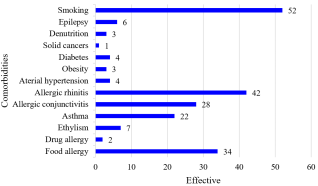
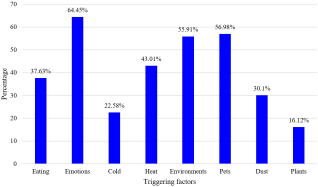
Atopic dermatitis is a chronic inflammatory skin disorder which develops in flare-ups. It is a global public health problem, and in Madagascar, its prevalence is 5.6% in children and 0.5% in adults people. Atopic dermatitis is often associated with various comorbidities. The aim of this study is to describe the profile of comorbidities associated with atopic dermatitis. A cross-sectional and analytical study was conducted over a five-year period from January 2019 to March 2023, involving pediatric and adult patients with atopic dermatitis seen at the department of Dermatology at Joseph Raseta Befelatanana Hospital, Antananarivo. Cases with incomplete and unusable medical records were excluded. Out of 6,495 consultations, 93 cases of atopic dermatitis were observed, with a prevalence of 1.43%, a female predominance with a sex ratio of 0.83, and the average age was 10 years. We found 13 comorbidities, with personal atopy being the most common (55.91%), followed by smoking (55.91%). A significant correlation was found between passive smoking and the occurrence of atopic dermatitis (p = 0.002). A significant association was also observed between personal atopy and flare-ups of atopic dermatitis (p < 0.05). These comorbidities have an impact on the quality of life and psychiatric status of patients. Additionally, several factors (environmental, dietary, climatic) were identified as potential triggers for atopic dermatitis in our study. Our study confirms the presence of comorbidities in patients with atopic dermatitis. Atopic dermatitis has implications for quality of life and psychological well-being.
| Published in | Medicine and Health Sciences (Volume 2, Issue 2) |
| DOI | 10.11648/j.mhs.20260202.14 |
| Page(s) | 97-102 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Antananarivo, Atopy, Comorbidities, Atopic Dermatitis, Madagascar
Comorbidities | Frequency n = 93 (100%) |
|---|---|
Personal atopy | 52 (55.91) |
Asthma | 22 (42.3) |
Allergic conjunctivitis | 28 (53.84) |
Hay fever | 0 (0) |
Allergic rhinitis | 42 (80.76) |
Smoking | 52 (55.91) |
Active smoking | 6 (11.53) |
Passive smoking | 46 (88.46) |
Variables | OR | CI (95%) | p-value |
|---|---|---|---|
Passive smoking | 4.2 | [2.74-215.98] | 0.002 |
Cardiovascular pathology | 24.3 | [2.74-215.98] | 0.0003 |
Arterial hypertension | 10.3 | [1.01-105.03] | 0.02 |
Variables | OR | CI (95%) | p-value |
|---|---|---|---|
Personal atopy | 7.9 | [2.46-25.46] | < 0.05 |
Asthma | 4.1 | [1.5-11.29] | 0.003 |
Allergic conjunctivitis | 3.5 | [1.38-9.22] | 0.004 |
Allergic rhinitis | 6.2 | [2.3-17.1] | < 0.05 |
Food allergy | 3.4 | [1.38-8.77] | 0.004 |
Smoking | 2.04 | [0.8-5.19] | 0.06 |
Consequences | OR | CI (95%) | p-value |
|---|---|---|---|
Sleep disorder | 0.28 | [0.08-0,91] | 0.01 |
Alteration of activities | 4.73 | [1.83-12,18] | 0.001 |
Absenteeism | 12.15 | [3.89-37,88] | < 0.05 |
Stress and anxiety | 14.14 | [3.39-58,99] | < 0.05 |
Family history | Frequency n = 93 (100%) |
|---|---|
History of familial atopy | 54 (58.06) |
Familial asthma | 26 (27.95) |
Familial eczema | 21 (21.5) |
Familial atopic dermatitis | 24 (25.8) |
Cutaneous manifestations | Number of patients n = 93 (100%) |
|---|---|
Erythemato-vesicular lesions | 77 (82.79) |
Weeping lesions | 11 (11.82) |
Cutaneous xerosis | 46 (49.46) |
Local superinfections | 20 (21.5) |
Post-inflammatory hyperpigmentation | 10 (10.75) |
Lichenified lesions | 15 (16.12) |
Location | Number of patients n = 93 (100%) |
|---|---|
Members | 75 (80.64) |
Face | 50 (53.76) |
head and neck | 29 (31.18) |
Trunk | 42 (45.16) |
External genitals | 11 (11.82) |
AD | Atopic Dermatitis |
| [1] | Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI, ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009; 124(6): 1251-1258. e23. |
| [2] |
