Abstract
Objective: To investigate the anesthetic effect and safety of remimazolam tosilate combined with sufentanil in outpatient painless abortion. Methods: From September 2025 to October 2025, 140 patients aged 18-50 years, body mass index (BMI) 18.5-28kg / m2, American Society of Anesthesiologists (ASA) grade I-II, who underwent painless abortion in the outpatient department were selected. The patients were randomly divided into two groups: remimazolam tosilate group (group R, n = 70) and control group (group C, n = 70). Sufentanil 0.1 μg / kg was intravenously injected for analgesia pretreatment in both groups before operation. Patients in group R were intravenously injected with 0.2 mg / kg of remimazolam tosilate during anesthesia induction, and patients in group C were intravenously injected with 2 mg / kg of propofol medium and long chain fat emulsion during anesthesia induction. The main observation index was the incidence of respiratory depression. The secondary observation indexes included numerical rating scales (NRS) pain score, onset time, recovery time, Post-Anesthesia Care Unit (PACU) stay time, remedial drug use rate and incidence of adverse reactions when entering the anesthesia recovery room. Results: A total of 140 patients were included in the analysis of results. Compared with group C, the incidence of respiratory depression was lower in group R (1.4% vs 15.7%, P = 0.003), and the postoperative recovery time was shorter (P = 0.010), but the use rate of secondary rescue sedatives was higher. There was no significant difference in the onset time, duration of operation, PACU stay time, intraoperative sufentanil dosage, incidence of adverse reactions, and degree of pain in PACU between the two groups. The adverse reactions in group R were mainly manifested as body movement, and the adverse reactions in group C were mainly manifested as procedural hypotension, injection pain and respiratory depression. There was no significant difference in adverse reactions such as dizziness, intraoperative awareness, bradycardia and nausea and vomiting between the two groups. Conclusion: Remimazolam tosilate combined with sufentanil is safe and effective in outpatient painless abortion patients. Its core advantages are low risk of respiratory depression, rapid recovery, stable hemodynamics, and no common injection pain of propofol. It is highly adapted to the efficiency and safety requirements of outpatient diagnosis and treatment, and has important clinical promotion value.
Keywords
Remimazolam Tosilate, Sufentanil, Outpatient Painless Abortion, Security
1. Introduction
As a remedial measure after contraceptive failure, artificial abortion is widespread all over the world. In recent years, with the popularization of sex education and the diversification of contraceptive measures, the number of induced abortions has been controlled to a certain extent, but still remains at a relatively high level. In China, due to the large population base, the number of women who undergo abortion each year is still considerable. However, traditional abortion surgery is often accompanied by severe pain and discomfort, even fear and struggle during the operation, which may lead to uterine perforation, incomplete uterine aspiration or other complications
| [1] | Jiang H, Xu J, Richards E, Qian X, Zhang W, Hu L, Wu S, Tolhurst R; INPAC Consortium. Opportunities, challenges and systems requirements for developing post-abortion family planning services: Perceptions of service stakeholders in China. PLoS One. 2017 Oct 18; 12(10): e0186555.
https://doi.org/10.1371/journal.pone.0186555 |
[1]
. Therefore, painless artificial abortion, as an improved method of artificial abortion, has higher safety and comfort, and has been widely used in clinical practice in recent years. Outpatient painless abortion surgery has the characteristics of short operation time and high comfort requirements of patients. Anesthesia needs to achieve rapid onset, stable operation and rapid recovery
| [2] | Gu J, Liu Y, Lin X, Fu L, Liu J, Sun B, Li X, Lu B. Comparison of Remimazolam-Flumazenil and Propofol on Psychomotor Function and Emergence Following General Anesthesia in Surgical Abortion: A Randomized Controlled Trial. Drug Des Devel Ther. 2024 Dec 30; 18: 6447-6457.
https://doi.org/10.2147/DDDT.S486892 |
[2]
. In view of the shortage of operating room resources and the demand for outpatient surgery, intravenous sedative and analgesic drugs are more and more widely used in outpatient painless abortion. At present, the commonly used drugs in clinical practice are propofol, ciprofol
| [3] | Akhtar SMM, Fareed A, Ali M, Khan MS, Ali A, Mumtaz M, Kirchoff R, Asghar MS. Efficacy and safety of Ciprofol compared with Propofol during general anesthesia induction: A systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024 Jun; 94: 111425.
https://doi.org/10.1016/j.jclinane.2024.111425 |
[3]
, etomidate
| [4] | Liu J, Hu S, Zhang E, Zhang P, Guo X, Zheng Z, Fu J, Nie H. Quality of Postoperative Recovery in Older Patients Undergoing Day Surgery: A Randomized, Non-Inferiority Trial of Remimazolam versus Etomidate for Anesthesia Induction. Clin Interv Aging. 2025 Nov 14; 20: 1993-2004.
https://doi.org/10.2147/CIA.S551569 |
[4]
, sufentanil
, nalbuphine
| [6] | Chen L, Zhou Y, Cai Y, Bao N, Xu X, Shi B. The ED95 of Nalbuphine in Outpatient-Induced Abortion Compared to Equivalent Sufentanil. Basic Clin Pharmacol Toxicol. 2018 Aug; 123(2): 202-206.
https://doi.org/10.1111/bcpt.13022 Epub 2018 May 28. |
[6]
and so on. Propofol has become a commonly used anesthetic for painless abortion due to its rapid onset and short action time. However, its defects include large hemodynamic fluctuations, injection pain and obvious respiratory depression, which will seriously affect the patient 's medical experience. Therefore, it is very important to find a safe and effective anesthesia scheme to meet the needs of painless abortion.
Remimazolam tosilate is an ultra-short-acting intravenous benzodiazepine drug with sedative, hypnotic and anti-anxiety effects. It acts on the gamma-aminobutyric acid (GABA) receptor in the central nervous system, and produces dose-dependent sedation, hypnosis, anti-anxiety and anterograde amnesia by regulating neurotransmitter transmission. Remimazolam tosilate takes effect quickly, which makes the anesthesia induction process more rapid and stable. Patients can achieve the ideal depth of anesthesia in a short time, so as to facilitate surgical operation, and the drug has less inhibition on circulation and respiratory system, which is convenient for intraoperative anesthesia management. At the same time, due to the short half-life and rapid elimination, patients can quickly wake up after surgery, which can improve the turnover rate of the operating room. In addition, its anterograde amnesia effect also helps to reduce the patient 's postoperative memory burden, reduce postoperative anxiety, and improve patient satisfaction and comfort. In summary, remimazolam tosilate has the characteristics of rapid onset, rapid elimination, short half-life, and low risk of cardiovascular and respiratory depression. These characteristics make it have great application potential in painless diagnosis and treatment, day surgery anesthesia and other fields. Sufentanil is a potent opioid analgesic with strong analgesic effect and long duration. In painless abortion surgery, sufentanil is often used as an analgesic drug to reduce the patient 's pain. Combined with remimazolam tosilate, it can form a combination of sedative and analgesic drugs, so as to better meet the needs of painless abortion.
