaluated for stability, reduction, bone loss, periodontal health and functional rehabilitation with a follow up period of 3 months. All the subjects healed without any complications. The screws were retrieved by the end of 3rd month. A descriptive statistical analysis was done for the assessed parameters. Good fracture stability was noted in 90% of the cases in immediate post operative period. Anatomical reduction assessed radiographically was ideal. Sound periodontal health was maintained effortlessly, inversely reflecting on minimal bone loss. Rehabilitative period was minimal with preinjury average bite force establishment by the end of 3 months. The study concluded that TGLS is an effective alternative to achieve reduction and stabilization in management of dentoalveolar fractures without jeopardizing the blood supply. VL - 11 IS - 1 ER -
Department of Facio-Maxillary Surgery, Sanjay Gandhi Institue of Trauma and Orthopaedics, Bengaluru, India
Department of Facio-Maxillary Surgery, Sanjay Gandhi Institue of Trauma and Orthopaedics, Bengaluru, India
Department of Facio-Maxillary Surgery, Sanjay Gandhi Institue of Trauma and Orthopaedics, Bengaluru, India
Biography: Sirisha Sampangi Pushpa, a Fellow in the Department of Facio-Maxillary Surgery currently pursuing fellowship in Maxillo-facial trauma at the Sanjay Gandhi Institute of Trauma and Ortho-paedics. Completed her Master in Oral and Maxillofacial Surgery in the year 2023. She is well-versed in managing complex trauma cases. Her primary focus and passion lies in emergency care, working diligently to provide timely and effective management for patients with facial injuries. In addition to trauma, her extended interests extend to minor surgical procedures and maxillofacial cleft surgeries.
Research Fields: Minor surgeries, Oral pathology, Maxillofacial trauma, Craniofacial reconstruction, Implantology, Regenerative medicine, Anaesthesia and Pain management

Department of Facio-Maxillary Surgery, Sanjay Gandhi Institue of Trauma and Orthopaedics, Bengaluru, India
Department of Facio-Maxillary Surgery, Sanjay Gandhi Institue of Trauma and Orthopaedics, Bengaluru, India

Figure 1. Transgingival lag screws of different sizes.

Figure 2. Pre-operative radiograph.

Figure 3. Intra-operative photograph after TGLS placement.
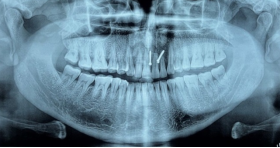
Figure 4. Post-operative Orthopantomogram.

Figure 5. Post-operative photograph after TGLS removal with re-established occlusion.
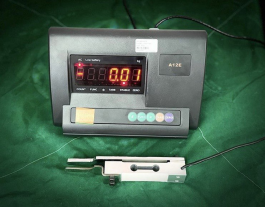
Figure 6. Bite force device.

Figure 7. Bite force assessment.
Information

