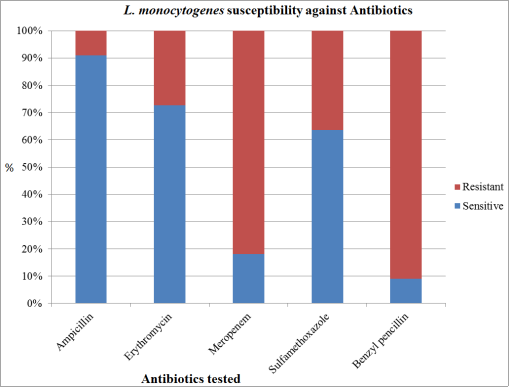
Background: Listeria monocytogenes is a facultative intracellular pathogen that causes serious invasive infections in pregnant women, resulting in disseminated fetal infections, abortions, and still-births. Although it causes a greater burden on pregnant women and their infants, the case in Ethiopia is overlooked, and there is a scarcity of data on L. monocytogenes, particularly in the southern parts of Ethiopia. Therefore, this study aimed to determine the prevalence and, antibiotics susceptibility of L. monocytogenes and its associated risk factors among pregnant women attending the Millennium Health Center, Hawassa, Ethiopia. Method: A cross-sectional study was conducted on 203 pregnant women between May 30 and July 30, 2022. Socio-demographic data and 5 ml venous blood samples were collected from pregnant women using structured questionnaire. Data were analyzed using SPSS version 25. Bivariate logistic regression was carried out then variables with p<0.25 were further analyzed by multivariate logistic regressions, p-values <0.05 were accepted as statistically significant. Results: The overall prevalence of L. monocytogenes among pregnant women was found to be 11/203 (5.42%; 95% CI=2.88-9.38). L. monocytogenes was resistant to benzyl penicillin (90.91%) and meropenem (81.82%), but susceptible to ampicillin (90.91%). Raw meat (AOR=6.99; 95% CI=1.39-35.14), p=0.018), uncooked vegetables (AOR=6.62; 95% CI=1.04-42.30), p=0.046), unpasteurized milk (AOR=7.56; 95% CI=1.33-42.97), p=0.023) and fever (AOR=14.65; 95% CI=3.15-68.15), p=0.001) were significantly associated with L. monocytogenes infection. Conclusion: L. monocytogenes was resistant to benzyl penicillin, meropenem, erythromycin, and sulfamethoxazole but susceptible to ampicillin. Raw meat, uncooked vegetables, unpasteurized milk, and fever were significantly associated with L. monocytogenes.
| Published in | Journal of Gynecology and Obstetrics (Volume 12, Issue 2) |
| DOI | 10.11648/j.jgo.20241202.12 |
| Page(s) | 20-30 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Antibiotics Susceptibility, Listeria monocytogenes, Pregnant Women, Prevalence, Hawassa, Ethiopia
2.1. Study Setting
2.2. Eligibility Criteria
2.3. Sample size Determination and Sampling Technique
2.3.1. Dependent Variable
2.3.2. Independent Variables
2.3.3. Co-variables
2.4. Data and Specimen Collection
2.5. Culture and Identification
2.6. Antibiotics Susceptibility Testing
2.7. Quality Assurance
2.8. Data Entry and Analysis
3.1. Socio-Demographic Characteristics
Variables | Category | Frequency | Percent (%) |
|---|---|---|---|
Age (years) | 18 – 24 | 91 | 44.8 |
25 – 34 | 72 | 35.5 | |
35 – 44 | 40 | 19.7 | |
Residence | Urban | 164 | 80.8 |
Rural | 39 | 19.2 | |
Marital Status | Single | 20 | 9.9 |
Married | 160 | 78.8 | |
Divorced | 14 | 6.9 | |
Widowed | 9 | 4.4 | |
Educational status | Read and Write | 20 | 9.9 |
Elementary School (1 – 8) | 54 | 26.6 | |
Secondary School (9 – 12) | 68 | 33.5 | |
College/University | 61 | 30 | |
Occupation | Government employee | 54 | 26.6 |
Merchant | 38 | 18.7 | |
Daily Worker | 40 | 19.7 | |
House Wife | 71 | 35 |
3.2. Gestational Age and Frequent Food Habits
Variables | Category | Frequency | Percent (%) |