Staumont D. La dermatite atopique [Internet]. dermato-info.fr. 2021 [cité 30 mars 2023]. Disponible sur:
https://dermato-info.fr/fr/les-maladies-de-la-peau/la-dermatite-atopique |
| [3] | Taïeb A. Atopic dermatitis: definition, epidemiology, natural history, severity and scores. Ann Dermatol Venereol. 2005; 132 Spec No 1: 1S35-43. |
| [4] | Sendrasoa FA, Ranaivo IM, Razanakoto NH, Andrianarison M, Raharolahy O, Ratovonjanahary VT, et al. Epidemiology and associated factors of atopic dermatitis in Malagasy children. Allergy Asthma Clin Immunol. 2020; 16: 4. |
| [5] | Sendrasoa FA, Ramily SL, Razafimaharo TI, Ranaivo IM, Andrianarison M, Raharolahy O, et al. Atopic dermatitis in adults: A cross-sectional study in the department of dermatology, Antananarivo, Madagascar. JAAD Int. 2021; 4: 28‑31. |
| [6] | Brunner PM, Silverberg JI, Guttman-Yassky E, Paller AS, Kabashima K, Amagai M, et al. Increasing Comorbidities Suggest that Atopic Dermatitis Is a Systemic Disorder. J Invest Dermatol. 2017; 137(1): 18‑25. |
| [7] | Thijs JL, Strickland I, Bruijnzeel-Koomen CAFM, Nierkens S, Giovannone B, Knol EF, et al. Serum biomarker profiles suggest that atopic dermatitis is a systemic disease. J Allergy Clin Immunol. 2018; 141(4): 1523‑6. |
| [8] | Rapelanoro Rabenja F, Raobijaona H, Rabenja N, Ratrimoarivony C, Ravelomanana N, Rasamindrakotroka A. La dermatite atopique chez le nourrisson et l’enfant. J Med Ther. 2000; 3(2): 2S41-42. |
| [9] | Barbarot S, Auziere S, Gadkari A, Girolomoni G, Puig L, Simpson EL, et al. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy. 2018; 73(6): 1284‑93. |
| [10] | Hello M, Aubert H, Bernier C, Néel A, Barbarot S. Atopic dermatitis of the adult. Rev Med Interne. 2016; 37(2): 91‑9. |
| [11] | Ezzedine K, Kechichian E. Epidemiology of atopic dermatitis. Ann Dermatol Venereol. 2017; 144 Suppl 5: VS4‑7. |
| [12] | Zeppa L, Bellini V, Lisi. Atopic dermatitis in adults. 2011; 22(1): 40‑6. |
| [13] | Lara A. Faut-il recommander l’arrêt du tabac aux patients souffrant de dermatite atopique ? [Internet]. Faut-il recommander l’arrêt du tabac aux patients souffrant de dermatite atopique ? [Should smoking cessation be recommended for patients with atopic dermatitis? [Internet]. Should smoking cessation be recommended for patients with atopic dermatitis?] | Univadis. 2016 [cité 2 avr 2023]. Disponible sur: |
| [14] | Kantor R, Kim A, Thyssen JP, Silverberg JI. Association of atopic dermatitis with smoking: A systematic review and meta-analysis. J Am Acad Dermatol. 2016; 75(6): 1119-1125. e1. |
| [15] | Carson CG, Halkjaer LB, Jensen SM, Bisgaard H. Alcohol intake in pregnancy increases the child’s risk of atopic dermatitis. the COPSAC prospective birth cohort study of a high risk population. PLoS One. 2012; 7(8): e42710. |
| [16] | Benhamou AH, Eigenmann PA. Dermatite atopique et allergies alimentaires. Rev Med Suisse. 2007; 108: 1038‑43. |
| [17] | Drucker A m., Qureshi A a., Dummer T j. b., Parker L, Li WQ. Atopic dermatitis and risk of hypertension, type 2 diabetes, myocardial infarction and stroke in a cross-sectional analysis from the Canadian Partnership for Tomorrow Project. British Journal of Dermatology. 2017; 177(4): 1043‑51. |
| [18] | Shalom G, Dreiher J, Kridin K, Horev A, Khoury R, Battat E, et al. Atopic dermatitis and the metabolic syndrome: a cross-sectional study of 116 816 patients. J Eur Acad Dermatol Venereol. 2019; 33(9): 1762‑7. |
| [19] | Drucker A, Li WQ, Lin L, Cho E, Li T, Camargo C, et al. Atopic dermatitis (eczema) in US female nurses: lifestyle risk factors and atopic co-morbidities. Br J Dermatol. 2016; 174(6): 1395‑7. |
| [20] | Zhang A, Silverberg JI. Association of atopic dermatitis with being overweight and obese: a systematic review and metaanalysis. J Am Acad Dermatol. 2015; 72(4): 606-616. e4. |
| [21] | Lin CH, Wei CC, Lin CL, Lin WC, Kao CH. Childhood type 1 diabetes may increase the risk of atopic dermatitis. Br J Dermatol. 2016; 174(1): 88‑94. |
