Abstract
The direct impact of the COVID-19 pandemic and the indirect impact of the ensuing economic and political response have affected the United States on a large scale. We document a substantial surge in anxiety and depression symptoms from 2019 to 2020 driven by the young adult population, indicating a disproportional indirect impact on the young. Multivariate regression analysis was utilized to quantify the stringency of state responses’ indirect effect on the changes in anxiety or depression symptoms during the pandemic. While we observe a slight decline in the share of the adult population experiencing anxiety and depression through July 2021- June 2022, such decline does not compensate for the large surge of mental health issues among young adults in 2020. Overall, our results indicate that the effects of the stringency of the mitigation measures on different areas of health are complex and vary by state, with a wide variation of mental health-related issues by age group and a higher prevalence in younger adult age categories. After discussing inequities in the accessibility of mental health treatment, lack of health insurance, and implications for quality of life among young adults, this paper adds to the breadth of ongoing COVID-19 research and emphasizes the importance of considering the overall health of the population in a large-scale health crisis as well as discussing the potential unintended consequences of the mitigation measures put in place.
Keywords
COVID-19, Anxiety, Depression, Pandemic Response, Stringency Index, Lifestyle, Young Adults
1. Introduction
On March 11, 2020, the World Health Organization declared the outbreak of COVID-19 a global pandemic
. The world suffered both from the outbreak and the ensuing response, as many were isolated in their homes for significant periods of time
. Disentangling the effects of the SARS-CoV-2 virus from the response taken to prevent its transmission is still subject to considerable research. This paper investigates the issue in the context of mental health among the U.S. young adult population.
In the United States, a nationwide emergency was declared on March 13, and the immediate policy response was to “shut down” the country. The Center for Disease Control and Prevention (CDC) issued a “No Sail Order” to all cruises in U.S. waters and New York City closed its public school system, affecting over 1 million students. Between March and May of 2020, all other U.S. states shut down. Forty-three U.S. states issued explicit stay-at-home orders for nonessential activities. The other seven states (Arkansas, Iowa, Nebraska, North Dakota, South Dakota, Utah, and Wyoming) issued executive orders restricting social gatherings and closing malls, restaurants, theaters, gyms, and schools, and adhered to CDC recommendations
.
The widespread pandemic-response strategy prioritized safeguarding the physical health of individuals by protecting them from getting infected by the SARS-CoV-2 virus. This strategy neglected the mental health of the population, specifically the young. While mental health was mentioned by the WHO for its connection with the pandemic, the considerations were vague and limited to uplifting messages and recommendations to the population
. Rigorous mental health considerations were absent in the policies taken by governments and government officials.
The consequences of such omission are dangerous and potentially catastrophic, leading to a concerning cycle of adverse mental health effects. Researchers have already documented the necessity for additional mental health services because of the ensuing psychological trauma resulting from COVID-19, both from the lockdown itself and the related worldly changes afterward, including an increased risk of violence
| [9] | Pereira-Sanchez, Victor, Frances Adiukwu, Samer El Hayek, Drita Gashi Bytyçi, Jairo M. Gonzalez-Diaz, Ganesh Kudva Kundadak, Amine Larnaout, et al. 2020. “COVID-19 Effect on Mental Health: Patients and Workforce.” The Lancet Psychiatry 7 (6): e29–30. https://doi.org/10.1016/S2215-0366(20)30153-X |
| [10] | Kim, Andrew Wooyoung, Tawanda Nyengerai, and Emily Mendenhall. 2022. “Evaluating the Mental Health Impacts of the COVID-19 Pandemic: Perceived Risk of COVID-19 Infection and Childhood Trauma Predict Adult Depressive Symptoms in Urban South Africa.” Psychological Medicine 52 (8): 1587–99. https://doi.org/10.1017/S0033291720003414 |
| [11] | Jonathan M Metzl. 2015. “Gun Violence, Stigma, and Mental Illness: Clinical Implications.” March 25, 2015. https://www.psychiatrictimes.com/view/gun-violence-stigma-and-mental-illness-clinical-implications |
[9-11]
. We assert that while government policies were intended to limit the SARS-CoV-2 virus transmission, they also limited individuals from taking care of themselves and other potential ailments, scheduling regular doctor visits, outdoor activities, visiting friends and family, etc., with severe mental health unintended outcomes. In this paper, we investigate these outcomes by age groups and across the 50 U.S. states and associate them with the stringency of the policy response in each state.
We find a negative effect on mental health, specifically in young adults (18-29 years), driving up the reported anxiety and depression symptoms for the whole U.S. population in 2020. Our findings suggest that the response to COVID-19 caused a “pandemic of mental health” – rapidly spreading mental health ailments throughout the country in 2020. While many factors influence this new “pandemic,” our analysis indicates that the approach taken by different U.S. states, and not the SARS-CoV-2 virus alone, caused an upsurge in a multitude of mental health categories including anxiety and depression, as well as a potential increase in unemployment, gun violence, and mass shootings.