Although remimazolam tosilate and sufentanil have shown good safety and efficacy in clinical application, the efficacy of their combination in painless abortion surgery is not fully studied. The purpose of this paper is to explore the efficacy and safety of remimazolam tosilate combined with sufentanil for painless abortion in outpatient clinics, to find a safer and more effective clinical drug combination for clinical implementation of painless abortion, and to improve the comfort and safety of patients.
2. Data and Methods
2.1. General Information
This study was approved by the ethics committee of Renshou maternity and child health hospital (2025-01) and registered on the medical research registration and recording information system. All participants provided written informed consent. We recruited patients who underwent painless abortion in the outpatient department from september 2025 to october 2025, aged 18-50 years, BMI 18.5-28 kg / m2, ASA grade I-II. Exclusion criteria: (1) patients allergic to benzodiazepines or any component of the product; (2) patients with myasthenia gravis; (3) Patients with poorly controlled or untreated hypertension (resting systolic / diastolic blood pressure > 180 / 100mmHg); (4) patients with abnormal liver and kidney function; (5) patients who needed other operations during the same period of surgery, or patients who had complications that affected the evaluation of the study during and after surgery; (6) being informed of his unwillingness to participate in the researcher; (7) The expected difficult airway (patients with modified Mahalanobis grade IV); (8) Patients who had or had a history of severe mental disorders; (9) Patients with congestive heart failure, previous severe angina pectoris, unstable angina pectoris or myocardial infarction in the past six months; (10) patients with long-term alcohol and drug abuse; (11) Patients who participated in other clinical trials in the past 3 months. Exclusion criteria: serious adverse reactions occurred during or after surgery, patients or their families asked to withdraw from the study, and patients were lost to follow-up.
2.2. Random and Blind Method
A computer is used to generate a random number table in a ratio of 1: 1, using sequential labeling, opaque sealed envelopes to hide groupings. Before anesthesia, the envelope was opened by a research assistant who did not participate in the trial. According to the results of random grouping, remimazolam tosilate injection or propofol medium long chain fat emulsion injection was prepared, and the intervention drugs were delivered to the attending anesthesiologist. All patients, surgeons, and researchers in charge of data collection and follow-up are unaware of the grouping.
2.3. Grouping and Intervention
The patients were randomly divided into two groups, remimazolam tosilate group (group R) and control group (group C). Sufentanil 0.1ug / kg was injected intravenously 5 minutes before induction of anesthesia in both groups. Group R was injected intravenously with 0.2mg / kg of remimazolam tosilate, and group C was injected intravenously with 2mg / kg of propofol medium long chain fat emulsion injection. During the operation, according to the patient 's body movement, group R was injected intravenously with 0.05mg / kg of remimazolam tosilate for remedial sedation, and group C was injected intravenously with 0.5mg / kg of propofol for remedial sedation.
2.4. Anesthesia Management
In the preoperative evaluation of anesthesia, the anesthesiologist asks to collect the general information of the patient, including past history, allergic history, gestational age, etc., informs the patient of the precautions and related risks of anesthesia, and signs the anesthesia consent. According to the inclusion and exclusion criteria, the patients who met the study were strictly screened, and the patients who met the study were patiently informed of their research protocol and possible risks. After obtaining the consent of the patients and their families, informed consent was signed and included in the study. All patients were routinely fasted for 6 hours and forbidden to drink for 2 hours before surgery. After the patient entered the operating room, a venous channel was established in the left arm, and 5% glucose and sodium chloride injection was intravenously infused. Non-invasive blood pressure, heart rate, respiratory rate, and pulse oxygen saturation were routinely monitored. All patients were in the lithotomy position and maintained at a flow rate of 2 L / min. The nasal catheter is inhalated with oxygen until it wakes up, and is sent to the PACU to wake up after the operation. If moderate to severe nausea and vomiting occurred after surgery, intravenous injection of 4 mg ondansetron was given for remedy. If the remission was not good, ondansetron 4 mg was given repeatedly, and ondansetron 8 mg was given at the maximum.
2.5. Data Collection and Outcome Evaluation
The baseline data of the patients were recorded, including age, height, weight, BMI, ASA classification, gestational age, disease history, allergy history, etc. Intraoperative data included onset time, duration of surgery, recovery time, PACU stay time, intraoperative sufentanil dosage, number of rescue analgesics used, PACU pain score and incidence of adverse reactions (respiratory depression, operative hypotension, nausea and vomiting, etc.). The NRS was used to evaluate the degree of pain after operation. Among them, 0 points = no pain, 1 ~ 3 points of mild pain, 4 ~ 6 points of moderate pain, 7 ~ 10 points of severe pain
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
. Modified Observer Alertness and Sedation Assessment (MOAA / S) score was used to evaluate the depth of sedation and anesthesia
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
. The onset time is defined as the time from the beginning of administration to the disappearance of eyelash reflex
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
. The recovery time was defined as the time interval from the end of surgery to the patient 's full alertness (MOAA / S = 5)
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
. The duration of PACU stay was defined as the time interval from the patient 's full alertness (MOAA / S = 5) to leaving the PACU room
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
. Respiratory depression was defined as SPO2 20% in the absence of human intervention (i.e., without mandibular support)
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
.
The primary outcome measure was the incidence of respiratory depression. Secondary outcome measures included the NRS pain score at the time of admission to the anesthesia recovery room, the onset time, the recovery time, the PACU stay time, the use rate of remedial drugs and the incidence of adverse reactions. Adverse events were closely monitored during and after surgery and appropriate treatment was made.
2.6. Statistical Analysis
PASS 15.0 software was used to calculate the sample size. It was found that the incidence of respiratory depression in low-dose intravenous propofol was 20%-30%
| [8] | Song N, Yang Y, Zheng Z, Shi WC, Tan AP, Shan XS, Liu H, Meng L, Peng K, Ji FH. Effect of Esketamine Added to Propofol Sedation on Desaturation and Hypotension in Bidirectional Endoscopy: A Randomized Clinical Trial. JAMA Netw Open. 2023 Dec 1; 6(12): e2347886.
https://doi.org/10.1001/jamanetworkopen.2023.47886 |
| [9] | Hu B, Jiang K, Shi W, Xiao S, Zhang S, Zhang Y, Zhou Y, Tan C, Tan S, Zou X. Effect of Remimazolam Tosilate on Respiratory Depression in Elderly Patients Undergoing Gastroscopy: A Multicentered, Prospective, and Randomized Study. Drug Des Devel Ther. 2022 Dec 5; 16: 4151-4159.
https://doi.org/10.2147/DDDT.S391147 |
| [10] | Zhang C, Luo J, Liao Y, Cao H, Wu X, Huang X, Lan H, Lin Y, Chen H, Guan X. Respiratory depression in women receiving propofol/esketamine versus propofol/fentanyl for abortion surgery or curettage: a randomized clinical trial. Ann Med. 2025 Dec; 57(1): 2483981. https://doi.org/10.1080/07853890.2025.2483981 Epub 2025 Apr 2. |
[8-10]
. According to our previous pre-experiment, we expected that the incidence of respiratory depression in the control group was 25%. The remimazolam tosilate group would reduce the incidence by 60%. Set α = 0.05, 1-β = 0.8. Considering about 10% loss of follow-up and withdrawal, the two groups were planned to include 70 patients, a total of 140 subjects.