|---|---|---|---|
Gestational age | 1st trimester | 41 | 20.2 |
2nd trimester | 85 | 41.9 | |
3rd trimester | 77 | 37.9 | |
Frequent eating/drinking habits | |||
Uncooked meat | Yes | 75 | 36.9 |
No | 128 | 63.1 | |
Uncooked/raw fish | Yes | 105 | 51.7 |
No | 98 | 48.3 | |
Uncooked vegetables | Yes | 95 | 46.8 |
No | 108 | 53.2 | |
Unpasteurized milk | Yes | 78 | 38.4 |
No | 125 | 61.6 | |
3.3. Clinical Characteristics of L. monocytogenes Infection
Variables | Category | Frequency | Percent (%) |
|---|---|---|---|
Fever | Yes | 24 | 11.8 |
No | 179 | 88.2 | |
Headache | Yes | 42 | 20.7 |
No | 161 | 79.3 | |
Gastroenteritis | Yes | 58 | 28.6 |
No | 145 | 71.4 | |
Nausea/Vomiting | Yes | 49 | 24.1 |
No | 154 | 75.9 | |
Backache | Yes | 35 | 17.2 |
No | 168 | 82.8 | |
Muscle pains | Yes | 33 | 16.3 |
No | 170 | 83.7 |
3.4. Prevalence of L. monocytogenes
Variables | Category | L. monocytogenes | p-value | COR (95% CI) | |
|---|---|---|---|---|---|
Positive (n=11) (%) | Negative (n=192) (%) | ||||
Age (years) | 18 – 24 | 2 (2.20) | 89 (97.80) | Ref | |
25 – 34 | 8 (11.11) | 64 (88.89) | 0.034* | 5.56 (1.14-27.07) | |
35 – 44 | 1 (2.50) | 39 (97.50) | 0.915 | 1.14 (0.10-12.96) | |
Residence | Urban | 8 (4.88) | 156 (95.12) | Ref | |
Rural | 3 (7.69) | 36 (92.31) | 0.489 | 1.63 (0.41-6.43) | |
Marital status | Single | 2 (10.00) | 18 (90.00) | Ref | |
Married | 7 (4.38) | 153 (95.62) | 0.291 | 0.41 (0.08-2.14) | |
Divorced | 1 (7.14) | 13 (92.86) | 0.773 | 0.69 (0.06-8.47) | |
Widowed | 1 (11.11) | 8 (88.89) | 0.928 | 1.13 (0.09-14.28) | |
Educational status | Read and Write | 2 (10.00) | 18 (90.00) | 0.252 | 3.28 (0.43-24.95) |
Elementary School | 3 (5.56) | 51 (94.44) | 0.555 | 1.74 (0.28-10.80) | |
Secondary School | 4 (5.88) | 64 (94.12) | 0.489 | 1.84 (0.33-10.44) | |
College/University | 2 (3.28) | 59 (96.72) | Ref | ||
Occupation | Government employee | 2 (3.70) | 52 (96.30) | Ref | |
Merchant | 2 (5.26) | 36 (94.74) | 0.719 | 1.44 (0.19-10.73) | |
Daily Worker | 4 (10.00) | 36 (90.00) | 0.235* | 2.89 (0.50-16.62) | |
House Wife | 3 (4.23) | 68 (95.77) | 0.883 | 1.15 (0.19-7.12) | |
3.5. Association of Possible Risk Factors for L. monocytogenes Infection
Variables | Category | L. monocytogenes | p-value | COR (95% CI) | |
|---|---|---|---|---|---|
Positive (n=11) (%) | Negative (n=192) (%) | ||||
Gestational age | 1st trimester | 1 (2.44) | 40 (97.56) | Ref | |
2nd trimester | 4 (4.71) | 81 (95.29) | 0.549 | 1.98 (0.21-18.26) | |
3rd trimester | 6 (7.79) | 71 (92.21) | 0.267 | 3.38 (0.39-29.08) | |
Frequently feeding habit | |||||
Uncooked meat | Yes | 8 (10.67) | 67 (89.33) | 0.021* | 4.98 (1.28-19.38) |
No | 3 (2.34) | 125 (97.66) | Ref | ||
Uncooked/raw fish | Yes | 7 (6.67) | 98 (93.33) | 0.421 | 1.68 (0.48-5.92) |
No | 4 (4.08) | 94 (95.92) | Ref | ||
Uncooked vegetables | Yes | 9 (9.47) | 86 (90.53) | 0.031* | 5.55 (1.17-26.35) |
No | 2 (1.85) | 106 (98.15) | Ref | ||
Unpasteurized milk | Yes | 9 (11.54) | 69 (88.46) | 0.009* | 8.02 (1.69-38.19) |
No | 2 (1.60) | 123 (98.40) | Ref | ||
3.6. Clinical Signs and Symptoms
Variables | Category | L. monocytogenes | p-value | COR (95% CI) | |
|---|---|---|---|---|---|
Positive (n=11) (%) | Negative (n=192) (%) | ||||
Fever | Yes | 7 (29.17) | 17 (70.83) | 0.001* | 18.02 (4.79-67.81) |