| [22] | Thyssen JP, Halling-Overgaard AS, Andersen YMF, Gislason G, Skov L, Egeberg A. The association with cardiovascular disease and type 2 diabetes in adults with atopic dermatitis: a systematic review and meta-analysis. Br J Dermatol. 2018; 178(6): 1272‑9. |
| [23] | Halling-Overgaard AS, Ravnborg N, Silverberg JI, Egeberg A, Thyssen JP. Atopic dermatitis and cancer in solid organs: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2019; 33(2): e81‑2. |
| [24] | Cribier B. Comorbidités de la dermatite atopique. Annales de Dermatologie et de Vénéréologie. 2019; 146(12, Supplement 3): 12S67‑75. |
| [25] | Wang H, Diepgen TL. Atopic dermatitis and cancer risk. British Journal of Dermatology. 2006; 154(2): 205‑10. |
| [26] | Chen MH, Wu YH, Su TP, Chen YS, Hsu JW, Huang KL, et al. Risk of epilepsy among patients with atopic dermatitis: a nationwide longitudinal study. Epilepsia. 2014; 55(8): 1307‑12. |
| [27] | Aronica E, Crino PB. Inflammation in epilepsy: clinical observations. Epilepsia. 2011; 52 Suppl 3: 26‑32. |
| [28] | Vezzani A, Aronica E, Mazarati A, Pittman QJ. Epilepsy and brain inflammation. Exp Neurol. 2013; 244: 11‑21. |
APA Style
Rakotonandrasana, F., Sendrasoa, F. A., Raharolahy, O., Manjarimanana, F., Andriatahina, H. F. P., et al. (2026). Profile of Comorbidities Associated with Atopic Dermatitis at the Department of Dermatology of Antananarivo, Madagascar. Medicine and Health Sciences, 2(2), 97-102. https://doi.org/10.11648/j.mhs.20260202.14
ACS Style
Rakotonandrasana, F.; Sendrasoa, F. A.; Raharolahy, O.; Manjarimanana, F.; Andriatahina, H. F. P., et al. Profile of Comorbidities Associated with Atopic Dermatitis at the Department of Dermatology of Antananarivo, Madagascar. Med. Health Sci. 2026, 2(2), 97-102. doi: 10.11648/j.mhs.20260202.14
AMA Style
Rakotonandrasana F, Sendrasoa FA, Raharolahy O, Manjarimanana F, Andriatahina HFP, et al. Profile of Comorbidities Associated with Atopic Dermatitis at the Department of Dermatology of Antananarivo, Madagascar. Med Health Sci. 2026;2(2):97-102. doi: 10.11648/j.mhs.20260202.14
@article{10.11648/j.mhs.20260202.14,
author = {Fenohasina Rakotonandrasana and Fandresena Arilala Sendrasoa and Onivola Raharolahy and Florine Manjarimanana and Herin’Ny Fitiavana Princia Andriatahina and Stevy Desana and Voahanginirina Nathalie Ralimalala and Tsiory Iarintsoa Razafimaharo and Volatantely Tobiniaina Ratovonjanahary and Moril Sata and Mendrika Fifaliana Rakotoarisaona and Naina Harinjara Razanakoto and Malalaniaina Andrianarison and Irina Mamisoa Ranaivo and Lala Soavina Ramarozatovo and Fahafahantsoa Rabenja Rapelanoro},
title = {Profile of Comorbidities Associated with Atopic Dermatitis at the Department of Dermatology of Antananarivo, Madagascar},
journal = {Medicine and Health Sciences},
volume = {2},
number = {2},
pages = {97-102},
doi = {10.11648/j.mhs.20260202.14},
url = {https://doi.org/10.11648/j.mhs.20260202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.mhs.20260202.14},
abstract = {Atopic dermatitis is a chronic inflammatory skin disorder which develops in flare-ups. It is a global public health problem, and in Madagascar, its prevalence is 5.6% in children and 0.5% in adults people. Atopic dermatitis is often associated with various comorbidities. The aim of this study is to describe the profile of comorbidities associated with atopic dermatitis. A cross-sectional and analytical study was conducted over a five-year period from January 2019 to March 2023, involving pediatric and adult patients with atopic dermatitis seen at the department of Dermatology at Joseph Raseta Befelatanana Hospital, Antananarivo. Cases with incomplete and unusable medical records were excluded. Out of 6,495 consultations, 93 cases of atopic dermatitis were observed, with a prevalence of 1.43%, a female predominance with a sex ratio of 0.83, and the average age was 10 