Nevertheless, regression analysis indicates that the stringency of the response, including both the initial containment and the subsequent economic relief, health system, and vaccination policies, had a significant effect in reducing peak anxiety and depression levels accrued during the first year of the pandemic. Although the reduction is small in magnitude and not yet close to pre-outbreak levels, it is statistically significant and an encouraging sign. Our findings are consistent with the effect of social climate and financial concerns associated with the COVID-19 pandemic
| [12] | Cindy H Liu, Ga Tin Finneas Wong, Sunah Hyun, and Hyeouk Chris Hahm. 2022. “Concerns about the Social Climate, Finances, and COVID-19 Risk on Depression and Anxiety: An Analysis on U.S. Young Adults across Two Waves - PubMed.” April 2022. https://pubmed.ncbi.nlm.nih.gov/35189512/ |
[12]
.
In sum, our analysis suggests that the pandemic had complex and multidimensional effects on overall health. While the SARS-CoV-2 virus had a direct impact on the health (both physical and mental health) of the old population, the policy response to the virus had a disproportionate, yet indirect, impact on the mental health of young adults. This indirect impact comes with complex and dangerous ramifications for our society.
2. Methods
The National Center for Health Statistics (NCHS) partnered with the U.S. Census Bureau on an experimental data platform called the Household Pulse Survey in order to provide information about the impact of the COVID-19 pandemic in the United States. Specifically, the influence of the COVID-19 pandemic on “employment status, consumer spending, food security, housing, education disruptions, and dimensions of physical and mental wellness” (U.S. Census Bureau, Household Pulse Survey). The data collection began on April 23, 2020. Through the survey, several topics were covered regarding mental health, including anxiety, depression, and mental health care.
In the Household Pulse Survey, questions were asked to gain information on the frequency of anxiety and depression symptoms over seven-day periods throughout the pandemic. The questions were adapted from the two-item Patient Health Questionnaire (PHQ-2) and the two-item Generalized Anxiety Disorder (GAD-2) scale.
The adapted PHQ-2 questions include:
“Over the last 7 days, how often have you been bothered by … having little interest or pleasure in doing things? Would you say not at all, several days, more than half the days, or nearly every day? Select only one answer.”
“Over the last 7 days, how often have you been bothered by … feeling down, depressed, or hopeless? Would you say not at all, several days, more than half the days, or nearly every day? Select only one answer.”
The adapted GAD-2 questions include:
“Over the last 7 days, how often have you been bothered by the following problems … Feeling nervous, anxious, or on edge? Would you say not at all, several days, more than half the days, or nearly every day? Select only one answer.”
“Over the last 7 days, how often have you been bothered by the following problems … Not being able to stop or control worrying? Would you say not at all, several days, more than half the days, or nearly every day? Select only one answer.”
For each question, the answer choices were given a numerical value: “not at all = 0, several days = 1, more than half the days = 2, and nearly every day = 3.” To calculate the individual’s score, their responses to the PHQ-2 and GAD-2 questionnaires are added together. On the PHQ-2, a sum score of three or greater is associated with major depressive disorder. On the GAD-2, a sum score of three or greater is associated with generalized anxiety disorder. When adults score above three, it is recommended that they are evaluated by a health professional.
In order to compare anxiety or depression reported symptoms rates from before and after the pandemic, data from the 2019 National Health Interview Survey were compared with 2020 data from the Household Pulse Survey. Because data from January 2020 to April 2020 are unavailable, only the months of May through December of both 2019 and 2020 are compared. The same questions from the PHQ-2 and GAD-2 questionnaires were used to ensure comparability in the anxiety or depression reported symptoms in 2019 and 2020.
To disentangle the direct and indirect impacts of the SARS-CoV-2 virus on mental health, we first analyze the changes in anxiety and depression in the U.S. from 2019 to 2020, and then disaggregate the analysis by age. Since COVID-19 affected disproportionally the older population relative to the younger population, it is natural to expect that the direct impact of the virus on changes in anxiety and depression before and after the pandemic is disproportionally larger in older-age categories
| [13] | Shahid, Zainab, Ricci Kalayanamitra, Brendan McClafferty, Douglas Kepko, Devyani Ramgobin, Ravi Patel, Chander Shekher Aggarwal, et al. 2020. “COVID-19 and Older Adults: What We Know.” Journal of the American Geriatrics Society 68(5): 926–29. https://doi.org/10.1111/jgs.16472 |
| [14] | Yanez, N. David, Noel S. Weiss, Jacques-André Romand, and Miriam M. Treggiari. 2020. “COVID-19 Mortality Risk for Older Men and Women.” BMC Public Health 20(1): 1742. https://doi.org/10.1186/s12889-020-09826-8 |
| [15] | Caramelo, F., N. Ferreira, and B. Oliveiros. 2020. “Estimation of Risk Factors for COVID-19 Mortality - Preliminary Results.” medRxiv. https://doi.org/10.1101/2020.02.24.20027268 |
[13-15]
. Since we only observe the total impact (
i.e., the direct plus indirect impact combined) of the virus on mental health, any difference between the observed and expected effects must be attributed to the indirect channel.
To investigate the indirect channel further, we define and analyze the human response to the SARS-CoV-2 virus. By “human response” we mean the indirect effect on mental health through human actions propitiated by the virus. If it is not the SARS-CoV-2 virus alone driving the changes in anxiety and depression across age categories and in particular the younger generations, it must be the human response accompanying the virus.