No | 4 (2.23) | 175 (97.77) | Ref | ||
Headache | Yes | 3 (7.14) | 39 (92.86) | 0.581 | 1.47 (0.38-5.81) |
No | 8 (4.97) | 153 (95.03) | Ref | ||
Gastroenteritis | Yes | 4 (6.90) | 54 (93.10) | 0.558 | 1.46 (0.41-5.19) |
No | 7 (4.83) | 138 (95.17) | Ref | ||
Nausea/Vomiting | Yes | 7 (14.29) | 42 (85.71) | 0.005* | 6.25 (1.75-22.37) |
No | 4 (2.60) | 150 (97.40) | Ref | ||
Backache | Yes | 3 (8.57) | 32 (91.43) | 0.372 | 1.88 (0.47-7.45) |
No | 8 (4.76) | 160 (95.24) | Ref | ||
Muscle pains | Yes | 3 (9.09) | 30 (90.91) | 0.317 | 2.03 (0.51-8.07) |
No | 8 (4.71) | 162 (95.29) | Ref | ||
Variables | Category | L. monocytogenes | p-value | COR (95% CI) | p-value | AOR (95% CI) | |
|---|---|---|---|---|---|---|---|
Positive (n=11) (%) | Negative (n=192) (%) | ||||||
Age (years) | 18 – 24 | 2 (2.20) | 89 (97.80) | Ref | Ref | ||
25 – 34 | 8 (11.11) | 64 (88.89) | 0.034* | 5.56 (1.14-27.07) | 0.141 | 4.40 (0.61-31.74) | |
35 – 44 | 1 (2.50) | 39 (97.50) | 0.915 | 1.14 (0.10-12.96) | 0.783 | 1.51 (0.80-28.53) | |
Uncooked meat | Yes | 8 (10.67) | 67 (89.33) | 0.021* | 4.98 (1.28-19.38) | 0.018** | 6.99 (1.39-35.14) |
No | 3 (2.34) | 125 (97.66) | Ref | Ref | |||
Uncooked vegetables | Yes | 9 (9.47) | 86 (90.53) | 0.031* | 5.55 (1.17-26.35) | 0.046** | 6.62 (1.04-42.30) |
No | 2 (1.85) | 106 (98.15) | Ref | Ref | |||
Unpasteurized milk | Yes | 9 (11.54) | 69 (88.46) | 0.009* | 8.02 (1.69-38.19) | 0.023** | 7.56 (1.33-42.97) |
No | 2 (1.60) | 123 (98.40) | Ref | Ref | |||
Fever | Yes | 7 (29.17) | 17 (70.83) | 0.001* | 18.02 (4.79-67.81) | 0.001** | 14.65 (3.15-68.15) |
No | 4 (2.23) | 175 (97.77) | Ref | Ref | |||
Nausea/Vomiting | Yes | 7 (14.29) | 42 (85.71) | 0.005* | 6.25 (1.75-22.37) | 0.716 | 1.47 (0.18-11.96) |
No | 4 (2.60) | 150 (97.40) | Ref | Ref | |||
3.7. Antibiotics Susceptibility of L. monocytogenes
3.8. Antibiogram of Listeria monocytogenes
Resistance pattern | Resistant strain, n (%) |
|---|---|
BP | 1 (10) |
BP, Mem | 5 (50) |
BP, Mem, SXT | 1 (10) |
BP, Ery, Mem, SXT | 2 (20) |
Amp, BP, Ery, Mem, SXT | 1 (10) |
Total | 10 (100) |
Ethics Approval and Consent to Participate
Consent for Publication
| [1] | Bucur, F. I., et al., Resistance of Listeria monocytogenes to stress conditions encountered in food and food processing environments. Frontiers in microbiology, 2018. 9: p. 2700. |
| [2] | Letchumanan, V., et al., A review on the characteristics, taxanomy and prevalence of Listeria monocytogenes. Progress In Microbes & Molecular Biology, 2018. 1(1). |
| [3] | Radoshevich, L. and P. Cossart, Listeria monocytogenes: towards a complete picture of its physiology and pathogenesis. Nature Reviews Microbiology, 2018. 16(1): p. 32-46. |
| [4] | Al Ohaly, R., et al., Listeria spondylodiscitis: an uncommon etiology of a common condition; a case report. BMC Infectious Diseases, 2020. 20(1): p. 1-4. |
| [5] | Ryser, E. T., Listeria. Foodborne Infections and Intoxications. 2021, Elsevier Academic press, p. 201-220. |
| [6] | Wadhwa Desai, R. and M. A. Smith, Pregnancy-related listeriosis. Birth defects research, 2017. 109(5): p. 324-335. |
| [7] | True, H., et al., Monocytes and macrophages in pregnancy: The good, the bad, and the ugly. Immunological Reviews, 2022. Volume 308, Issue 1, Pages 77-92. |
