Background: Non-reassuring fetal heart rate, which indicates fetal hypoxia due to inadequate oxygen supply, is the most common reason for increasing cesarean sections and operative vaginal deliveries beyond world health organization recommendations. However, there is a lack of research on this issue nationally and no studies have been conducted in the study area. Objective: This study aimed to assess the prevalence and factors associated with non-reassuring fetal heart rate among laboring mothers who gave birth at Jigjiga Public Hospital, Eastern Ethiopia, 2024 Methods: An institution-based cross-sectional study was conducted among 281 laboring mothers who gave birth at Jigjiga Public Hospital from April 15 to May 15, 2024. Study subjects were selected using a systematic random sampling technique. Data was collected through pretested, interviewer-administered, semi-structured questionnaires, then entered into EPI-DATA Version 4.6 and exported to SPSS Version 25 for analysis. Binary logistic regression analyses were performed to identify factors associated with non-reassuring fetal heart rate. Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were calculated to assess the strength of associations, with statistical significance declared at a p-value < 0.05. Model fitness was assessed using the Hosmer-Lemeshow test. Results: The prevalence of non-reassuring fetal heart rate was 22.4% (95% CI: 17.5-27.5). Meconium-stained amniotic fluid (AOR = 6.239, 95% CI: 2.726-12.281), bloody amniotic fluid (AOR = 6.232, 95% CI: 2.726-19.183), not having antenatal contact (AOR = 4.196, 95% CI: 1.859-9.473), obstetric complications (AOR = 9.562, 95% CI: 4.139-20.090), and rural residence (AOR = 3.32, 95% CI: 1.32-8.346) were significantly associated with Non-reassuring fetal heart rate. Conclusions: The overall prevalence of non-reassuring fetal heart rate was high. Significant associations were found with residing in rural areas, having obstetric complications, meconium- and blood-stained amniotic fluid, and not having anti natal care visits.
| Published in | Science Journal of Public Health (Volume 13, Issue 3) |
| DOI | 10.11648/j.sjph.20251303.14 |
| Page(s) | 134-145 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Non-reassuring Fetal Heart Rate, Jigjiga, Ethiopia
Sr. no | Variables | CI | Power | Prevalence among unexposed group | Prevalence among exposed group | AOR | Non response rate | Total sample size | Reference |
|---|---|---|---|---|---|---|---|---|---|
1 | Referral from health facility | 95% | 80 | 36.81 | 12.98 | 3.90 | 10 | 130 | (27) |
2 | Augmentation of labor | 95% | 80 | 42.30 | 10.73 | 3.24 | 10 | 140 | (28) |
3 | Current pregnancy complication | 95% | 80 | 35.41 | 18.36 | 2.44 | 10 | 257 | (27) |
Variable | Category | Frequency (n) | Percentage% |
|---|---|---|---|
Maternal age | 15 – 25 | 96 | 34.2 |
26 – 35 | 132 | 47 | |
36 – 45 | 53 | 18.9 | |
Residence | Urban | 211 | 75.1 |
Rural | 70 | 24.9 | |
Marital status | Married | 259 | 92.2 |
Single | 17 | 6 | |
Others* | 5 | 1.8 | |
Occupational status of the mother | House wife | 177 | 63 |
Marchent | 45 | 16 | |
Governmental employe | 42 | 14.9 | |
Others* | 17 | 6.2 | |
Educational status of the mother | Havingno forma leducation | 179 | 63.6 |
Having formal education | 102 | 36.4 | |
Religion | Muslim | 230 | 81.9 |