We subdivide the “human response” into formal and informal responses. Formal responses include policies, laws, executive orders, mandates, stimulus bills, and actions formally enacted by governments, government officials, and official organizations, comparable to recommendations issued by the CDC. Informal responses include unspoken norms, beliefs, fears, and behaviors that have shaped the interactions among individuals since March 2020. While the latter is difficult to quantify, it is of paramount importance and requires future investigation. Our analysis will focus on the former, formal human responses, to the extent they can be (imperfectly) quantified.
To investigate the association between the formal response to the pandemic and mental health more thoroughly, we also use correlation and regression analysis. We measure the formal policy response with the stringency index. The stringency index provides a quantitative representation (1-100) to estimate the rigidity of individual state responses to COVID-19 in the United States. Subcategories of the stringency index include virus containment and closure restrictions, economic support, health system mandates, vaccination administration, and other miscellaneous components. All five subcategories are combined into one stringency index value for each U.S. state.
To construct our regression design matrix, the average stringency index from January 2020 to April 2021 was calculated as well as the change in the percentage of the population showing anxiety or depression symptoms in each U.S. state from the pandemic peak period (May/2020 to Jul/2021) to the post-pandemic peak period (Jul/2021 to Jun/2022). We lagged the stringency index (our key explanatory variable) relative to the change in the percentage of the population showing anxiety or depression (our key dependent variable) to minimize reverse causality endogeneity concerns.
3. Results
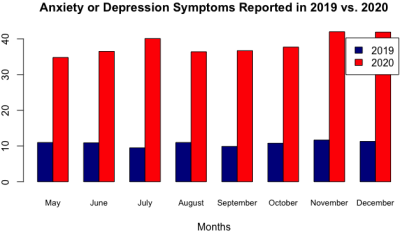
Figure 1 shows that anxiety or depression symptoms increased significantly from about 10 percent in May-December of 2019 to more than 35 percent during May-December of 2020, about a four-fold increase in one year.
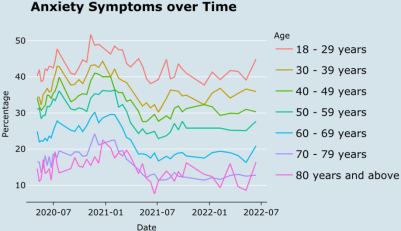
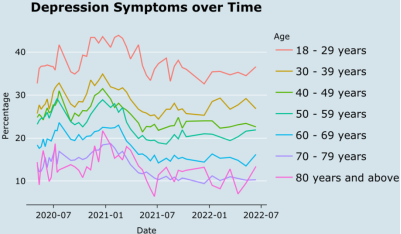
Figures 2 and 3 show the trends in anxiety and depression in varying adult age groups from April 23, 2020, to June 13, 2022, illustrating a large variation in anxiety and depression across age groups and over time. As seen in the figures, young adults (aged 18-29 years) had the highest rates of anxiety and depression throughout the pandemic, while older adults (aged 80 years or above) had the lowest rates of anxiety and depression. In
Figure 3, the depression rates for adults aged 18-29 remain significantly large compared to other age groups throughout the survey collection period. Each age group follows a similar trend of a slight decrease in both anxiety and depression rates from December 2020 to July 2021.
Figures 2 and 3 also reveal that the four-fold increase in mental health symptoms shown in
Figure 1 was driven by the younger generations (18-29 age category mostly). This provides insight into the fundamental cause of the significant increase in mental health problems from 2019 to 2020: It is the indirect channel associated with the human response to the pandemic.
Figure 1. Trends in reported anxiety or depression symptoms from May to December in 2019 and 2020 for adults aged 18-29 years to 80 years and above.
Source: National Health Interview Survey, National Health Center for Statistics, 2019. U.S. Census Bureau, Household Pulse Survey, 2020-2022.
Figure 2. Trends in anxiety symptoms over time for adults aged 18-29 years to 80 years and above. Source: U.S. Census Bureau, Household Pulse Survey, 2020-2022.
Figure 3. Trends in depression symptoms over time for adults aged 18-29 years to 80 years and above. Source: U.S. Census Bureau, Household Pulse Survey, 2020-2022.
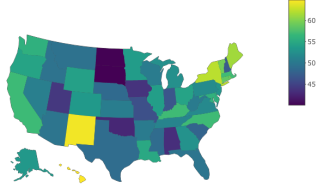
Figure 4. Average stringency index by U.S. states from January 2020 to April 2021. Lighter colors represent a higher stringency index. Source: Oxford Coronavirus Government Response Tracker, 2020-2021.
To investigate this indirect channel,
Figure 4 shows a heatmap of the average stringency index by U.S. states from January 2020 to April 2021. States with a less stringent approach include North Dakota, South Dakota, Utah, Oklahoma, and Alabama. These states had more lenient policy responses and less generous income support. In contrast, northeastern states plus New Mexico, Washington, California, and Hawaii, implemented more stringent policies, specifically regarding facial coverings, with a near two-fold difference in ‘days on average with facial covering requirements in place’
. The varying degree of the stringency index throughout the United States, as seen in
Figure 4, reflects varying U.S. state policies in response to the pandemic.