SPSS 25.0 statistical software was used to analyze the data. The histogram is used to visually evaluate the normality of the data, and the Shapiroe-Wilk test is used for verification. Quantitative data conforming to normal distribution were expressed as mean ± standard deviation, and two independent samples t test was used for comparison between groups. Non-normally distributed quantitative data were expressed as median (M) and interquartile range (IQR). Mann-Whitney U test was used for comparison between groups. Qualitative data were expressed in the form of percentage (%). Chi-square test or Fisher 's exact test was used for comparison between groups. P ≤ 0.05 was considered statistically significant.
3. Results
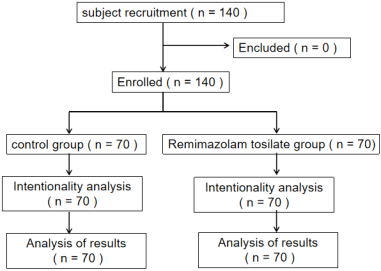
The standard flow chart of this study is shown in
Figure 1. A total of 140 patients were initially included, and no patients were lost during the study period. Finally, a total of 140 patients were included in the result analysis.
There was no significant difference in baseline data between the two groups, including age, height, weight, BMI, number of days of pregnancy, number of previous abortions, ASA classification, history of motion sickness, history of allergy and history of chronic diseases, as shown in
Table 1.
Table 1. Demographic characteristics of the participants.
Factor | Control Group (n=70) | Remimazolam tosilate Group (n=70) | P value |
Age, mean±SD, years | 31.6±5.0 | 32.2±5.4 | 0.266 |
Height, M (IQR), cm | 160(8) | 158(7) | 0.169 |
Weight, M (IQR), kg | 57(7.6) | 55(10) | 0.057 |
BMI, M (IQR), kg/m2 | 22.1(3.3) | 21.6(3.7) | 0.202 |
Pregnancy days, M (IQR), days | 44.5(9) | 43(8) | 0.065 |
Number of previous abortions, M (IQR), times | 1(2) | 1(2) | 0.702 |
ASA Classification, n (%) | | | |
Grade I | 18(25.7) | 23(32.9) | 0.353 |
Grade II | 52(74.3) | 47(67.1) |
History of nausea or motion sickness, n (%) | | | |
Yes | 29(41.4) | 21(30.0) | 0.158 |
No | 41(58.6) | 49(70.0) |
Chronic diseases, n (%) | | | |
Yes | 4(5.7) | 2(2.9) | 0.681 |
No | 66(94.3) | 68(97.1) |
Allergic history, n (%) | | | |
Yes | 4(5.7) | 5(7.1) | 0.730 |
No | 66(94.3) | 65(92.9) |
Values are expressed as mean ± standard deviation, median (interquartile range) or number (percentage). BMI = body mass index, ASA = American Society of Anesthesiologists. |
As shown in
Table 2, compared with group C, the incidence of respiratory depression in group R was lower (1.4% vs 15.7%, P = 0.003), the postoperative recovery time was shorter (P = 0.010), but the use of secondary remedial sedative drugs was higher. There was no significant difference in the onset time, duration of operation, PACU stay time, intraoperative sufentanil dosage, incidence of adverse reactions, and degree of pain in PACU between the two groups.
Table 2. Comparison of intraoperative and postoperative conditions.
Factor | Control Group (n=70) | Remimazolam tosilate group (n=70) | P value |
Onset time, M(IQR), minutes | 1(0) | 1(1) | 0.148 |
Operative duration, M(IQR), minutes | 5(2) | 5(2) | 0.832 |
Recovery time, M(IQR), minutes | 5(3) | 4(3) | 0.010 |
PACU residence time, M(IQR), minutes | 35(8) | 37(11) | 0.069 |
Sufentanil dosage during operation, M(IQR), μg | 6(1) | 5.5(1) | 0.082 |
Remedial drug use rate, n (%) | 24(34.3) | 41(58.6) | 0.004 |
Success rate of single-dose surgery, n (%) | 46(65.7) | 29(41.4) | 0.004 |
Incidence of adverse reactions, n (%) | 44(62.9) | 45(64.3) | 0.861 |
Incidence of respiratory depression, n (%) | 11(15.7) | 1(1.4) | 0.003 |
The degree of pain in PACU, n (%) | | | |
no pain | 3(4.3) | 1(1.4) | 0.682 |
mild pain | 63(90) | 63(90) |
moderate pain | 3(4.3) | 5(7.1) |
severe pain | 1(1.4) | 1(1.4) |
Values are expressed in the form of median (interquartile range) or number (percentage). |
As shown in
Table 3, the adverse reactions in group R were mainly manifested as body movement, and the adverse reactions in group C were mainly manifested as procedural hypotension, injection pain and respiratory depression. There was no significant difference in dizziness, intraoperative awareness, bradycardia, nausea and vomiting between the two groups.
Table 3. Difference of adverse reactions between two groups.
Factor | Control Group (n=70) | Remimazolam tosilate group (n=70) | P value |
body movement, n (%) | 23(32.9) | 43(61.4) | 0.001 |
Operational hypotension, n (%) | 8(11.4) | 1(1.4) | 0.033 |
injection pain, n (%) | 10(14.3) | 1(1.4) | 0.005 |
respiratory depression, n (%) | 11(15.7) | 1(1.4) | 0.003 |
Dizziness, n (%) | 0(0) | 1(1.4) | 1.000 |
intraoperative awareness, n (%) | 2(2.9) | 1(1.4) | 1.000 |
Bradycardia, n (%) | 2(2.9) | 0(0) | 0.496 |
nausea and vomiting, n (%) | 0(0) | 1(0) | 1.000 |
Values are expressed in numbers (percentages). |
4. Discussion
The results of this study showed that in the outpatient painless abortion patients, the combination of remimazolam tosilate and sufentanil was significantly superior to the propofol group in terms of respiratory safety, postoperative recovery efficiency and hemodynamic stability, but at the same time, there were more body movement reactions, resulting in a higher utilization rate of secondary remedial sedative drugs. These findings provide an important evidence-based basis for the selection of anesthesia options for short-term outpatient surgery, which is conducive to the development of better sedation and analgesia programs in clinical practice.
