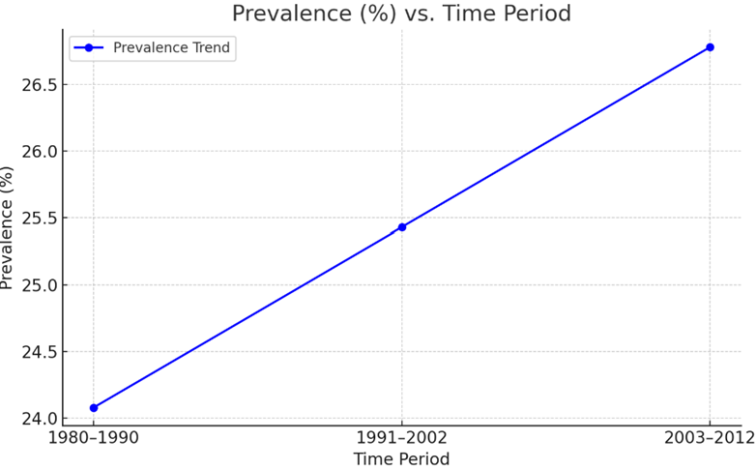
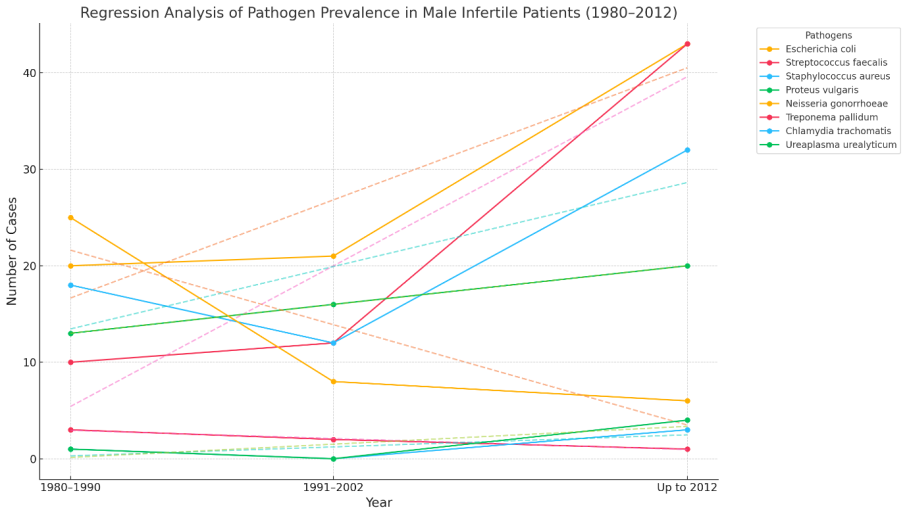
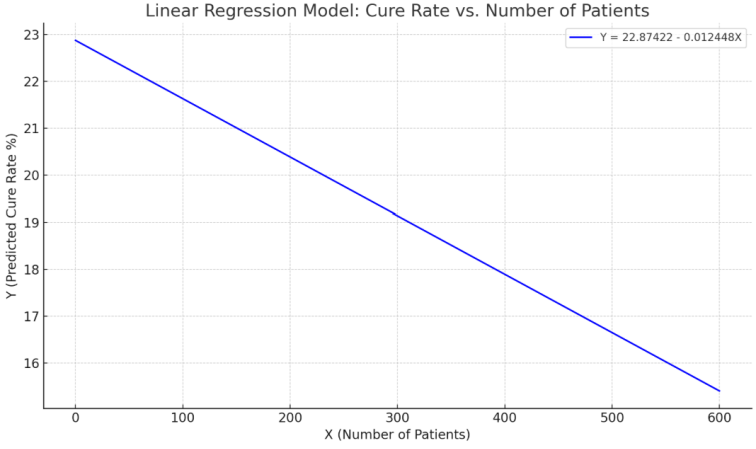
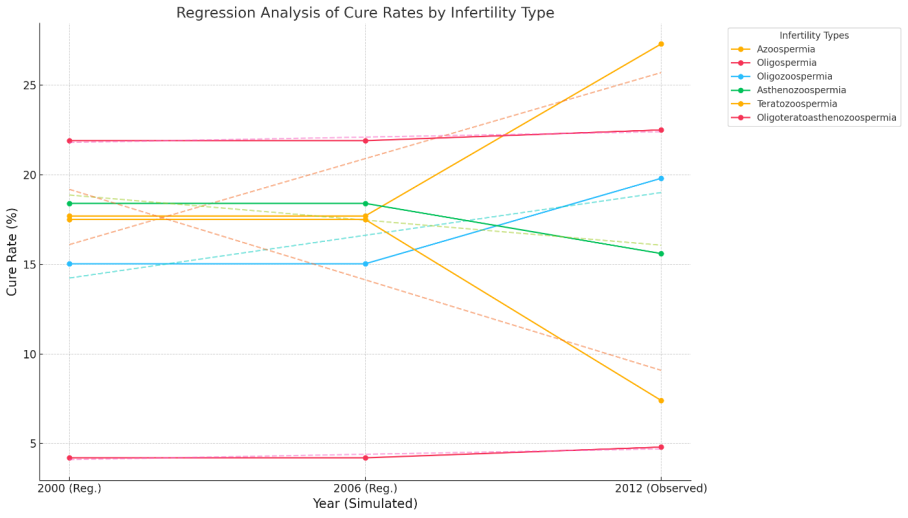
Aims: Male infertility is a multifactorial condition influenced by anatomical, hormonal, genetic and infectious causes. While advancements in diagnostics and treatments have improved outcomes, infertility remains a challenge, particularly in regions where access to specialized care is limited. Understanding both the success rates of various treatments and the etiological role of pathogens is essential for developing effective strategies. Methods and Results: This retrospective analysis examines the prevalence of urogenital pathogens isolated from male patients diagnosed with infertility across three decades: 1980-1990, 1991-2002, and 2003-2012. Bacterial and atypical pathogens were identified using standard microbiological and molecular techniques available during each respective period. Mathematical modeling, particularly through regression analysis, is a powerful tool for uncovering relationships between variables in clinical research. Patterns and quantify of different factors influence outcomes were identified, such as treatment effectiveness or disease prevalence. Regression equation was created for better predictive model that not only describes the current dataset but can also be used to estimate outcomes under different conditions. A total of 3,600 patients were e treated across various infertility types, yielding an overall cure rate of 11.5%. Azoospermia and Oligospermia showed the highest recovery rates, while Oligoteratoasthenozoospermia had the lowest. Pathogen prevalence data from 1980 to 2012 was analyzed to understand shifts in microbial contributors to infertility. The presented data revealed a decline in classic sexually transmitted infections like Neisseria gonorrhoeae and Treponema pallidum, with increasing presence of opportunistic pathogens such as Escherichia coli and Streptococcus faecalis. Azoospermia showed the highest treatment success rate, while Oligoteratoasthenozoospermia showed the lowest. The regression model captured the general trend of patient cure rates. Conclusion, significance and impact of study: The present study highlights evolving trends in pathogen prevalence among infertile male patients over 32 years. While classic sexual transmitted infectants like Neisseria gonorrhoeae have declined and opportunistic and uropathogenic bacteria like E. coli and S. faecalis have become more prominent. Outliers showed larger deviations suggesting a possible non-linearity in the real relationship using linear regression equation Y= a + bX + εi.
| Published in | World Journal of Public Health (Volume 10, Issue 4) |
| DOI | 10.11648/j.wjph.20251004.12 |
| Page(s) | 449-458 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Bacteria, Infections, Infertility, Male Infection, Treatment, Semen Analysis, Mathematical Modelling
Pathogens | No. (%) | ||
|---|---|---|---|
1980-1990 | 1991-2002 | -2012 | |
Escherichia coli | 20(22) | 21(29.6) | 43(24.7) |
Streptococcus Faecalis | 10(11) | 12(16.9) | 43(24.7) |
Staphylococcus aureus | 18(20) | 12(16.9) | 32(22.1) |