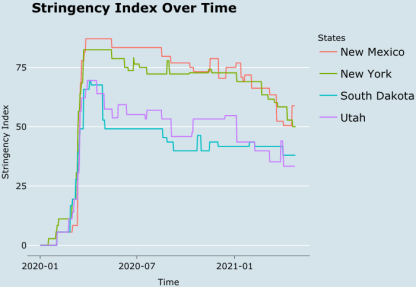
Figure 5 shows the trends in the stringency index for a selection of four U.S. states (New Mexico, New York, South Dakota, and Utah). Until April 2020, every state exhibited a significant spike in the stringency of COVID-19-related policy responses. From this point forward, the variation in the responses widened as states implemented different policies. This observation is consistent with patterns of location and income support documented in the literature that were influenced by weak institutional systems, inadequate funds, and the initial success of government health interventions
.
Figure 5. Trends in stringency index for New Mexico, New York, South Dakota, and Utah from January 2020 to April 2021. Source: Oxford Coronavirus Government Response Tracker, 2020-2021.
Results from our multivariate regression analysis are presented in
Table 1. Column 1 of
Table 1 shows a statistically significant relationship between the stringency index and the change in the percentage of the population showing symptoms of anxiety or depression from the first year of the pandemic to the second year. This significant value of –0.096 (
p<0.01) indicates that U.S. states with higher stringency indices from January 2020 to April 2021 experienced an average reduction in anxiety or depression symptoms between the periods May/2020-Jul/2021 and Jul/2021-Jun/2022.
Column 2 of
Table 1 adds the percentage of the adult population over 65 to the model. Adding this demographic variable means holding it constant in the model when interpreting the other variables. The coefficient for the stringency index became larger in magnitude (-0.100) and remained statistically significant at the 1 percent significance level (
p<0.01).
Column 3 holds constant the annual growth rate of per capita GDP for each state during 2019-2022. As a result, the coefficient associated with the stringency index increased in magnitude and remained significant (p<0.01), confirming the association between the stringency index and mental health during and after the pandemic. Our findings suggest that different COVID-19 pandemic responses across U.S. states impacted changes in adults' mental health as measured by the stringency index.
Table 1. Determinants of Anxiety or Depression during the Pandemic: Multivariate Regression Analysis.
| Dependent variable: |
| Anxiety or Depression Difference Average during Jul 2021–Jun 2022 minus May 2020–Jul 2021 |
| (1) | (2) | (3) | (4) | (5) |
Mean of the Stringency Index | -0.096*** | -0.100*** | -0.114*** | -0.128*** | -0.122*** |
(Jan 2020 – Apr 2021) | (0.033) | (0.034) | (0.032) | (0.030) | (0.032) |
Population Over 65 | | 5.608 | 3.807 | 4.421 | 3.350 |
(% of the Adult Population) | | (9.104) | (8.497) | (7.857) | (8.069) |
Growth Rate of per capita GDP | | | -73.124*** | -68.841*** | -67.535*** |
(Annual Rate During 2019–2022) | | | (25.454) | (23.574) | (23.803) |
All-Cause Mortality Rate | | | | -822.474*** | -775.196*** |
(Jan 2020 – Apr 2021) | | | | (276.778) | (287.465) |
Anxiety and Depression Peak | | | | | -0.043 |
(May 2020 – Jul 2021) | | | | | (0.065) |
Model Intercept | 0.308 | -0.731 | 3.655 | 5.339** | 6.666** |
| (1.735) | (2.428) | (2.727) | (2.584) | (3.279) |
Observations | 50 | 50 | 50 | 50 | 50 |
Adjusted R2 | 0.131 | 0.119 | 0.237 | 0.348 | 0.340 |
Note: | *p<0.1, **p<0.05, ***p<0.01 |
In addition to the percentage of the adult population over 65 years old and the annual growth rate of per capita GDP for each U.S. state, Column 4 also adds the all-cause mortality rate during the first leg of the pandemic (specifically Jan/2020 – Apr/2021). Adding this variable increased the magnitude and significance of the stringency index. The coefficient changed from (-0.114) in column 3 to (-0.128) in column 4.
Finally, the reduction in anxiety and depression levels in the second leg of the pandemic (specifically Jul/2021-Jun/2022) may be associated with the peak of mental health issues accrued during the first leg (prior to July 2021). To investigate this, column 5 also controls for the average anxiety and depression levels from May 2020 to July 2021. Interestingly, the coefficient associated with the Stringency Index remained virtually unchanged and statistically significant (p<0.01). This finding suggests that the reduction in anxiety or depression levels during the second leg of the pandemic was more associated with the stringency index than with the peak mental health issues of the first leg.