| [8] | Goudar, V. and N. Prasad, A Critical Review on Listeria monocytogenes. International Journal of Innovations in Biological and Chemical Sciences, Volume 13, 2020, 95-103.2. |
| [9] | Madjunkov, M., S. Chaudhry, and S. Ito, Listeriosis during pregnancy. Archives of gynecology and obstetrics, 2017. 296(2): p. 143-152. |
| [10] | Hunjak, B., et al., Listeria monocytogenes–clinical significance in pregnant women and newborns. International Journal of Infectious Diseases, 2019. 79: p. 88. |
| [11] | Lamond, N. M., et al., Cardiotropic isolates of Listeria monocytogenes with enhanced vertical transmission dependent upon the bacterial surface protein InlB. Infection and Immunity, 2021. 89(2): p. e00321-20. |
| [12] | Zhao, Q., et al., Prevalence and transmission characteristics of Listeria species from ruminants in farm and slaughtering environments in China. Emerging microbes & infections, 2021. 10(1): p. 356-364. |
| [13] | Skowron, K., et al., Characteristics of Listeria monocytogenes strains isolated from milk and humans and the possibility of milk-borne strains transmission. Polish journal of microbiology, 2019. 68(3): p. 353. |
| [14] | Kurpas, M., K. Wieczorek, and J. Osek, Ready-to-eat meat products as a source of Listeria monocytogenes. Journal of veterinary research, 2018. 62(1): p. 49. |
| [15] | Fagerlund, A., S. Langsrud, and T. Møretrø, In-depth longitudinal study of Listeria monocytogenes ST9 isolates from the meat processing industry: resolving diversity and transmission patterns using whole-genome sequencing. Applied and environmental microbiology, 2020. 86(14): p. e00579-20. |
| [16] | Craig, A. M., et al., Listeriosis in pregnancy: a review. Obstetrical & gynecological survey, 2019. 74(6): p. 362-368. |
| [17] | Roberts, B. N., et al., Listeria monocytogenes response to anaerobic environments. Pathogens, 2020. 9(3): p. 210. |
| [18] | Rodriguez, C., et al., Listeria monocytogenes dissemination in farming and primary production: Sources, shedding and control measures. Food Control, 2021. 120: p. 107540. |
| [19] | Wang, Z., et al., An Update Review on Listeria Infection in Pregnancy. Infection and Drug Resistance, 2021. 14: p. 1967. |
| [20] | Etty, M.-C., et al., Effect of the optimized selective enrichment medium on the expression of the p60 protein used as Listeria monocytogenes antigen in specific sandwich ELISA. Research in microbiology, 2019. 170(4-5): p. 182-191. |
| [21] | Al-dorri, A. Z. R. A., Study of bacteria Listeria monocytogenes in spontaneous aborted women in Salah Al-deen province. Tikrit Journal of Pure Science, 2018. 21(3): p. 12-17. |
| [22] | Valenti, M., et al., Listeria monocytogenes infections: presentation, diagnosis and treatment. British Journal of Hospital Medicine, 2021. 82(10): p. 1-6. |
| [23] | Xu, L., Y. Du, and Y. Wu, Neglected listeria infection in pregnancy in China: 93 cases. The Journal of Maternal-Fetal & Neonatal Medicine, 2022: p. 1-9. |
| [24] | Feyisa, A., M. Negash, and Y. Melka, Urban green infrastructure affects woody plant diversity and carbon stock in Hawassa city in Ethiopia. Arboricultural Journal, 2022: p. 1-15. |
| [25] | FEDD Hawassa, F. A. E. D. D. O. H. C., Socio-Economic and Geo-Spatial Data Analysis and Dissemination Core Work Process: Socio-Economic Profile. 2019: Hawassa, Ethiopia: FEDD-Hawassa. |