years. We found 13 comorbidities, with personal atopy being the most common (55.91%), followed by smoking (55.91%). A significant correlation was found between passive smoking and the occurrence of atopic dermatitis (p = 0.002). A significant association was also observed between personal atopy and flare-ups of atopic dermatitis (p ). These comorbidities have an impact on the quality of life and psychiatric status of patients. Additionally, several factors (environmental, dietary, climatic) were identified as potential triggers for atopic dermatitis in our study. Our study confirms the presence of comorbidities in patients with atopic dermatitis. Atopic dermatitis has implications for quality of life and psychological well-being.},
year = {2026}
}
TY - JOUR T1 - Profile of Comorbidities Associated with Atopic Dermatitis at the Department of Dermatology of Antananarivo, Madagascar AU - Fenohasina Rakotonandrasana AU - Fandresena Arilala Sendrasoa AU - Onivola Raharolahy AU - Florine Manjarimanana AU - Herin’Ny Fitiavana Princia Andriatahina AU - Stevy Desana AU - Voahanginirina Nathalie Ralimalala AU - Tsiory Iarintsoa Razafimaharo AU - Volatantely Tobiniaina Ratovonjanahary AU - Moril Sata AU - Mendrika Fifaliana Rakotoarisaona AU - Naina Harinjara Razanakoto AU - Malalaniaina Andrianarison AU - Irina Mamisoa Ranaivo AU - Lala Soavina Ramarozatovo AU - Fahafahantsoa Rabenja Rapelanoro Y1 - 2026/04/15 PY - 2026 N1 - https://doi.org/10.11648/j.mhs.20260202.14 DO - 10.11648/j.mhs.20260202.14 T2 - Medicine and Health Sciences JF - Medicine and Health Sciences JO - Medicine and Health Sciences SP - 97 EP - 102 PB - Science Publishing Group SN - 3070-6300 UR - https://doi.org/10.11648/j.mhs.20260202.14 AB - Atopic dermatitis is a chronic inflammatory skin disorder which develops in flare-ups. It is a global public health problem, and in Madagascar, its prevalence is 5.6% in children and 0.5% in adults people. Atopic dermatitis is often associated with various comorbidities. The aim of this study is to describe the profile of comorbidities associated with atopic dermatitis. A cross-sectional and analytical study was conducted over a five-year period from January 2019 to March 2023, involving pediatric and adult patients with atopic dermatitis seen at the department of Dermatology at Joseph Raseta Befelatanana Hospital, Antananarivo. Cases with incomplete and unusable medical records were excluded. Out of 6,495 consultations, 93 cases of atopic dermatitis were observed, with a prevalence of 1.43%, a female predominance with a sex ratio of 0.83, and the average age was 10 years. We found 13 comorbidities, with personal atopy being the most common (55.91%), followed by smoking (55.91%). A significant correlation was found between passive smoking and the occurrence of atopic dermatitis (p = 0.002). A significant association was also observed between personal atopy and flare-ups of atopic dermatitis (p ). These comorbidities have an impact on the quality of life and psychiatric status of patients. Additionally, several factors (environmental, dietary, climatic) were identified as potential triggers for atopic dermatitis in our study. Our study confirms the presence of comorbidities in patients with atopic dermatitis. Atopic dermatitis has implications for quality of life and psychological well-being. VL - 2 IS - 2 ER -
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar;Department of Dermatology, Place Kabary Hospital, Antsiranana, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, Place Kabary Hospital, Antsiranana, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, University Hospital of Morafeno, Toamasina, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, Place Kabary Hospital, Antsiranana, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Department of Dermatology, Joseph Raseta Befelatanana Hospital, Antananarivo, Madagascar
Information