The negative coefficient for the Stringency Index is an encouraging sign, indicating that the response was eventually associated with a reduction in anxiety or depression levels after July 2021. This finding may be explained by the economic relief and stimulus packages that were subsequently included in the stringency index, improving the social climate and reducing financial concerns for U.S. families and by the public perception of stringency
| [12] | Cindy H Liu, Ga Tin Finneas Wong, Sunah Hyun, and Hyeouk Chris Hahm. 2022. “Concerns about the Social Climate, Finances, and COVID-19 Risk on Depression and Anxiety: An Analysis on U.S. Young Adults across Two Waves - PubMed.” April 2022. https://pubmed.ncbi.nlm.nih.gov/35189512/ |
| [18] | Lee, Sanguk, Tai-Quan Peng, Maria Knight Lapinski, Monique Mitchell Turner, Youjin Jang, and Andrea Schaaf. 2021. “Too Stringent or Too Lenient: Antecedents and Consequences of Perceived Stringency of COVID-19 Policies in the United States.” Health Policy OPEN 2 (December): 100047. https://doi.org/10.1016/j.hpopen.2021.100047 |
[12, 18]
. Nevertheless, while the decrease in anxiety or depression levels after July 2021 was statistically significant, it was relatively small in magnitude and not large enough to mitigate the drastic increase from 2019 to 2020. In other words, the anxiety and depression levels as of June 2022 are still far higher than the pre-pandemic levels.
4. Discussion
This paper finds that the mental health of the younger adult population (18-29 years) in the United States was significantly affected by the COVID-19 pandemic, both directly and indirectly. While the approaches of different U.S. states’ pandemic responses varied, the main goal was to protect the health and safety of Americans, specifically the elderly population. We hypothesized that during the pandemic, the older adult population would have the highest reported anxiety and depression symptoms. However, our results indicate a massive surge in reported anxiety and depression symptoms in the younger adult population following the pandemic. This rejects our initial hypothesis that the older adult populations would suffer the greatest from mental health issues due to a greater physical health risk from COVID-19.
Possible explanations for the increase in reported anxiety and depression symptoms of the younger adult population are complex and vary by state. On the one hand, our analysis suggests that the indirect effect of the SARS-CoV-2 virus, categorized as formal and informal human responses, is a vital factor driving the spike in mental health problems among the younger generations. On the other hand, while we recognize that the stringency index is an imperfect measure of the formal response, we find a small (yet statistically significant) reduction in peak anxiety and depression levels during the second year of the pandemic associated with the stringency of the response. The reduction is not close to pre-pandemic levels, suggesting that the informal human response plays a considerable role in understanding mental health and needs further investigation.
Adults aged 18-29 years face the problem of accessibility to mental health treatment, specifically prescription medications as well as counseling and therapy, due to financial limitations and inequitable access
| [19] | Kola, Lola, Brandon A. Kohrt, Bibhav Acharya, Byamah B. Mutamba, Christian Kieling, Manasi Kumar, Charlene Sunkel, Wufang Zhang, and Charlotte Hanlon. 2021. “The Path to Global Equity in Mental Health Care in the Context of COVID-19.” The Lancet 398 (10312): 1670–72. https://doi.org/10.1016/S0140-6736(21)02233-9 |
[19]
. In May 2022, more than 23% of adults aged 18-29 years indicated having taken medications for mental health. This number is almost half of those who indicated having anxiety or depression, and the share needing counseling and therapy is increasing. If the young adult population continues to go untreated for mental health concerns, this age group may struggle with long-term mental health consequences.
Another obstacle that young adults face in receiving mental health treatment is the lack of health insurance coverage. According to the health insurance coverage data from the Household Pulse Survey, 16% of adults aged 18-24 years were uninsured from April 23, 2020, to June 13, 2022, resulting in difficulty treating their declining mental health with prescription medication. In contrast, 8.8% of adults aged 45-64 years were uninsured during the same collection period allowing greater access to prescription medications. That is, the youngest adult population with the greatest need for mental health resources are the most uninsured compared to other age categories, resulting in a major difficulty for this demographic group to access mental health treatments.
Our results also have implications for overall well-being, quality of life, and lifestyle. While these areas are subjective and multidimensional, mental health contributes to them
. Therefore, our results imply a significant drop in the overall quality of life in young adults stemming from the SARS-CoV-2 virus itself and the human response to it. The human response (i.e., the indirect channel) had a substantially larger impact on mental health and the subsequent well-being of the population.
5. Limitations
Our research is limited by the availability of data. Due to pandemic restrictions on the data collection process, it was not possible to obtain a reliable sample for the first few months of the pandemic. Attrition from January 2020-April 2020 implies that our mental health dataset from the Household Pulse Survey starts in May 2020. In addition, the mental health data used in our investigation are self-reported, which lends itself to potential response bias. This could potentially affect the accuracy of our results. For example, if the young are more likely to over-report symptoms than the old following the COVID-19 pandemic, our results would be biased.
There are no other events like the COVID-19 pandemic in recent history. Thus, the potential for comparative analysis is limited, especially when analyzing mental health. Although some comparisons could be made between the COVID-19 and the 1918 Spanish Flu pandemics, the state of the world in 1918 was not comparable to 2020. However, our findings indicate the need for large-scale research of the long-term consequences of the COVID-19 pandemic, both directly and indirectly, on mental health
| [21] | Aknin, Lara B., Jan-Emmanuel De Neve, Elizabeth W. Dunn, Daisy E. Fancourt, Elkhonon Goldberg, John F. Helliwell, Sarah P. Jones, et al. 2022. “Mental Health During the First Year of the COVID-19 Pandemic: A Review and Recommendations for Moving Forward.” Perspectives on Psychological Science 17 (4): 915–36. https://doi.org/10.1177/17456916211029964 |
| [22] | Montesinos-Yufa, H. M., Nagasuru-McKeever, T. (2024). Gender-Specific Mental Health Outcomes in Central America: A Natural Experiment. International Journal on Data Science and Technology, 10(3), 45-50. https://doi.org/10.11648/j.ijdst.20241003.11 |
[21, 22]
. Future research could also forecast the effects of the pandemic over time on mental health, overall health, and society at large.