| [26] | Muleta, D., et al., Bacterial Profile and Their Antimicrobial Resistance Pattern among Adult Patients with Suspected Bloodstream Infection at Jimma University Medical Center, Ethiopia. Sciences, 2022. 11(6): p. 104-116. |
| [27] | EUCAST, Breakpoint tables for interpretation of MICs and zone diameters. T. E. C. O. A. S. Testing. Vol. Version 12.0,. 2022. |
| [28] | Wayne, P., CLSI. Performance Standards for Antimicrobial Susceptibility Testing. 30th ed. |
| [29] | Heidarzadeh, S., et al., Antimicrobial Susceptibility, Serotyping, and Molecular Charac-terization of Antibiotic Resistance Genes in Listeria monocyto-genes Isolated from Pregnant Women with a History of Abortion. Iranian Journal of Public Health, 2021. 50(1): p. 170-179. |
| [30] | Girma, L., et al., Isolation and characterization of Listeria monocytogenes among women attending Jimma University medical center, Southwest Ethiopia. BMC Infectious Diseases, 2021. 21(1): p. 1-6. |
| [31] | Heidari, S. and M. M. Soltan Dallal, Prevalence of Listeria monocytogenes isolated from pregnant women with and without history of abortion and detection of hemolysin (hlyA) gene in clinical samples. Scientific Journal of Kurdistan University of Medical Sciences, 2018. 23(5): p. 96-107. |
| [32] | Freitag, I. G. R., et al., Prevalence of Listeria monocytogenes fecal carriers in HIV-infected and-uninfected pregnant women from Brazil. Brazilian Journal of Microbiology, 2021. 52(4): p. 2081-2084. |
| [33] | Jha, B. K., N. Adhikari, and S. Rajkumari, Isolation, Identification and Antibiotic Susceptibility Patterns of Listeria Monocytogens from Pregnant Women. Journal of College of Medical Sciences-Nepal, 2021. 17(3). |
| [34] | Welekidan, L. N., et al., Prevalence and drug resistance pattern of Listeria monocytogenes among pregnant women in Tigray region, Northern Ethiopia: a cross-sectional study. BMC research notes, 2019. 12(1): p. 1-6. |
| [35] | Singaravelu, B., G. Babu, and S. K. Kannan, Prevalence of Pregnancy Associated Listerioisis in and around Puducherry, India. Indian Journal of Public Health Research & Development, 2019. 10(2). |
| [36] | Diriba, K., E. Awulachew, and K. Diribsa, The prevalence of Listeria species in different food items of animal and plant origin in Ethiopia: a systematic review and meta-analysis. European Journal of Medical Research, 2021. 26(1): p. 1-9. |
| [37] | Kayode, A. J. and A. I. Okoh, Incidence and genetic diversity of multi-drug resistant Listeria monocytogenes isolates recovered from fruits and vegetables in the Eastern Cape Province, South Africa. International Journal of Food Microbiology, 2022. 363: p. 109513. |
| [38] | Borena, B. M., et al., Listeria Species Occurrence and Associated Risk Factors and Antibiogram of Listeria Monocytogenes in Milk and Milk Products in Ambo, Holeta, and Bako Towns, Oromia Regional State, Ethiopia. Veterinary Medicine International, 2022. 2022. |
| [39] | Anwar, T. M., et al., Genetic diversity, virulence factors, and antimicrobial resistance of Listeria monocytogenes from food, livestock, and clinical samples between 2002 and 2019 in China. International Journal of Food Microbiology, 2022. 366: p. 109572. |
APA Style