Orthodox | 31 | 11 | |
Protestant | 19 | 6.8 | |
Catholic | 1 | 0.4 |
Variable | Category | Frequency (n) | Percentage% |
|---|---|---|---|
Parity | Primi parous | 52 | 18.5 |
Multi parous | 229 | 81.5 | |
Gravidity | Primi gravida | 48 | 17.1 |
Multi gravida | 233 | 82.9 | |
ANC visit | Yes | 121 | 43.1 |
No | 160 | 56.9 | |
Frequency of ANC visit (N=121) | <4 | 37 | 30.6 |
≥ 4 | 84 | 69.4 | |
Current obstetric history | Yes | 61 | 21.7 |
No | 220 | 78.3 | |
Hematocrit level | Anemic | 58 | 20.6 |
Normal | 223 | 79.4 | |
MUAC | Malnourished | 76 | 27 |
Normal | 205 | 73 |
Variable | Category | Frequency (n) | Percentage% |
|---|---|---|---|
Birth weight | <2500 | 11 | 3.5 |
2500-3999 | 170 | 63.7 | |
>=4000 | 91 | 32.4 | |
Duration of ROM | >=12 Hr | 54 | 19.2 |
<12 Hr | 227 | 80.2 | |
Mode of delivery | SVD | 195 | 69.4 |
C/S | 30 | 10.7 | |
Vacuum extraction | 43 | 15.3 | |
Other* | 13 | 4.6 | |
Presentation | Cephalic | 240 | 85.4 |
Breach | 32 | 11.4 | |
Others* | 9 | 3.2 | |
Color of amniotic fluid | Clear | 188 | 66.9 |
Blood containing | 27 | 9.6 | |
Meconium | 66 | 23.5 |
Variables | Categories | NRFHR | P-value | COR (95%C. I) | AOR (95%C. I) | P –value | |
|---|---|---|---|---|---|---|---|
YES | NO | ||||||
Residence | Urban | 31 | 180 | 1 | |||
Rural | 32 | 38 | 0.000 | 4.8 (2.7-8.9) | 3.3 (1.3-8.3) | 0.011 | |
Parity | Primi parous | 15 | 37 | 0.221 | 1.5 (0.8-3.0) | 1.3 (0.5-3.2) | 0.658 |
Multi parous | 48 | 181 | 1 | ||||
ANC visit | Yes | 15 | 106 | 1 | |||
No | 48 | 112 | 0.001 | 3.1 (1.61-5.7) | 4.2 ((1.9 -9.5) | 0.001 | |
MUAC | <23cm | 23 | 53 | 0.057 | 1.8 (0.9-3.3) | 1.8 (0.7-4.4) | 0.189 |
≥23cm | 40 | 165 | 1 | ||||
Obstetric complication | Yes | 34 | 27 | 1 | |||
No | 29 | 191 | 0.000 | 8.3 (4.4-15.7) | 9.5 (4.1-20.1) | 0.000 | |
Color of amniotic fluid | Clear | 22 | 166 | 1 | |||
Bloody | 10 | 17 | 0.001 | 4.4 (1.8-10.9) | 6.2 (2.7-19.1) | 0.002 | |
Meconium | 31 | 35 | 0.000 | 6.7 (3.5-12.9) | 6.2 (2.7-12.3) | 0.000 | |
Hematocrit level | Anemic | 17 | 41 | 0.160 | 1.6 (0.8-3.1) | 1.3 (0.5-3.2) | 0.142 |
Normal | 46 | 177 | 1 | ||||
Referred | Yes | 25 | 42 | 0.001 | 2.8 (1.5-5.1) | 0.7 (0.3-1.7) | 0.390 |
No | 37 | 173 | 1 | ||||
ACOG | American College of Obstetrics and Gynecology |
BPP | Biophysical Profile |
CEFM | Continuous Electronic Fetal Monitoring |
CTG | Cardiotocograph |
C/S | Caesarian Section |
EFW | Estimated Fetal Weight |
FHR | Fetal Heart Rate |
FHRS | Fetal Heart Rate Status |
FPO | Fetal Pulse Oximetry |
FSB | Fresh Still Birth |
FSE | Fetal Scalp Electrode |
FSS | Fetal Scalp Sampling |
GA | Gestational Age |
IA | Intermittent Auscultation |
MSAF | Meconium Stained Amniotic Fluid |
NRFHRP | Non Reassuring Fetal Heart Rate Pattern |
WHO | World Health Organization |
| [1] | KONAR H. DC DUTTA’s. TEXST BOOK OF OBSTETRICS including Perinatology and Contraception. 7th ed Novomber 2013. |
| [2] | Mohan M, Ramawat J, La Monica G, Jayaram P, Fattah SA, Learmont J, et al. Electronic intrapartum fetal monitoring: a systematic review of international clinical practice guidelines. 2021; 1(2): 100008. |
| [3] | Gravett C, Eckert LO, Gravett MG, Dudley DJ, Stringer EM, Mujobu TBM, et al. Non-reassuring fetal status: case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2016; 34(49): 6084. |