Other kinds of indirect effects, such as changes in the sentiment of the media on the mood, emotions, behavioral changes, and immune response of the population, are not accounted for. Nevertheless, a systematic decline in the sentiment of major U.S. newspaper during the pandemic has already been documented, with immediate ties to the mental health of their readers
| [23] | Montesinos-Yufa, H. M., Musgrove, E. (2024). A Sentiment Analysis of News Articles Published Before and During the COVID-19 Pandemic. International Journal on Data Science and Technology, 10(2), 38-44. https://doi.org/10.11648/j.ijdst.20241002.13 |
[23]
. Similarly, both direct and indirect effects of the COVID-19 pandemic induced profound behavioral changes that eroded the well-functioning of the immune and metabolic systems, the full understanding of which requires further investigation
. However, with limited exceptions, current research predominantly focuses on the detection, prevention, and treatment of specific diseases, leaving the complexities of maintaining long-term health in the absence of disease, particularly unexplored
| [25] | Cutler W, Kolter J, Chambliss C, O'Neill H, Montesinos-Yufa HM. Long term absence of invasive breast cancer diagnosis in 2,402,672 pre and postmenopausal women: A systematic review and meta-analysis. PLoS One. 2020, Sep 10; 15 (9): e0237925. https://doi.org/10.1371/journal.pone.0237925 PMID: 21496745; PMCID: PMC3137947. |
[25]
.
Finally, the spike in mental health problems can have devastating consequences on modern-day society that need to be investigated further. Preliminary analyses by the authors indicate a dangerous connection between mental health and mass shootings traceable to the pandemic response. The ramifications of mental health problems on violence, civic behavior, lifestyle, culture, and other areas of society require urgent investigation.
Abbreviations
SARS-CoV-2 | Virus That Causes the Coronavirus Disease 2019 (COVID-19) |
COVID-19 | Coronavirus Disease 2019 |
GAD-2 | Two-Item Generalized Anxiety Disorder Questionnaire |
PHQ-2 | Two-Item Patient Health Questionnaire |
Acknowledgments
The authors gratefully acknowledge the support of Ursinus College, its Department of Mathematics, Computer Science and Statistics, the Summer 2023 Ursinus Research Experience with Undergraduates (REU) and Summer Fellows programs, and the Inclusive Data Science and Innovative Research Initiative (IDSIRI). We also extend our thanks to the National Science Foundation for its support through Grant No. 1851948, and to the Mathematical Association of America (MAA) community, particularly those at MathFest 2023, for their valuable feedback.
Author Contributions
Ed Coleman: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Jhavon Innocent: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Sarah Kircher: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Hugo Moisés Montesinos-Yufa: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
McKade Trauger: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Data Availability Statement
All data supporting the findings of this study along with replication keys in R/R-Studio are publicly available at: https://data.mendeley.com/datasets/vmwmn4252k/1
| [26] | Kircher, Sarah; Coleman, Ed; Innocent, Jhavon; Trauger, McKade; Montesinos-Yufa, Hugo (2022), “Data for "A Pandemic of Mental Health"”, Mendeley Data, V1, https://doi.org/10.17632/vmwmn4252k.1 |
[26]
.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
CDC. 2020. “COVID Data Tracker.” Centers for Disease Control and Prevention. March 28, 2020.
https://covid.cdc.gov/covid-data-tracker
|
| [2] |
CDC. 2022. “CDC Museum COVID-19 Timeline.” Centers for Disease Control and Prevention. January 5, 2022.
https://www.cdc.gov/museum/timeline/covid19.html
|
| [3] |
WHO. 2020a. “WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19 - 11 March 2020.” March 11, 2020.
https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020
|
| [4] |
WHO. 2020b. “Mental Health and Psychosocial Considerations during the COVID-19 Outbreak.” World Health Organization, March.
https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf
|
| [5] |
Cucinotta, Domenico, and Maurizio Vanelli. 2020. “WHO Declares COVID-19 a Pandemic.” Acta Bio-Medica: Atenei Parmensis 91 (1): 157–60.
https://doi.org/10.23750/abm.v91i1.9397
|
| [6] |
Mareike Ernst. 2022. “COVID-19 Pandemic Led to Increase in Loneliness around the World.” American Psychological Association. May 9, 2022.
https://www.apa.org/news/press/releases/2022/05/covid-19-increase-loneliness
|
| [7] |
Clair, Ruta, Maya Gordon, Matthew Kroon, and Carolyn Reilly. 2021. “The Effects of Social Isolation on Well-Being and Life Satisfaction during Pandemic.” Humanities and Social Sciences Communications 8 (1): 1–6.
https://doi.org/10.1057/s41599-021-00710-3
|
| [8] |
BallotPedia. 2020. “States That Did Not Issue Stay-at-Home Orders in Response to the Coronavirus (COVID-19) Pandemic, 2020.” BallotPedia.