Respiratory depression is the most critical safety hazard of intravenous anesthesia. Especially in short operations such as outpatient abortion, airway management space is limited, and mild respiratory depression can cause the risk of hypoxemia. In this study, the incidence of respiratory depression in group R was only 1.4%, which was significantly lower than that in group C (15.7%) (P = 0.003), which was similar to the results of Zhou B et al
| [9] | Hu B, Jiang K, Shi W, Xiao S, Zhang S, Zhang Y, Zhou Y, Tan C, Tan S, Zou X. Effect of Remimazolam Tosilate on Respiratory Depression in Elderly Patients Undergoing Gastroscopy: A Multicentered, Prospective, and Randomized Study. Drug Des Devel Ther. 2022 Dec 5; 16: 4151-4159.
https://doi.org/10.2147/DDDT.S391147 |
| [11] | Zhou B, Li S, Luo A, Zheng H. The efficacy and safety of remimazolam tosilate compared with propofol for endoscopic retrograde cholangiopancreatography under monitored anesthesia care: A single-center randomized controlled clinical trial. Erratum in: Heliyon. 2025 Mar 26; 11(9): e43275.
https://doi.org/10.1016/j.heliyon.2025.e43275 |
[9, 11]
. This may be closely related to the unique pharmacological mechanism of remimazolam tosilate. From the perspective of pharmacological mechanism, remimazolam tosilate, as a new type of ultra-short-acting benzodiazepine drug, plays a role by specifically binding to GABAA (γ-aminobutyric acid type A) receptor, only increases the opening frequency of chloride channel, and does not directly inhibit the basic activity of respiratory central neurons. Its respiratory inhibition is limited, and even at higher doses, it rarely leads to severe respiratory inhibition. Propofol has no subtype selectivity for GABAA receptors, and can directly inhibit the ventilation drive of the medullary respiratory center, resulting in dose-dependent respiratory center inhibition, resulting in reduced tidal volume and slowed respiratory rate, especially when combined with sufentanil, this synergistic inhibition is more significant. This difference in mechanism is of great significance in clinical practice, especially for patients with limited respiratory function or obesity. A number of studies in recent years have supported our findings. Guo J
| [12] | Guo J, Qian Y, Zhang X, Han S, Shi Q, Xu J. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: a prospective, randomized and controlled study. BMC Anesthesiol. 2022 Jun 10; 22(1): 180.
https://doi.org/10.1186/s12871-022-01713-6 |
[12]
et al. reported similar results in a comparative study of the effects of remimazolam tosilate and propofol on gastrointestinal endoscopy in elderly patients. The incidence of respiratory depression in the remimazolam tosilate group was significantly lower than that in the propofol group (5% VS 23.7%, P = 0.026). The mechanism may be related to the metabolite HR7054 of remimazolam tosilate. HR7054 has almost no pharmacological activity and avoids delayed respiratory depression caused by the accumulation of metabolites. This provides strong pharmacological and clinical evidence for the significant difference in the incidence of respiratory depression in this study. In addition, the study of Chen J
| [13] | Chen J, Zhang J, Zhang M, Zou X, Hu B, Yang Y, Li H. Efficacy of Different Doses of Remimazolam Tosilate Combined with Esketamine in Painless Abortion Patients: A Prospective, Double-Blind, Randomized Controlled Trial. Drug Des Devel Ther. 2025 Oct 8; 19: 9117-9126. https://doi.org/10.2147/DDDT.S548701 |
[13]
and others further confirmed that during the anesthesia of remimazolam tosilate combined with esketamine, the fluctuation of blood oxygen saturation in the patients was significantly smaller than that in the propofol group, and the incidence of hypoxemia during the operation was reduced, which can not only reduce the risk of anesthesia-related complications, but also reduce the human resource investment required for respiratory intervention and improve the efficiency of outpatient surgery. In summary, the characteristic of mild respiratory depression of remimazolam tosilate is particularly important in the rapid turnover outpatient surgery environment, which helps to reduce the respiratory-related risks during postoperative recovery.
Postoperative rapid recovery is the core evaluation index of outpatient anesthesia, which directly affects the patient 's discharge time and medical experience. This study showed that the recovery time of group R was significantly shorter than that of group C (P = 0.010), which was consistent with the results of Yu X
| [14] | Yu X, Xu X, Wang J, Wang Z, Zhang Y. Effects of Remimazolam Tosilate Combined with Esketamine on Anesthetic Efficacy and Psychiatric Symptoms in Patients Undergoing Ambulatory Surgery: A Randomized Controlled Study. Drug Des Devel Ther. 2025 May 30; 19: 4527-4535.
https://doi.org/10.2147/DDDT.S519732 |
[14]
and Cheng W
| [15] | Cheng W, Cheng Y, He H, Zhou D, Wang J, Zhang Y, Wang Z. Efficacy and safety of remimazolam tosilate in anesthesia for short otolaryngology surgery. BMC Anesthesiol. 2024 Nov 11; 24(1): 407. https://doi.org/10.1186/s12871-024-02790-5 |
[15]
. This advantage may be mainly attributed to the different metabolic pathways and pharmacokinetic characteristics of the two drugs. Propofol is mainly metabolized by liver and tissue redistribution. Its elimination half-life is long (usually 30-60 minutes), and may lead to prolonged recovery time after continuous infusion due to 'atrioventricular saturation '. In contrast, the introduction of methyl propionate side chain on the basis of midazolam structure can be rapidly hydrolyzed by non-specific tissue esterase in vivo. The final half-life is about 1h, and the metabolites have no pharmacological activity. The elimination is not affected by liver and kidney function, and there is no accumulation after continuous infusion, so the recovery is more rapid and thorough. Zhang L
| [10] | Zhang C, Luo J, Liao Y, Cao H, Wu X, Huang X, Lan H, Lin Y, Chen H, Guan X. Respiratory depression in women receiving propofol/esketamine versus propofol/fentanyl for abortion surgery or curettage: a randomized clinical trial. Ann Med. 2025 Dec; 57(1): 2483981. https://doi.org/10.1080/07853890.2025.2483981 Epub 2025 Apr 2. |
[10]
et al. found that general anesthesia with remimazolam tosilate combined with flumazenil can achieve rapid recovery of consciousness during daytime surgery, but obvious re-sedation (10.8%) and drowsiness (60%) were observed in the recovery room. Different from the results of Zhang L et al., the PACU stay time of the two groups of patients in this study was similar, and no residual effects such as postoperative drowsiness and dizziness were found, which may be related to the small sample size. In addition, the awakening advantage of remimazolam tosilate is also reflected in the recovery of cognitive function, which is of great significance for outpatients to leave the hospital safely after operation. Liu B
| [16] | Liu B, Wang P, Liang L, Zhu W, Zhang H. Effect of Remimazolam vs Midazolam on Early Postoperative Cognitive Recovery in Elderly Patients Undergoing Dental Extraction: A Prospective Randomized Controlled Study. Drug Des Devel Ther. 2024 Dec 9; 18: 5895-5904.
https://doi.org/10.2147/DDDT.S491223 |
[16]
et al. in a study on the effect of remifentanil and midazolam on early postoperative cognitive function recovery in elderly patients with tooth extraction mentioned that remimazolam sedation can significantly improve the early postoperative cognitive function recovery, which is consistent with the results of Liu J
| [17] | Liu J, Li M, Zhao K, Wang H, Wu P, Yin T, He K, Yang X, Wang S. The Effects of Remimazolam Tosylate on Postoperative Memory Function in Young and Middle-Aged Patients Undergoing Laparoscopic Surgery. Drug Des Devel Ther. 2026 Mar 27; 20: 580654. https://doi.org/10.2147/DDDT.S580654 |
[17]
et al. In summary, the rapid recovery characteristics of remimazolam tosilate not only improve the turnover efficiency of the operating room, but also may improve the postoperative experience of patients.