Lemma, F. D., Adinew, A. A., Reda, D. Y., Gidebo, D. D., Bankere, A. W. (2024). Prevalence, Antibiotics Susceptibility Profile of Listeria Monocytogenes, and Its Associated Risk Factors Among Pregnant Women Attending Millennium Health Center. Journal of Gynecology and Obstetrics, 12(2), 20-30. https://doi.org/10.11648/j.jgo.20241202.12
ACS Style
Lemma, F. D.; Adinew, A. A.; Reda, D. Y.; Gidebo, D. D.; Bankere, A. W. Prevalence, Antibiotics Susceptibility Profile of Listeria Monocytogenes, and Its Associated Risk Factors Among Pregnant Women Attending Millennium Health Center. J. Gynecol. Obstet. 2024, 12(2), 20-30. doi: 10.11648/j.jgo.20241202.12
AMA Style
Lemma FD, Adinew AA, Reda DY, Gidebo DD, Bankere AW. Prevalence, Antibiotics Susceptibility Profile of Listeria Monocytogenes, and Its Associated Risk Factors Among Pregnant Women Attending Millennium Health Center. J Gynecol Obstet. 2024;12(2):20-30. doi: 10.11648/j.jgo.20241202.12
@article{10.11648/j.jgo.20241202.12,
author = {Fikru Deressa Lemma and Alegntaw Abate Adinew and Dawit Yihdego Reda and Deresse Daka Gidebo and Assefa Washo Bankere},
title = {Prevalence, Antibiotics Susceptibility Profile of Listeria Monocytogenes, and Its Associated Risk Factors Among Pregnant Women Attending Millennium Health Center
},
journal = {Journal of Gynecology and Obstetrics},
volume = {12},
number = {2},
pages = {20-30},
doi = {10.11648/j.jgo.20241202.12},
url = {https://doi.org/10.11648/j.jgo.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20241202.12},
abstract = {Background: Listeria monocytogenes is a facultative intracellular pathogen that causes serious invasive infections in pregnant women, resulting in disseminated fetal infections, abortions, and still-births. Although it causes a greater burden on pregnant women and their infants, the case in Ethiopia is overlooked, and there is a scarcity of data on L. monocytogenes, particularly in the southern parts of Ethiopia. Therefore, this study aimed to determine the prevalence and, antibiotics susceptibility of L. monocytogenes and its associated risk factors among pregnant women attending the Millennium Health Center, Hawassa, Ethiopia. Method: A cross-sectional study was conducted on 203 pregnant women between May 30 and July 30, 2022. Socio-demographic data and 5 ml venous blood samples were collected from pregnant women using structured questionnaire. Data were analyzed using SPSS version 25. Bivariate logistic regression was carried out then variables with pp-values Results: The overall prevalence of L. monocytogenes among pregnant women was found to be 11/203 (5.42%; 95% CI=2.88-9.38). L. monocytogenes was resistant to benzyl penicillin (90.91%) and meropenem (81.82%), but susceptible to ampicillin (90.91%). Raw meat (AOR=6.99; 95% CI=1.39-35.14), p=0.018), uncooked vegetables (AOR=6.62; 95% CI=1.04-42.30), p=0.046), unpasteurized milk (AOR=7.56; 95% CI=1.33-42.97), p=0.023) and fever (AOR=14.65; 95% CI=3.15-68.15), p=0.001) were significantly associated with L. monocytogenes infection. Conclusion: L. monocytogenes was resistant to benzyl penicillin, meropenem, erythromycin, and sulfamethoxazole but susceptible to ampicillin. Raw meat, uncooked vegetables, unpasteurized milk, and fever were significantly associated with L. monocytogenes.