Proteus vulgaris | 13(14.3) | 16(22.5) | 20(13.8) |
Neisseria gonorrhoeae | 25(27.8) | 8(11.3) | 6(4.1) |
Treponema pallidum | 3(3.3) | 2(2.8) | 1(0.7) |
Chlamydia trachomatis | 1(1.1) | 0 | 3(2.1) |
Ureaplasma urealyticum | 1(1.1) | 0 | 4(2.8) |
Total | 91 | 71 | 152 |
Infertility Type | Patients treated | Patients cured (%) | Patients cured (%) from regression equation |
|
|---|---|---|---|---|
Azoospermia | 410 | 112 (27.3%) | 17.7% |
|
Oligospermia | 80 | 18 (22.5%) | 21.9% |
|
Oligozoospermia | 630 | 125 (19.8%) | 15.03% |
|
Astherozoospermia | 360 | 56 (15.6%) | 18.4% |
|
8 | 430 | 32 (7.4%) | 17.5% |
|
Oligoteratoasthero-zoospermia | 1500 | 72 (4.8%) | 4.2% |
|
Total | 3600 | 415 (11.5%) | 15.7% |
|
STIs | Sexual transmitted infections |
| [1] | Miyamoto, T., Tsujimura, A., Miyagawa, Y., Koh, E., Namiki, M. & Sengoku, K. (2011`). Male Infertility and Its Causes in Human. Advances in Urol olgy 2012, 1- 7. |
| [2] | Al-Jebouri, M. M. (2023). Modellings of Infectious Diseases and Cancers under Wars and Pollution Impacts in Iraq with Reference to a Novel Mathematical Model and Literature Review. Open Journal of Pathology 13 (3): 126-139. |
| [3] | Al-Jebouri, M. M. (2024). Impact of sublethal disinfectant exposure on antibiotic resistance patterns of Pseudomonas aeruginosa. Medical Principles and Practice 13: 1-9. |
| [4] | Ugwuja, E.., Ugwu, N. C., & Ejikeme, B. N. (2008). Prevalence of Low Sperm Count and Abnormal Semen Parameters in Male Partners of Women Consulting at Infertility Clinic in Abakaliki, Nigeria. African Reproductive Health 12, 67-73. |
| [5] | Schmidt, L., Minister, K.,& Helm, P. (1995) Infertility and the seeking of infertility treatment in a representative population. Britain Journal Obstetics and Gynaecology 102, 978-984. |
| [6] | Apari, P., de Sousa, J. D., & Müller, V. (2014). Why sexually transmitted infections tend to cause infertility: An evolutionary hypothesis. PLoS Pathogens 10: e1004111. |
| [7] | Ikechebelu, J. I., Adinma, J. I., Orie, E. F., & Ikegwonu, S. O. (2003). High prevalence of male infertility in South-eastern Nigeria. Journal of Obstetics and Gynaecolology 23: 657-659. |
| [8] | Larsen, U. (2000). Primary and secondary infertility in sub-Saharan Africa. International Journal of Epidemiology 29, 285-291. |
| [9] | Okonofua, F. E. (2003). Infertility in Sub-Saharan Africa. In: Okonofua F, and L Odunsi, eds. Contemporary Obstetrics and Gynaecology for Developing Countries. Women’s Health and Action Research Centre, 128-156. |
| [10] | Agyei-Mensah, S. (1996). New perspective on the fertility situation in Sub-Saharan Africa NorskGeografiskTidsskrift - Norwegian Journal of Geography 50: 101 - 112. |
| [11] | Tahmasbpour, E., Balasubramanian, D., & Agarwal, A. (2014). A multi‑faceted approach to understanding male infertility: gene mutations, molecular defects and assisted reproductive techniques (ART). Journal of Assisted Reproduction and Genetics 31(9), 1115-1137. |
| [12] | Stormont, G. D., & Deibert, C. M. (2021). Genetic causes and management of male infertility. Translational Andrology and Urology 10(3), 1365-1372. |
| [13] | Salonia, A., Bettocchi, C., Boeri, L., Capogrosso, P., Carvalho, J., Cilesiz, N. C.,& Fijak, M. (2023). Infections and inflammation as etiological factors in male infertility. Human Reproduction Update 24(5), 416-440. |