Outpatient abortion patients are mostly young healthy people, but surgical stimulation and anesthetic drugs can cause hemodynamic fluctuations, especially hypotension may lead to insufficient uterine blood perfusion, affecting the safety of surgery. Consistent with previous research results
| [14] | Yu X, Xu X, Wang J, Wang Z, Zhang Y. Effects of Remimazolam Tosilate Combined with Esketamine on Anesthetic Efficacy and Psychiatric Symptoms in Patients Undergoing Ambulatory Surgery: A Randomized Controlled Study. Drug Des Devel Ther. 2025 May 30; 19: 4527-4535.
https://doi.org/10.2147/DDDT.S519732 |
| [18] | Hu B, Zhang M, Wu Z, Zhang X, Zou X, Tan L, Song T, Li X. Comparison of Remimazolam Tosilate and Etomidate on Hemodynamics in Cardiac Surgery: A Randomised Controlled Trial. Drug Des Devel Ther. 2023 Feb 8; 17: 381-388.
https://doi.org/10.2147/DDDT.S401969 |
[14, 18]
, this study found that patients in group R had more stable hemodynamics during surgery, which was consistent with the pharmacological characteristics of remimazolam tosilate that had less effect on the cardiovascular system. By inhibiting sympathetic activity and directly relaxing blood vessels, propofol often leads to a dose-dependent decrease in blood pressure and a decrease in heart rate, especially in patients with insufficient blood volume. Remimazolam tosilate has a slight effect on the circulatory system, which can better maintain tissue perfusion and reduce the risk of intraoperative hypotension-related complications. Tan Y
| [19] | Tan Y, Ouyang W, Tang Y, Fang N, Fang C, Quan C. Effect of remimazolam tosilate on early cognitive function in elderly patients undergoing upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2022 Mar; 37(3): 576-583.
https://doi.org/10.1111/jgh.15761 Epub 2022 Jan 3. |
[19]
et al. confirmed that in elderly patients undergoing upper gastrointestinal endoscopy, the incidence of hypotension after induction in the remimazolam tosilate group was significantly lower than that in the propofol group, and the perioperative hemodynamics was more stable. This result shows that even in people with poor hemodynamic reserve, remimazolam tosilate can still maintain stable circulatory function, and its advantages are also prominent in young patients in this study. Hemodynamic stability is particularly important for artificial abortion, because early pregnant women are often accompanied by pregnancy-related physiological changes, such as increased basal heart rate and increased blood volume, which are more sensitive to circulatory inhibition. Severe intraoperative blood flow fluctuations may lead to insufficient uterine perfusion and increase the risk of postoperative complications. The circulatory stability of remimazolam tosilate makes it particularly suitable for such patients, especially early pregnant women with anemia or relatively insufficient blood volume. In summary, the hemodynamic stability of remimazolam tosilate not only improves the safety of surgery, but also reduces postoperative discomfort caused by hemodynamic fluctuations, which meets the core requirements of ' minimally invasive and safe ' outpatient anesthesia. With the accumulation of clinical experience and the improvement of medication strategy, it is expected to become one of the important choices for anesthesia in short-term outpatient surgery.
Consistent with the results of previous studies
| [20] | Xu C, He L, Ren J, Zhou J, Guo H, Chen N, Chen H, Lv Y. Efficacy and Safety of Remimazolam Besylate Combined with Alfentanil in Painless Gastroscopy: A Randomized, Single-Blind, Parallel Controlled Study. Contrast Media Mol Imaging. 2022 Sep 22; 2022: 7102293.
https://doi.org/10.1155/2022/7102293 |
| [21] | Chen J, Zou X, Hu B, Yang Y, Wang F, Zhou Q, Shen M. Remimazolam vs Etomidate: Haemodynamic Effects in Hypertensive Elderly Patients Undergoing Non-Cardiac Surgery. Drug Des Devel Ther. 2023 Sep 27; 17: 2943-2953.
https://doi.org/10.2147/DDDT.S425590 |
[20, 21]
, this study observed that the incidence of injection pain in the remimazolam tosilate group was significantly lower than that in the propofol group, which was closely related to the physicochemical properties and preparation characteristics of the two drugs. From the perspective of drug structure, remimazolam tosilate is a derivative of benzodiazepines. After the introduction of tosylate groups in its molecular structure, the water solubility is significantly improved, and it can be made into an isotonic solution with a pH value closer to the physiological body fluid, which avoids the traditional benzodiazepines (such as midazolam). Local irritation caused by poor water solubility and the need for organic solvent solubilization. In addition, remimazolam tosilate is less toxic to vascular endothelial cells, and does not cause local osmotic pressure sudden changes or chemical inflammatory reactions after administration, reducing the stimulation signal transduction of nerve endings in the vascular wall, thereby reducing the risk of injection pain. In clinical practice, the occurrence of injection pain is directly related to the irritation of pharmaceutical preparations. The results of this study are consistent with the pharmaceutical advantages of remimazolam tosilate, and also confirm its safety advantages in minimally invasive drug delivery scenarios. It provides a basis for drug selection to reduce patients ' discomfort during drug administration in outpatient surgery.
Theoretically, as a highly selective benzodiazepine, remimazolam tosilate should have a strong anterograde amnesia effect, which may cause patients to forget about intraoperative events after surgery, thereby reducing the incidence of intraoperative awareness. However, in this study, no statistical difference was found between the two groups in the incidence of intraoperative awareness. This seemingly contradictory result may be related to the following factors. First of all, the synergistic effect of sufentanil in the anesthesia regimen may mask the difference in awareness prevention between the two groups of sedative drugs: sufentanil, as a potent opioid, can not only relieve pain, but also enhance the central inhibitory effect of sedative drugs. There is no difference in the dosage of sufentanil between the two groups. The sedative synergistic effect may make both groups of patients reach sufficient depth of consciousness inhibition, thus offsetting the potential advantages of remimazolam tosilate in preventing intraoperative awareness. Secondly, the limitation of sample size and the incidence of events may affect the statistical performance: the 2014 edition of the"Chinese Anesthesiology Quick Guide " mentioned that the incidence of intraoperative awareness reported abroad was 0.1% ~ 0.2%, and the domestic multi-center large sample survey showed that the incidence was 0.4%. It can be seen that intraoperative awareness itself is an anesthetic complication with a very low incidence. The 140 sample size included in this study is not statistically effective for testing events with such a low incidence, and further studies with a larger sample size are needed for further verification. In addition, the particularity of the type and duration of the operation may also be an important factor: the operation of painless abortion in outpatient department is simple and the duration is short. The patient enters the operation stage quickly after anesthesia induction, and the intraoperative stimulation intensity is relatively mild, and the overall awareness risk is low.