https://ballotpedia.org/States_that_did_not_issue_stay-at-home_orders_in_response_to_the_coronavirus_(COVID-19)_pandemic,_2020
|
| [9] |
Pereira-Sanchez, Victor, Frances Adiukwu, Samer El Hayek, Drita Gashi Bytyçi, Jairo M. Gonzalez-Diaz, Ganesh Kudva Kundadak, Amine Larnaout, et al. 2020. “COVID-19 Effect on Mental Health: Patients and Workforce.” The Lancet Psychiatry 7 (6): e29–30.
https://doi.org/10.1016/S2215-0366(20)30153-X
|
| [10] |
Kim, Andrew Wooyoung, Tawanda Nyengerai, and Emily Mendenhall. 2022. “Evaluating the Mental Health Impacts of the COVID-19 Pandemic: Perceived Risk of COVID-19 Infection and Childhood Trauma Predict Adult Depressive Symptoms in Urban South Africa.” Psychological Medicine 52 (8): 1587–99.
https://doi.org/10.1017/S0033291720003414
|
| [11] |
Jonathan M Metzl. 2015. “Gun Violence, Stigma, and Mental Illness: Clinical Implications.” March 25, 2015.
https://www.psychiatrictimes.com/view/gun-violence-stigma-and-mental-illness-clinical-implications
|
| [12] |
Cindy H Liu, Ga Tin Finneas Wong, Sunah Hyun, and Hyeouk Chris Hahm. 2022. “Concerns about the Social Climate, Finances, and COVID-19 Risk on Depression and Anxiety: An Analysis on U.S. Young Adults across Two Waves - PubMed.” April 2022.
https://pubmed.ncbi.nlm.nih.gov/35189512/
|
| [13] |
Shahid, Zainab, Ricci Kalayanamitra, Brendan McClafferty, Douglas Kepko, Devyani Ramgobin, Ravi Patel, Chander Shekher Aggarwal, et al. 2020. “COVID-19 and Older Adults: What We Know.” Journal of the American Geriatrics Society 68(5): 926–29.
https://doi.org/10.1111/jgs.16472
|
| [14] |
Yanez, N. David, Noel S. Weiss, Jacques-André Romand, and Miriam M. Treggiari. 2020. “COVID-19 Mortality Risk for Older Men and Women.” BMC Public Health 20(1): 1742.
https://doi.org/10.1186/s12889-020-09826-8
|
| [15] |
Caramelo, F., N. Ferreira, and B. Oliveiros. 2020. “Estimation of Risk Factors for COVID-19 Mortality - Preliminary Results.” medRxiv.
https://doi.org/10.1101/2020.02.24.20027268
|
| [16] |
Laura Hallas, Ariq Hatibie, Saptarshi Majumdar, Monika Pyarali, and Thomas Hale. 2020. “Variation in US States’ Responses to COVID-19.” University of Oxford, December.
https://www.bsg.ox.ac.uk/sites/default/files/2020-12/BSG-WP-2020-034-v2_0.pdf
|
| [17] |
Oliver, Thomas. 2006. “The Politics of Public Health Policy.” Annual Review of Public Health 27 (February): 195–233.
https://doi.org/10.1146/annurev.publhealth.25.101802.123126
|
| [18] |
Lee, Sanguk, Tai-Quan Peng, Maria Knight Lapinski, Monique Mitchell Turner, Youjin Jang, and Andrea Schaaf. 2021. “Too Stringent or Too Lenient: Antecedents and Consequences of Perceived Stringency of COVID-19 Policies in the United States.” Health Policy OPEN 2 (December): 100047.
https://doi.org/10.1016/j.hpopen.2021.100047
|
| [19] |
Kola, Lola, Brandon A. Kohrt, Bibhav Acharya, Byamah B. Mutamba, Christian Kieling, Manasi Kumar, Charlene Sunkel, Wufang Zhang, and Charlotte Hanlon. 2021. “The Path to Global Equity in Mental Health Care in the Context of COVID-19.” The Lancet 398 (10312): 1670–72.
https://doi.org/10.1016/S0140-6736(21)02233-9
|
| [20] |
Cella, David F. 1994. “Quality of Life: Concepts and Definition.” Journal of Pain and Symptom Management 9 (3): 186–92.
https://doi.org/10.1016/0885-3924(94)90129-5
|
| [21] |
Aknin, Lara B., Jan-Emmanuel De Neve, Elizabeth W. Dunn, Daisy E. Fancourt, Elkhonon Goldberg, John F. Helliwell, Sarah P. Jones, et al. 2022. “Mental Health During the First Year of the COVID-19 Pandemic: A Review and Recommendations for Moving Forward.” Perspectives on Psychological Science 17 (4): 915–36.
https://doi.org/10.1177/17456916211029964
|
| [22] |
Montesinos-Yufa, H. M., Nagasuru-McKeever, T. (2024). Gender-Specific Mental Health Outcomes in Central America: A Natural Experiment. International Journal on Data Science and Technology, 10(3), 45-50.
https://doi.org/10.11648/j.ijdst.20241003.11
|
| [23] |
Montesinos-Yufa, H. M., Musgrove, E. (2024). A Sentiment Analysis of News Articles Published Before and During the COVID-19 Pandemic. International Journal on Data Science and Technology, 10(2), 38-44.