| [14] | Guiton, R., & Drevet, J. R. (2023). Viruses, bacteria and parasites: infection of the male genital tract and fertility. Basic and Clinical Andrology, 33, Article 19. Springer. |
| [15] | Henkel, R. (2021). The role of infections and leukocytes in male infertility. Andrology 9(4), 101-116. |
| [16] | Vynnycky, E. & White, R. (2010). An Introduction to Infectious Disease Modelling. Oxford University Press, Oxford. 282-315. |
| [17] | Garnett, G. P., Swinton, J., Brunham, R. C. & Anderson, R. M. (1992). Gonococcal infection, infertility, and population growth: II. The influence of heterogeneity in sexual behaviour. IMA Journal of Mathematics and Applied Medical Biology 9(2), 127-144. |
| [18] | White, R. G., Orroth, K. K., Glynn, J. R., Freeman, E. E., Bakker, R., Habbema, J. D. F., et al. (2008). Treating curable sexually transmitted infections to prevent HIV in Africa: still an effective control strategy? Journal of Aquired Immune Deficiency Syndrome 47, 940-946. |
| [19] | Hethcote, H. W. (1976). Qualitative analysis for communicable disease models. Mathematical Biosciences 28: 335-356. |
| [20] | WHO Laboratory Manual for the Examination of Human Semen and Sperm-Cervical Mucus Interaction. 4th edition, Geneva, World Health Organization., 1999. |
| [21] | Cowan and Steel's Manual for Identification of Medical Bacteria. Edited by G. I. Barrow, R. K. A. Feltham, cambridge University Press, 2009. |
| [22] | Samli H, Samli MM, Solak M., & Imirzalioglu, N. (2006). Genetic anomalies detected in patients with non-obstructive azoospermia and oligozoospermia. Archives of Androlology 52.263-267. |
| [23] | Abarikwu, S. O. (2013). Causes and Risk Factors for Male-Factor Infertility in Nigeria: A Review of African Journal of Reproductive Health 17(4), 150-166. |
| [24] | Okonofua, E. F., Harris, D., Odebiyi, A., Kane, T. & Snow, R. (1997). The social meaning of infertility in Southwest Nigeria. Health Transformation Review 7, 205-220. |
| [25] | Nwabuisi, C. & Onile, B. A. (2001). Male infertility among sexually transmitted diseases clinic attendees in Ilorin, Nigeria. Nigerian Journal of Medicine 10: 68-71. |
| [26] | Sule-Odu, A. O., Oladapo, O. T., Jagun, O. E., & Awosile, J. (2005). Microbial isolates and HIV infection in couples attending fertility clinics in Sagamu, Nigerian Journal of Obstetics and Gynaecology 25, 685-688. |
| [27] | Esimai, O. A., Orji, E. O., & Lasisi, A. R. (2002). Male contribution to infertility in Ile-Ife, Nigeria. Nigerian Journal of Medicine 11, 70-72. |
| [28] | Obiechina, N. J., Okoye, R. N., & Emelife, E. C. (2002). Seminal fluid indices of men attending infertility clinic at St. Charles Borromeo Hospital, Onitsha, Nigeria (1994-1998). Nigerian Journal of Medicine 11, 20-22. |
| [29] | Ekwere, P. D. (2004). Profile of sub-fertile Nigerian men in an infertility Clinic in Calabar, Nigeria. Nigerian Journal of Surgery 10, 37-42. |
| [30] | Agbakoba NR, Adetosoye AI, & Ikechebelu JI. (2007). Genital mycoplasmas in semen samples of males attending a tertiary care hospital in Nigeria: any role in sperm count reduction? Nigerian Journal of Clinical Practice 10: 169-173. |