Although remimazolam tosilate has shown advantages in many aspects, this study also found that its secondary remedial sedative drug use rate is higher, and body movement reaction is more common. Liu X
| [22] | Liu X, Ding B, Shi F, Zhang Y, Liu L, Sha Y, Zhao T. The Efficacy and Safety of Remimazolam Tosilate versus Etomidate-Propofol in Elderly Outpatients Undergoing Colonoscopy: A Prospective, Randomized, Single-Blind, Non-Inferiority Trial. Drug Des Devel Ther. 2021 Nov 16; 15: 4675-4685.
https://doi.org/10.2147/DDDT.S339535 |
[22]
et al. also reported that the remimazolam tosilate group had a higher incidence of body movement. This phenomenon may need to be analyzed from three aspects: drug sedation intensity, dose selection and surgical stimulation matching. From the perspective of sedative intensity, as a benzodiazepine, the main role of remimazolam tosilate is anti-anxiety and amnesia, and its analgesic effect is limited. Under strong noxious stimulation (such as cervical dilatation and uterine cavity suction), the simple sedative effect may not be sufficient to completely inhibit the body movement response. From the perspective of dose selection and surgical stimulation matching, the anesthesia induction of group R in this study was induced by intravenous injection of 0.2 mg / kg of remimazolam tosilate, with a lower dose. The sedative intensity of remimazolam tosilate is lower than that of propofol. The sequential test of 2022 in the Journal of Medical Science Monitoring
| [23] | Cao Y, Chi P, Zhou C, Lv W, Quan Z, Xue FS. Remimazolam Tosilate Sedation with Adjuvant Sufentanil in Chinese Patients with Liver Cirrhosis Undergoing Gastroscopy: A Randomized Controlled Study. Med Sci Monit. 2022 Jun 16; 28: e936580. https://doi.org/10.12659/MSM.936580 |
[23]
showed that the ED50 and ED95 for endoscopic deep sedation were 0.174 mg / kg and 0.219 mg / kg, respectively. However, the induction dose in this study did not reach the effective sedation threshold of the individual, and it was difficult to completely inhibit the strong stimulation such as cervical dilatation and negative pressure suction during abortion. In addition, the analgesic dose fixation of sufentanil may also be an important factor. There are individual differences in pain stimulation during abortion surgery. When the depth of sedation is insufficient, a single dose of sufentanil is difficult to fully cover the pain, which in turn triggers body movement. The study of different doses of remimazolam tosilate
| [19] | Tan Y, Ouyang W, Tang Y, Fang N, Fang C, Quan C. Effect of remimazolam tosilate on early cognitive function in elderly patients undergoing upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2022 Mar; 37(3): 576-583.
https://doi.org/10.1111/jgh.15761 Epub 2022 Jan 3. |
[19]
provides a solution: the researchers compared the application of 0.1 mg / kg (R1 group) and 0.2 mg / kg (R2 group) of remimazolam tosilate in painless gastrointestinal endoscopy, and found that the sedation time and recovery time of R2 group were significantly longer than those of R1 group. This indicates that the sedative effect of remimazolam tosilate will increase with the increase of dose. By optimizing the dosing regimen, the body movement problem may be improved without sacrificing the recovery speed. Another strategy is to adjust the dose or timing of opioids. Studies have shown
| [24] | Guo Y, Yao Z, Feng Y, Wang D, Wang Y, Lin J. ED50 and ED95 of Remimazolam Tosilate Combined with Different Doses of Fentanyl in Elderly Patients for Painless Gastroscopy. Drug Des Devel Ther. 2024 Jun 18; 18: 2347-2356.
https://doi.org/10.2147/DDDT.S462607 |
[24]
that remimazolam tosilate has a synergistic effect with fentanyl in a dose-dependent manner. Appropriately increasing the dose of fentanyl or optimizing the timing of administration may enhance the analgesic effect and reduce the occurrence of body movement. In addition, considering that body movement often occurs in the most stimulating steps of surgery (such as cervical dilatation and uterine aspiration), some scholars suggest prophylactic addition of drugs or target-controlled infusion to maintain a stable blood concentration before these critical steps
| [7] | Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860 |
[7]
. These strategies need to be continuously adjusted according to the individual response of patients in clinical practice to achieve the best balance between sedation and recovery speed. In summary, although there may be many challenges in the clinical application of remimazolam tosilate, it can be improved by optimizing the scheme. With the accumulation of clinical experience and the improvement of medication strategy, remimazolam tosilate is expected to become one of the important choices for anesthesia in short-term outpatient surgery.
There are some limitations in this study. First of all, this is a single-center, small-sample study, and more high-quality large-scale prospective studies are needed to verify the results of this study. Secondly, this study only studied the combined effect of fixed dose of remimazolam tosilate and sufentanil, and did not explore other doses. Further studies are still needed to explore the optimal dose regimen of remimazolam tosilate for painless abortion, including initial dose, additional dose and dose adjustment of different populations. Third, the effect of different doses of remimazolam tosilate on body movement was not discussed.
5. Conclusions
In conclusion, remimazolam tosilate combined with sufentanil is safe and effective for outpatient painless abortion. Its core advantages are low risk of respiratory depression, rapid recovery, stable hemodynamics, and no common injection pain of propofol. It is highly suitable for the efficiency and safety requirements of outpatient diagnosis and treatment, especially for patients who are intolerant to propofol (such as injection pain sensitivity, poor respiratory function reserve, and allergy to soy products). Its characteristics of ' safety priority and rapid recovery ' are in line with the development trend of modern outpatient anesthesia and have important clinical promotion value.
Abbreviations
BMI | Body Mass Index |
ASA | American Society of Anesthesiologists |
NRS | Numerical Rating Scales |
PACU | Post-Anesthesia Care Unit |
GABA | Gamma-Aminobutyric Acid |
R | Remimazolam Tosilate |
C | Control |
MOAA / S | Modified Observer Alertness and Sedation Assessment |
M | Median |
IQR | Interquartile Range |
Author Contributions
Zeng Xu: Conceptualization, Formal Analysis, Investigation, Methodology, Software
Peng Jian: Data curation, Funding acquisition, Project administration, Resources
Funding
This work is supported by Name of Sichuan Medical Science and Technology Innovation Research Association(Grant No. 2025YCZD014).
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Jiang H, Xu J, Richards E, Qian X, Zhang W, Hu L, Wu S, Tolhurst R; INPAC Consortium. Opportunities, challenges and systems requirements for developing post-abortion family planning services: Perceptions of service stakeholders in China. PLoS One. 2017 Oct 18; 12(10): e0186555.
https://doi.org/10.1371/journal.pone.0186555
|
| [2] |
Gu J, Liu Y, Lin X, Fu L, Liu J, Sun B, Li X, Lu B. Comparison of Remimazolam-Flumazenil and Propofol on Psychomotor Function and Emergence Following General Anesthesia in Surgical Abortion: A Randomized Controlled Trial. Drug Des Devel Ther. 2024 Dec 30; 18: 6447-6457.
https://doi.org/10.2147/DDDT.S486892
|
| [3] |
Akhtar SMM, Fareed A, Ali M, Khan MS, Ali A, Mumtaz M, Kirchoff R, Asghar MS. Efficacy and safety of Ciprofol compared with Propofol during general anesthesia induction: A systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024 Jun; 94: 111425.
https://doi.org/10.1016/j.jclinane.2024.111425
|
| [4] |
Liu J, Hu S, Zhang E, Zhang P, Guo X, Zheng Z, Fu J, Nie H. Quality of Postoperative Recovery in Older Patients Undergoing Day Surgery: A Randomized, Non-Inferiority Trial of Remimazolam versus Etomidate for Anesthesia Induction. Clin Interv Aging. 2025 Nov 14; 20: 1993-2004.
https://doi.org/10.2147/CIA.S551569
|
| [5] |
Zuurmond WW, van Leeuwen L. Recovery from sufentanil anaesthesia for outpatient arthroscopy: a comparison with isoflurane. Acta Anaesthesiol Scand. 1987 Feb; 31(2): 154-6.