| [4] | Ayres-de-Campos D, Spong CY, Chandraharan E. FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography. International Journal of Gynecology & Obstetrics. 2015; 131(1): 13-24. |
| [5] | Monson M, Heuser CC, Esplin I, Einerson B, Butler A, Esplin SMJO, et al. Interpretation of the Fetal Heart Rate Tracing: Fetal Electrocardiogram Versus Standard Monitoring [20O]. 2020; 135: 161S-2S. |
| [6] | Peter Mc AD, Kilian M, James M, Gerry B, Fionnuala B, Brigid D, Geraldine G, Róisín M, Deirdre N:. National Clinical Guideline for Intrapartum Fetal Heart Rate Monitoring. Ireland Dublin: Health Service Executive july 2019.. |
| [7] | Clark SL, Nageotte MP, Garite TJ, Freeman RK, Miller DA, Simpson KR, et al. Intrapartum management of category II fetal heart rate tracings: towards standardization of care. American journal of obstetrics and gynecology. 2013; 209(2): 89-97. |
| [8] | Ekblom A, Målqvist M, Gurung R, Rossley A, Basnet O, Bhattarai P, et al. Factors associated with poor adherence to intrapartum fetal heart monitoring in relationship to intrapartum related death: a prospective cohort study. PLOS Global Public Health. 2022; 2(5): e0000289. |
| [9] | UNICEF W. WHO, World Bank and United Nations on Behalf of UN Inter-agency group for Child Mortality Estimation: Level and trend of Child Mortality 2019. New York: UNICEF. 2019. |
| [10] | Ayebare E, Ndeezi G, Hjelmstedt A, Nankunda J, Tumwine JK, Hanson C, et al. Health care workers’ experiences of managing foetal distress and birth asphyxia at health facilities in Northern Uganda. Reproductive health. 2021; 18(1): 1-11. |
| [11] | Bhatia N, Krishna K. Intraoperative findings in primary caesarean section for non-reassuring fetal status and its correlation with cardiotocography. International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2018; 7(6): 2351-5. |
| [12] | Zeleke GT, Zemedu TG. Modern contraception use and associated factors in Ethiopia: Evidence from the 2019 Ethiopian Mini Demographic and Health Survey. 2022. |
| [13] | Yeoh M, Ameratunga D, Lee J, Beckmann M. Simplifying the language of fetal monitoring. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2019; 59(4): 538-44. |
| [14] | Kassa EM. Clinical Profile and Out Come of Pregnancies with NRFHR in Labor at Three Teaching Hospitals, Addis Ababa, Ethiopia. 2018. |
| [15] | Tofaeono Fueta'ai M. An evaluation of fetal heart monitoring during labour for low-risk women in Samoa (Upolu): Open Access Te Herenga Waka-Victoria University of Wellington; 2023. |
| [16] | Seid SS, Ibro SA, Ahmed AA, Olani Akuma A, Reta EY, Haso TK, et al. Causes and factors associated with neonatal mortality in neonatal intensive care unit (NICU) of Jimma University medical center, Jimma, south West Ethiopia. Pediatric health, medicine and therapeutics. 2019: 39-48. |
| [17] | Cahill AG, Tuuli MG, Stout MJ, López JD, Macones GA. A prospective cohort study of fetal heart rate monitoring: deceleration area is predictive of fetal acidemia. American journal of obstetrics and gynecology. 2018; 218(5): 523. e1-. e12. |
| [18] | Asnake AB, Mezmur H, Desalew A. Non-reassuring fetal heart rate and associated factors among laboring mothers at the public hospitals of South Omo, Southern Ethiopia, 2023: Haramaya University; 2023. |