| [31] | Huang, J., Tian, Y., Xu, X., & Wang, Y. (2015). Mycoplasma and Ureaplasma infection and male infertility: A systematic review and meta‑analysis. Andrology 3(6), 1121-1130. |
| [32] | Maisey, K., Nardocci, G., Imarai, M., Cardenas, H., Rios, M., Croxatto, H. B., et al. (2003). Expression of S150-161. Proinflammatory cytokines and receptors by human fallopian tubes in organ culture following challenge with Neisseria gonorrhoeae. Infection and Immunity 71: 527-32. |
| [33] | Malhotra, M., Sood, S., Mukherjee, A., Muralidhar, S., & Bala, M. (2013). Genital Chlamydia trachomatis: An update. Indian Journal of Medical Research 138: 303-16. |
| [34] | Turner, K. M., Garnett, G. P., Ghani, A. C., Sterne, J. A., & Low N. (2004). Investigating ethnic inequalities in the incidence of sexually transmitted infections: mathematical modelling study. Sex Transformation Infection 80(5): 379-385. |
| [35] | Zeighami, H., Peerayeh, S. N., Yazdi, R. S., & Sorouri, R. (2009). Prevalence of Ureaplasma urealyticum and Ureaplasma parvum in semen of infertile and healthy men. International Journal of Sexual Transmitted Diseases & AIDS, 20(6), 387-390. |
| [36] | Pai, M. O., Venkatesh, S.,& Gupta, P. (2020). The role of infections in infertility: A review. International Journal of Academic Medicine 6(3), 189-196. |
| [37] | Ruggeri, M., Cannas, S., Cubeddu, M., Molicotti, P., Piras, G. L., Dessole, S., et al. (2016). Bacterial agents as a cause of infertility in humans. New Microbiology 39: 206-209. |
| [38] | Mascarenhas, M. N., Flaxman, S. R., Boerma, T., Vanderpoel, S.,& Stevens, G. A. (2012). National, regional, and global trends in infertility prevalence since 1990: A systematic analysis of 277 health surveys. PLoS of Medicine 9, e1001356. |
| [39] | Kamath, M. S., & Deepti MK. (2016). Unexplained infertility: An approach to diagnosis and management. Current Medical Issues 14, 94-100. |
APA Style
Al-Jebouri, M. M., Kaki, M. N. M. (2025). Mathematical Considerations for the Infectious Infertility of Male in Iraq. World Journal of Public Health, 10(4), 449-458. https://doi.org/10.11648/j.wjph.20251004.12
ACS Style
Al-Jebouri, M. M.; Kaki, M. N. M. Mathematical Considerations for the Infectious Infertility of Male in Iraq. World J. Public Health 2025, 10(4), 449-458. doi: 10.11648/j.wjph.20251004.12
@article{10.11648/j.wjph.20251004.12,
author = {Mohemid Maddallah Al-Jebouri and Mohammed Nokhas Murad Kaki},
title = {Mathematical Considerations for the Infectious Infertility of Male in Iraq
},
journal = {World Journal of Public Health},
volume = {10},
number = {4},
pages = {449-458},
doi = {10.11648/j.wjph.20251004.12},
url = {https://doi.org/10.11648/j.wjph.20251004.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251004.12},