https://doi.org/10.11648/j.ijdst.20241002.13
|
| [24] |
Fisher E., Fitzgibbon M., Glasgow R., Haire-Joshu D., Hayman L., Kaplan R., Nanney MS, Ockene JK. Behavior matters. Am J Prev Med. 2011, 40 (5), 15-30.
https://doi.org/10.1016/j.amepre.2010.12.031
|
| [25] |
Cutler W, Kolter J, Chambliss C, O'Neill H, Montesinos-Yufa HM. Long term absence of invasive breast cancer diagnosis in 2,402,672 pre and postmenopausal women: A systematic review and meta-analysis. PLoS One. 2020, Sep 10; 15 (9): e0237925.
https://doi.org/10.1371/journal.pone.0237925
PMID: 21496745; PMCID: PMC3137947.
|
| [26] |
Kircher, Sarah; Coleman, Ed; Innocent, Jhavon; Trauger, McKade; Montesinos-Yufa, Hugo (2022), “Data for "A Pandemic of Mental Health"”, Mendeley Data, V1,
https://doi.org/10.17632/vmwmn4252k.1
|
Cite This Article
-
APA Style
Coleman, E., Innocent, J., Kircher, S., Montesinos-Yufa, H. M., Trauger, M. (2024). A Pandemic of Mental Health: Evidence from the U.S.. International Journal of Data Science and Analysis, 10(4), 77-85. https://doi.org/10.11648/j.ijdsa.20241004.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Coleman, E.; Innocent, J.; Kircher, S.; Montesinos-Yufa, H. M.; Trauger, M. A Pandemic of Mental Health: Evidence from the U.S.. Int. J. Data Sci. Anal. 2024, 10(4), 77-85. doi: 10.11648/j.ijdsa.20241004.12
Copy
|
Download
-
@article{10.11648/j.ijdsa.20241004.12,
author = {Ed Coleman and Jhavon Innocent and Sarah Kircher and Hugo Moisés Montesinos-Yufa and McKade Trauger},
title = {A Pandemic of Mental Health: Evidence from the U.S.
},
journal = {International Journal of Data Science and Analysis},
volume = {10},
number = {4},
pages = {77-85},
doi = {10.11648/j.ijdsa.20241004.12},
url = {https://doi.org/10.11648/j.ijdsa.20241004.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijdsa.20241004.12},
abstract = {The direct impact of the COVID-19 pandemic and the indirect impact of the ensuing economic and political response have affected the United States on a large scale. We document a substantial surge in anxiety and depression symptoms from 2019 to 2020 driven by the young adult population, indicating a disproportional indirect impact on the young. Multivariate regression analysis was utilized to quantify the stringency of state responses’ indirect effect on the changes in anxiety or depression symptoms during the pandemic. While we observe a slight decline in the share of the adult population experiencing anxiety and depression through July 2021- June 2022, such decline does not compensate for the large surge of mental health issues among young adults in 2020. Overall, our results indicate that the effects of the stringency of the mitigation measures on different areas of health are complex and vary by state, with a wide variation of mental health-related issues by age group and a higher prevalence in younger adult age categories. After discussing inequities in the accessibility of mental health treatment, lack of health insurance, and implications for quality of life among young adults, this paper adds to the breadth of ongoing COVID-19 research and emphasizes the importance of considering the overall health of the population in a large-scale health crisis as well as discussing the potential unintended consequences of the mitigation measures put in place.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - A Pandemic of Mental Health: Evidence from the U.S.
AU - Ed Coleman
AU - Jhavon Innocent
AU - Sarah Kircher
AU - Hugo Moisés Montesinos-Yufa
AU - McKade Trauger
Y1 - 2024/09/26
PY - 2024
N1 - https://doi.org/10.11648/j.ijdsa.20241004.12
DO - 10.11648/j.ijdsa.20241004.12
T2 - International Journal of Data Science and Analysis
JF - International Journal of Data Science and Analysis
JO - International Journal of Data Science and Analysis
SP - 77
EP - 85
PB - Science Publishing Group
SN - 2575-1891
UR - https://doi.org/10.11648/j.ijdsa.20241004.12
AB - The direct impact of the COVID-19 pandemic and the indirect impact of the ensuing economic and political response have affected the United States on a large scale. We document a substantial surge in anxiety and depression symptoms from 2019 to 2020 driven by the young adult population, indicating a disproportional indirect impact on the young. Multivariate regression analysis was utilized to quantify the stringency of state responses’ indirect effect on the changes in anxiety or depression symptoms during the pandemic. While we observe a slight decline in the share of the adult population experiencing anxiety and depression through July 2021- June 2022, such decline does not compensate for the large surge of mental health issues among young adults in 2020. Overall, our results indicate that the effects of the stringency of the mitigation measures on different areas of health are complex and vary by state, with a wide variation of mental health-related issues by age group and a higher prevalence in younger adult age categories. After discussing inequities in the accessibility of mental health treatment, lack of health insurance, and implications for quality of life among young adults, this paper adds to the breadth of ongoing COVID-19 research and emphasizes the importance of considering the overall health of the population in a large-scale health crisis as well as discussing the potential unintended consequences of the mitigation measures put in place.
VL - 10
IS - 4
ER -
Copy
|
Download