| [19] | Morgan JA, Hankins ME, Wang Y, Hutchinson D, Sams HL, Voltz JH, et al. Prolonged fetal heart rate decelerations in labor: can we reduce unplanned primary cesarean sections in this group? Advances in Therapy. 2020; 37: 4325-35. |
| [20] | Kc A, Wrammert J, Clark RB, Ewald U, Målqvist M. Inadequate fetal heart rate monitoring and poor use of partogram associated with intrapartum stillbirth: a case-referent study in Nepal. BMC pregnancy and childbirth. 2016; 16: 1-11. |
| [21] | Morokuma S, Michikawa T, Kato K, Sanefuji M, Shibata E, Tsuji M, et al. Non-reassuring foetal status and neonatal irritability in the Japan Environment and Children’s Study: a cohort study. Scientific reports. 2018; 8(1): 15853. |
| [22] | Lu J, Jiang J, Zhou Y, Chen Q. Prediction of non-reassuring fetal status and umbilical artery acidosis by the maternal characteristic and ultrasound prior to induction of labor. BMC Pregnancy and Childbirth. 2021; 21: 1-7. |
| [23] | Housseine N, Punt MC, Mohamed AG, Said SM, Maaløe N, Zuithoff NP, et al. Quality of intrapartum care: direct observations in a low-resource tertiary hospital. Reproductive health. 2020; 17: 1-11. |
| [24] | Borzie K, Jasper N, Southall D, MacDonald R, Kola AA, Dolo O, et al. Monitoring intrapartum fetal heart rates by mothers in labour in two public hospitals: an initiative to improve maternal and neonatal healthcare in Liberia. BMC Pregnancy and Childbirth. 2020; 20(1): 1-24. |
| [25] | Shiferaw Z, Mahad A, Haile S. Maternal satisfaction and associated factors towards institutional delivery service at public hospitals in the Somali region, Eastern Ethiopia. Plos one. 2022; 17(11): e0277224. |
| [26] | Demographic E. Addis Ababa, Ethiopia, and Rockville. Maryland, MA, USA: CSA and ICF. 2016. |
| [27] | Belete E, Bazezew Y, Desta M, Misganaw D, Tefera M. Magnitude, Associated Factors and Immediate Outcomes of Non-Reassuring Fetal Heart Rate Status Among Laboring Mothers at South Gondar Zone Public Hospitals, North, West Ethiopia, 2022; Cross Sectional Study. medRxiv. 2022: 2022.10. 02.22280615. |
| [28] | Kassahun EA, Aweke AM, Getu AA, Gela GB, Limenih SK, Mekonnen ME, et al. Proportion and associated factors of nonreassuring fetal heart rate patterns in Finote Selam Primary Hospital, North West Ethiopia. BioMed Research International. 2020; 2020. |
| [29] | Boonchuan K, Wattananirun K, Boriboonhirunsarn D. Incidence of Intrapartum abnormal fetal heart rate pattern in Siriraj hospital. Thai Journal of Obstetrics and Gynaecology. 2018: 18-26. |
| [30] | Care A. National. 2022. |
| [31] | Minalbat A. Fetal Heart Rate Abnormalities and Associated Factors Among Mothers Who Gave Birth at Tertiary Hospitals, Bahir Dar, North-West Ethiopia 2022. |
| [32] | Ganer Herman H, Tamayev L, Houli R, Miremberg H, Bar J, Kovo MJB. Risk factors for nonreassuring fetal heart rate tracings after artificial rupture of membranes in spontaneous labor. 2018; 45(4): 393-8. |
| [33] | Mdoe PF, Ersdal HL, Mduma ER, Perlman JM, Moshiro R, Wangwe PT, et al. Intermittent fetal heart rate monitoring using a fetoscope or hand held Doppler in rural Tanzania: a randomized controlled trial. BMC pregnancy and childbirth. 2018; 18(1): 1-8. |
| [34] | Abate E, Alamirew K, Admassu E, Derbie AJO, International G. Prevalence and factors associated with meconium-stained amniotic fluid in a tertiary hospital, Northwest Ethiopia: a cross-sectional study. 2021; 2021: 1-8. |