https://doi.org/10.1111/j.1399-6576.1987.tb02539.x
|
| [6] |
Chen L, Zhou Y, Cai Y, Bao N, Xu X, Shi B. The ED95 of Nalbuphine in Outpatient-Induced Abortion Compared to Equivalent Sufentanil. Basic Clin Pharmacol Toxicol. 2018 Aug; 123(2): 202-206.
https://doi.org/10.1111/bcpt.13022
Epub 2018 May 28.
|
| [7] |
Li W, Zhao J, Hao R, Wang S, Chen M, Liu H, Qi L, Hao Z. The Efficacy and Safety of Remimazolam Besylate Combined with Esketamine for Outpatient Colonoscopy: A Prospective, Randomized, Controlled Clinical Trial. Drug Des Devel Ther. 2023 Sep 18; 17: 2875-2887.
https://doi.org/10.2147/DDDT.S425860
|
| [8] |
Song N, Yang Y, Zheng Z, Shi WC, Tan AP, Shan XS, Liu H, Meng L, Peng K, Ji FH. Effect of Esketamine Added to Propofol Sedation on Desaturation and Hypotension in Bidirectional Endoscopy: A Randomized Clinical Trial. JAMA Netw Open. 2023 Dec 1; 6(12): e2347886.
https://doi.org/10.1001/jamanetworkopen.2023.47886
|
| [9] |
Hu B, Jiang K, Shi W, Xiao S, Zhang S, Zhang Y, Zhou Y, Tan C, Tan S, Zou X. Effect of Remimazolam Tosilate on Respiratory Depression in Elderly Patients Undergoing Gastroscopy: A Multicentered, Prospective, and Randomized Study. Drug Des Devel Ther. 2022 Dec 5; 16: 4151-4159.
https://doi.org/10.2147/DDDT.S391147
|
| [10] |
Zhang C, Luo J, Liao Y, Cao H, Wu X, Huang X, Lan H, Lin Y, Chen H, Guan X. Respiratory depression in women receiving propofol/esketamine versus propofol/fentanyl for abortion surgery or curettage: a randomized clinical trial. Ann Med. 2025 Dec; 57(1): 2483981.
https://doi.org/10.1080/07853890.2025.2483981
Epub 2025 Apr 2.
|
| [11] |
Zhou B, Li S, Luo A, Zheng H. The efficacy and safety of remimazolam tosilate compared with propofol for endoscopic retrograde cholangiopancreatography under monitored anesthesia care: A single-center randomized controlled clinical trial. Erratum in: Heliyon. 2025 Mar 26; 11(9): e43275.
https://doi.org/10.1016/j.heliyon.2025.e43275
|
| [12] |
Guo J, Qian Y, Zhang X, Han S, Shi Q, Xu J. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: a prospective, randomized and controlled study. BMC Anesthesiol. 2022 Jun 10; 22(1): 180.
https://doi.org/10.1186/s12871-022-01713-6
|
| [13] |
Chen J, Zhang J, Zhang M, Zou X, Hu B, Yang Y, Li H. Efficacy of Different Doses of Remimazolam Tosilate Combined with Esketamine in Painless Abortion Patients: A Prospective, Double-Blind, Randomized Controlled Trial. Drug Des Devel Ther. 2025 Oct 8; 19: 9117-9126.
https://doi.org/10.2147/DDDT.S548701
|
| [14] |
Yu X, Xu X, Wang J, Wang Z, Zhang Y. Effects of Remimazolam Tosilate Combined with Esketamine on Anesthetic Efficacy and Psychiatric Symptoms in Patients Undergoing Ambulatory Surgery: A Randomized Controlled Study. Drug Des Devel Ther. 2025 May 30; 19: 4527-4535.
https://doi.org/10.2147/DDDT.S519732
|
| [15] |
Cheng W, Cheng Y, He H, Zhou D, Wang J, Zhang Y, Wang Z. Efficacy and safety of remimazolam tosilate in anesthesia for short otolaryngology surgery. BMC Anesthesiol. 2024 Nov 11; 24(1): 407.
https://doi.org/10.1186/s12871-024-02790-5
|
| [16] |
Liu B, Wang P, Liang L, Zhu W, Zhang H. Effect of Remimazolam vs Midazolam on Early Postoperative Cognitive Recovery in Elderly Patients Undergoing Dental Extraction: A Prospective Randomized Controlled Study. Drug Des Devel Ther. 2024 Dec 9; 18: 5895-5904.
https://doi.org/10.2147/DDDT.S491223
|
| [17] |
Liu J, Li M, Zhao K, Wang H, Wu P, Yin T, He K, Yang X, Wang S. The Effects of Remimazolam Tosylate on Postoperative Memory Function in Young and Middle-Aged Patients Undergoing Laparoscopic Surgery. Drug Des Devel Ther. 2026 Mar 27; 20: 580654.
https://doi.org/10.2147/DDDT.S580654
|
| [18] |
Hu B, Zhang M, Wu Z, Zhang X, Zou X, Tan L, Song T, Li X. Comparison of Remimazolam Tosilate and Etomidate on Hemodynamics in Cardiac Surgery: A Randomised Controlled Trial. Drug Des Devel Ther. 2023 Feb 8; 17: 381-388.
https://doi.org/10.2147/DDDT.S401969
|
| [19] |
Tan Y, Ouyang W, Tang Y, Fang N, Fang C, Quan C. Effect of remimazolam tosilate on early cognitive function in elderly patients undergoing upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2022 Mar; 37(3): 576-583.
https://doi.org/10.1111/jgh.15761
Epub 2022 Jan 3.
|
| [20] |
Xu C, He L, Ren J, Zhou J, Guo H, Chen N, Chen H, Lv Y. Efficacy and Safety of Remimazolam Besylate Combined with Alfentanil in Painless Gastroscopy: A Randomized, Single-Blind, Parallel Controlled Study. Contrast Media Mol Imaging. 2022 Sep 22; 2022: 7102293.
https://doi.org/10.1155/2022/7102293
|
| [21] |
Chen J, Zou X, Hu B, Yang Y, Wang F, Zhou Q, Shen M. Remimazolam vs Etomidate: Haemodynamic Effects in Hypertensive Elderly Patients Undergoing Non-Cardiac Surgery. Drug Des Devel Ther. 2023 Sep 27; 17: 2943-2953.
https://doi.org/10.2147/DDDT.S425590
|
| [22] |
Liu X, Ding B, Shi F, Zhang Y, Liu L, Sha Y, Zhao T. The Efficacy and Safety of Remimazolam Tosilate versus Etomidate-Propofol in Elderly Outpatients Undergoing Colonoscopy: A Prospective, Randomized, Single-Blind, Non-Inferiority Trial. Drug Des Devel Ther. 2021 Nov 16; 15: 4675-4685.
https://doi.org/10.2147/DDDT.S339535
|
| [23] |
Cao Y, Chi P, Zhou C, Lv W, Quan Z, Xue FS. Remimazolam Tosilate Sedation with Adjuvant Sufentanil in Chinese Patients with Liver Cirrhosis Undergoing Gastroscopy: A Randomized Controlled Study. Med Sci Monit. 2022 Jun 16; 28: e936580.