},
year = {2024}
}
TY - JOUR T1 - Prevalence, Antibiotics Susceptibility Profile of Listeria Monocytogenes, and Its Associated Risk Factors Among Pregnant Women Attending Millennium Health Center AU - Fikru Deressa Lemma AU - Alegntaw Abate Adinew AU - Dawit Yihdego Reda AU - Deresse Daka Gidebo AU - Assefa Washo Bankere Y1 - 2024/04/17 PY - 2024 N1 - https://doi.org/10.11648/j.jgo.20241202.12 DO - 10.11648/j.jgo.20241202.12 T2 - Journal of Gynecology and Obstetrics JF - Journal of Gynecology and Obstetrics JO - Journal of Gynecology and Obstetrics SP - 20 EP - 30 PB - Science Publishing Group SN - 2376-7820 UR - https://doi.org/10.11648/j.jgo.20241202.12 AB - Background: Listeria monocytogenes is a facultative intracellular pathogen that causes serious invasive infections in pregnant women, resulting in disseminated fetal infections, abortions, and still-births. Although it causes a greater burden on pregnant women and their infants, the case in Ethiopia is overlooked, and there is a scarcity of data on L. monocytogenes, particularly in the southern parts of Ethiopia. Therefore, this study aimed to determine the prevalence and, antibiotics susceptibility of L. monocytogenes and its associated risk factors among pregnant women attending the Millennium Health Center, Hawassa, Ethiopia. Method: A cross-sectional study was conducted on 203 pregnant women between May 30 and July 30, 2022. Socio-demographic data and 5 ml venous blood samples were collected from pregnant women using structured questionnaire. Data were analyzed using SPSS version 25. Bivariate logistic regression was carried out then variables with pp-values Results: The overall prevalence of L. monocytogenes among pregnant women was found to be 11/203 (5.42%; 95% CI=2.88-9.38). L. monocytogenes was resistant to benzyl penicillin (90.91%) and meropenem (81.82%), but susceptible to ampicillin (90.91%). Raw meat (AOR=6.99; 95% CI=1.39-35.14), p=0.018), uncooked vegetables (AOR=6.62; 95% CI=1.04-42.30), p=0.046), unpasteurized milk (AOR=7.56; 95% CI=1.33-42.97), p=0.023) and fever (AOR=14.65; 95% CI=3.15-68.15), p=0.001) were significantly associated with L. monocytogenes infection. Conclusion: L. monocytogenes was resistant to benzyl penicillin, meropenem, erythromycin, and sulfamethoxazole but susceptible to ampicillin. Raw meat, uncooked vegetables, unpasteurized milk, and fever were significantly associated with L. monocytogenes. VL - 12 IS - 2 ER -
Department of Medical Laboratory Science, College of Medicine and Health Sciences, Werabe University, Werabe, Ethiopia
Department of Medical Laboratory Science, Hawassa College of Health Sciences, Hawassa, Ethiopia
Department of Microbiology, School of Medical Laboratory Science, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia
Information