| [35] | FMOH E. Management protocol on selected obstetrics topics for hospitals. December; 2020. |
APA Style
Abasimel, H. Z., Husen, M., Oyato, B. T., Shiferaw, G., Gabre, M. K. (2025). Magnitude and Associated Factors of Non-Reassuring Fetal Heart Rate Among Laboring Mothers at Jigjiga Public Hospitals, Eastern Ethiopia, 2024. Science Journal of Public Health, 13(3), 134-145. https://doi.org/10.11648/j.sjph.20251303.14
ACS Style
Abasimel, H. Z.; Husen, M.; Oyato, B. T.; Shiferaw, G.; Gabre, M. K. Magnitude and Associated Factors of Non-Reassuring Fetal Heart Rate Among Laboring Mothers at Jigjiga Public Hospitals, Eastern Ethiopia, 2024. Sci. J. Public Health 2025, 13(3), 134-145. doi: 10.11648/j.sjph.20251303.14
@article{10.11648/j.sjph.20251303.14,
author = {Husen Zakir Abasimel and Muna Husen and Befekadu Tesfaye Oyato and Getachew Shiferaw and Misgana Kebede Gabre},
title = {Magnitude and Associated Factors of Non-Reassuring Fetal Heart Rate Among Laboring Mothers at Jigjiga Public Hospitals, Eastern Ethiopia, 2024},
journal = {Science Journal of Public Health},
volume = {13},
number = {3},
pages = {134-145},
doi = {10.11648/j.sjph.20251303.14},
url = {https://doi.org/10.11648/j.sjph.20251303.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251303.14},
abstract = {Background: Non-reassuring fetal heart rate, which indicates fetal hypoxia due to inadequate oxygen supply, is the most common reason for increasing cesarean sections and operative vaginal deliveries beyond world health organization recommendations. However, there is a lack of research on this issue nationally and no studies have been conducted in the study area. Objective: This study aimed to assess the prevalence and factors associated with non-reassuring fetal heart rate among laboring mothers who gave birth at Jigjiga Public Hospital, Eastern Ethiopia, 2024 Methods: An institution-based cross-sectional study was conducted among 281 laboring mothers who gave birth at Jigjiga Public Hospital from April 15 to May 15, 2024. Study subjects were selected using a systematic random sampling technique. Data was collected through pretested, interviewer-administered, semi-structured questionnaires, then entered into EPI-DATA Version 4.6 and exported to SPSS Version 25 for analysis. Binary logistic regression analyses were performed to identify factors associated with non-reassuring fetal heart rate. Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were calculated to assess the strength of associations, with statistical significance declared at a p-value Results: The prevalence of non-reassuring fetal heart rate was 22.4% (95% CI: 17.5-27.5). Meconium-stained amniotic fluid (AOR = 6.239, 95% CI: 2.726-12.281), bloody amniotic fluid (AOR = 6.232, 95% CI: 2.726-19.183), not having antenatal contact (AOR = 4.196, 95% CI: 1.859-9.473), obstetric complications (AOR = 9.562, 95% CI: 4.139-20.090), and rural residence (AOR = 3.32, 95% CI: 1.32-8.346) were significantly associated with Non-reassuring fetal heart rate. Conclusions: The overall prevalence of non-reassuring fetal heart rate was high. Significant associations were found with residing in rural areas, having obstetric complications, meconium- and blood-stained amniotic fluid, and not having anti natal care visits.},
year = {2025}
}