https://doi.org/10.12659/MSM.936580
|
| [24] |
Guo Y, Yao Z, Feng Y, Wang D, Wang Y, Lin J. ED50 and ED95 of Remimazolam Tosilate Combined with Different Doses of Fentanyl in Elderly Patients for Painless Gastroscopy. Drug Des Devel Ther. 2024 Jun 18; 18: 2347-2356.
https://doi.org/10.2147/DDDT.S462607
|
Cite This Article
-
APA Style
Xu, Z., Jian, P. (2026). Efficacy and Safety of Remimazolam Tosilate Combined with Sufentanil for Outpatient Painless Abortion:
A Randomized, Double-blind, Prospective Trial. Journal of Drug Design and Medicinal Chemistry, 12(1), 19-28. https://doi.org/10.11648/j.jddmc.20261201.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Xu, Z.; Jian, P. Efficacy and Safety of Remimazolam Tosilate Combined with Sufentanil for Outpatient Painless Abortion:
A Randomized, Double-blind, Prospective Trial. J. Drug Des. Med. Chem. 2026, 12(1), 19-28. doi: 10.11648/j.jddmc.20261201.12
Copy
|
Download
AMA Style
Xu Z, Jian P. Efficacy and Safety of Remimazolam Tosilate Combined with Sufentanil for Outpatient Painless Abortion:
A Randomized, Double-blind, Prospective Trial. J Drug Des Med Chem. 2026;12(1):19-28. doi: 10.11648/j.jddmc.20261201.12
Copy
|
Download
-
@article{10.11648/j.jddmc.20261201.12,
author = {Zeng Xu and Peng Jian},
title = {Efficacy and Safety of Remimazolam Tosilate Combined with Sufentanil for Outpatient Painless Abortion:
A Randomized, Double-blind, Prospective Trial},
journal = {Journal of Drug Design and Medicinal Chemistry},
volume = {12},
number = {1},
pages = {19-28},
doi = {10.11648/j.jddmc.20261201.12},
url = {https://doi.org/10.11648/j.jddmc.20261201.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jddmc.20261201.12},
abstract = {Objective: To investigate the anesthetic effect and safety of remimazolam tosilate combined with sufentanil in outpatient painless abortion. Methods: From September 2025 to October 2025, 140 patients aged 18-50 years, body mass index (BMI) 18.5-28kg / m2, American Society of Anesthesiologists (ASA) grade I-II, who underwent painless abortion in the outpatient department were selected. The patients were randomly divided into two groups: remimazolam tosilate group (group R, n = 70) and control group (group C, n = 70). Sufentanil 0.1 μg / kg was intravenously injected for analgesia pretreatment in both groups before operation. Patients in group R were intravenously injected with 0.2 mg / kg of remimazolam tosilate during anesthesia induction, and patients in group C were intravenously injected with 2 mg / kg of propofol medium and long chain fat emulsion during anesthesia induction. The main observation index was the incidence of respiratory depression. The secondary observation indexes included numerical rating scales (NRS) pain score, onset time, recovery time, Post-Anesthesia Care Unit (PACU) stay time, remedial drug use rate and incidence of adverse reactions when entering the anesthesia recovery room. Results: A total of 140 patients were included in the analysis of results. Compared with group C, the incidence of respiratory depression was lower in group R (1.4% vs 15.7%, P = 0.003), and the postoperative recovery time was shorter (P = 0.010), but the use rate of secondary rescue sedatives was higher. There was no significant difference in the onset time, duration of operation, PACU stay time, intraoperative sufentanil dosage, incidence of adverse reactions, and degree of pain in PACU between the two groups. The adverse reactions in group R were mainly manifested as body movement, and the adverse reactions in group C were mainly manifested as procedural hypotension, injection pain and respiratory depression. There was no significant difference in adverse reactions such as dizziness, intraoperative awareness, bradycardia and nausea and vomiting between the two groups. Conclusion: Remimazolam tosilate combined with sufentanil is safe and effective in outpatient painless abortion patients. Its core advantages are low risk of respiratory depression, rapid recovery, stable hemodynamics, and no common injection pain of propofol. It is highly adapted to the efficiency and safety requirements of outpatient diagnosis and treatment, and has important clinical promotion value.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Efficacy and Safety of Remimazolam Tosilate Combined with Sufentanil for Outpatient Painless Abortion:
A Randomized, Double-blind, Prospective Trial
AU - Zeng Xu
AU - Peng Jian
Y1 - 2026/04/23
PY - 2026
N1 - https://doi.org/10.11648/j.jddmc.20261201.12
DO - 10.11648/j.jddmc.20261201.12
T2 - Journal of Drug Design and Medicinal Chemistry
JF - Journal of Drug Design and Medicinal Chemistry
JO - Journal of Drug Design and Medicinal Chemistry
SP - 19
EP - 28
PB - Science Publishing Group
SN - 2472-3576
UR - https://doi.org/10.11648/j.jddmc.20261201.12
AB - Objective: To investigate the anesthetic effect and safety of remimazolam tosilate combined with sufentanil in outpatient painless abortion. Methods: From September 2025 to October 2025, 140 patients aged 18-50 years, body mass index (BMI) 18.5-28kg / m2, American Society of Anesthesiologists (ASA) grade I-II, who underwent painless abortion in the outpatient department were selected. The patients were randomly divided into two groups: remimazolam tosilate group (group R, n = 70) and control group (group C, n = 70). Sufentanil 0.1 μg / kg was intravenously injected for analgesia pretreatment in both groups before operation. Patients in group R were intravenously injected with 0.2 mg / kg of remimazolam tosilate during anesthesia induction, and patients in group C were intravenously injected with 2 mg / kg of propofol medium and long chain fat emulsion during anesthesia induction. The main observation index was the incidence of respiratory depression. The secondary observation indexes included numerical rating scales (NRS) pain score, onset time, recovery time, Post-Anesthesia Care Unit (PACU) stay time, remedial drug use rate and incidence of adverse reactions when entering the anesthesia recovery room. Results: A total of 140 patients were included in the analysis of results. Compared with group C, the incidence of respiratory depression was lower in group R (1.4% vs 15.7%, P = 0.003), and the postoperative recovery time was shorter (P = 0.010), but the use rate of secondary rescue sedatives was higher. There was no significant difference in the onset time, duration of operation, PACU stay time, intraoperative sufentanil dosage, incidence of adverse reactions, and degree of pain in PACU between the two groups. The adverse reactions in group R were mainly manifested as body movement, and the adverse reactions in group C were mainly manifested as procedural hypotension, injection pain and respiratory depression. There was no significant difference in adverse reactions such as dizziness, intraoperative awareness, bradycardia and nausea and vomiting between the two groups. Conclusion: Remimazolam tosilate combined with sufentanil is safe and effective in outpatient painless abortion patients. Its core advantages are low risk of respiratory depression, rapid recovery, stable hemodynamics, and no common injection pain of propofol. It is highly adapted to the efficiency and safety requirements of outpatient diagnosis and treatment, and has important clinical promotion value.
VL - 12
IS - 1
ER -
Copy
|
Download