TY - JOUR T1 - Magnitude and Associated Factors of Non-Reassuring Fetal Heart Rate Among Laboring Mothers at Jigjiga Public Hospitals, Eastern Ethiopia, 2024 AU - Husen Zakir Abasimel AU - Muna Husen AU - Befekadu Tesfaye Oyato AU - Getachew Shiferaw AU - Misgana Kebede Gabre Y1 - 2025/06/23 PY - 2025 N1 - https://doi.org/10.11648/j.sjph.20251303.14 DO - 10.11648/j.sjph.20251303.14 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 134 EP - 145 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20251303.14 AB - Background: Non-reassuring fetal heart rate, which indicates fetal hypoxia due to inadequate oxygen supply, is the most common reason for increasing cesarean sections and operative vaginal deliveries beyond world health organization recommendations. However, there is a lack of research on this issue nationally and no studies have been conducted in the study area. Objective: This study aimed to assess the prevalence and factors associated with non-reassuring fetal heart rate among laboring mothers who gave birth at Jigjiga Public Hospital, Eastern Ethiopia, 2024 Methods: An institution-based cross-sectional study was conducted among 281 laboring mothers who gave birth at Jigjiga Public Hospital from April 15 to May 15, 2024. Study subjects were selected using a systematic random sampling technique. Data was collected through pretested, interviewer-administered, semi-structured questionnaires, then entered into EPI-DATA Version 4.6 and exported to SPSS Version 25 for analysis. Binary logistic regression analyses were performed to identify factors associated with non-reassuring fetal heart rate. Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were calculated to assess the strength of associations, with statistical significance declared at a p-value Results: The prevalence of non-reassuring fetal heart rate was 22.4% (95% CI: 17.5-27.5). Meconium-stained amniotic fluid (AOR = 6.239, 95% CI: 2.726-12.281), bloody amniotic fluid (AOR = 6.232, 95% CI: 2.726-19.183), not having antenatal contact (AOR = 4.196, 95% CI: 1.859-9.473), obstetric complications (AOR = 9.562, 95% CI: 4.139-20.090), and rural residence (AOR = 3.32, 95% CI: 1.32-8.346) were significantly associated with Non-reassuring fetal heart rate. Conclusions: The overall prevalence of non-reassuring fetal heart rate was high. Significant associations were found with residing in rural areas, having obstetric complications, meconium- and blood-stained amniotic fluid, and not having anti natal care visits. VL - 13 IS - 3 ER -
Department of Midwifery, College of Health Sciences, Salale University, Fiche, Ethiopia
Department of Midwifery, College of Health Sciences, Bule Hora University, Bule Hora, Ethiopia
Department of Midwifery, College of Health Sciences, Salale University, Fiche, Ethiopia
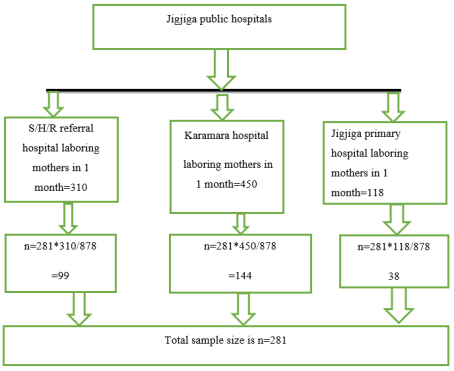
Figure 1. Schematic diagram showing the sampling technique and procedures to select a sample of 281 laboring mothers who gave birth at jigjiga public hospitals, Somalia, Ethiopia.
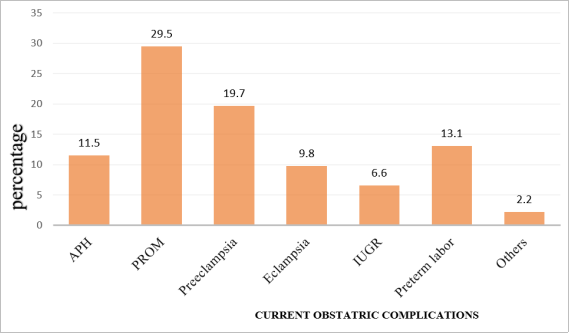
Figure 2. Current obstetrics complications among laboring mothers who gave birth at jigjiga public hospitals eastern Ethiopia, 2024.
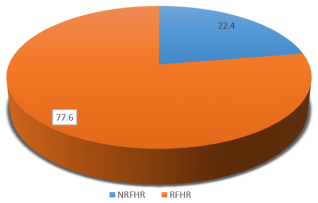
Figure 3. Magnitude of NRFHR among laboring mothers who gave birth at jigjiga public hospitals eastern Ethiopia, 2024.
Information