abstract = {Aims: Male infertility is a multifactorial condition influenced by anatomical, hormonal, genetic and infectious causes. While advancements in diagnostics and treatments have improved outcomes, infertility remains a challenge, particularly in regions where access to specialized care is limited. Understanding both the success rates of various treatments and the etiological role of pathogens is essential for developing effective strategies. Methods and Results: This retrospective analysis examines the prevalence of urogenital pathogens isolated from male patients diagnosed with infertility across three decades: 1980-1990, 1991-2002, and 2003-2012. Bacterial and atypical pathogens were identified using standard microbiological and molecular techniques available during each respective period. Mathematical modeling, particularly through regression analysis, is a powerful tool for uncovering relationships between variables in clinical research. Patterns and quantify of different factors influence outcomes were identified, such as treatment effectiveness or disease prevalence. Regression equation was created for better predictive model that not only describes the current dataset but can also be used to estimate outcomes under different conditions. A total of 3,600 patients were e treated across various infertility types, yielding an overall cure rate of 11.5%. Azoospermia and Oligospermia showed the highest recovery rates, while Oligoteratoasthenozoospermia had the lowest. Pathogen prevalence data from 1980 to 2012 was analyzed to understand shifts in microbial contributors to infertility. The presented data revealed a decline in classic sexually transmitted infections like Neisseria gonorrhoeae and Treponema pallidum, with increasing presence of opportunistic pathogens such as Escherichia coli and Streptococcus faecalis. Azoospermia showed the highest treatment success rate, while Oligoteratoasthenozoospermia showed the lowest. The regression model captured the general trend of patient cure rates. Conclusion, significance and impact of study: The present study highlights evolving trends in pathogen prevalence among infertile male patients over 32 years. While classic sexual transmitted infectants like Neisseria gonorrhoeae have declined and opportunistic and uropathogenic bacteria like E. coli and S. faecalis have become more prominent. Outliers showed larger deviations suggesting a possible non-linearity in the real relationship using linear regression equation Y= a + bX + εi.
},
year = {2025}
}
TY - JOUR T1 - Mathematical Considerations for the Infectious Infertility of Male in Iraq AU - Mohemid Maddallah Al-Jebouri AU - Mohammed Nokhas Murad Kaki Y1 - 2025/09/25 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251004.12 DO - 10.11648/j.wjph.20251004.12 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 449 EP - 458 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251004.12 AB - Aims: Male infertility is a multifactorial condition influenced by anatomical, hormonal, genetic and infectious causes. While advancements in diagnostics and treatments have improved outcomes, infertility remains a challenge, particularly in regions where access to specialized care is limited. Understanding both the success rates of various treatments and the etiological role of pathogens is essential for developing effective strategies. Methods and Results: This retrospective analysis examines the prevalence of urogenital pathogens isolated from male patients diagnosed with infertility across three decades: 1980-1990, 1991-2002, and 2003-2012. Bacterial and atypical pathogens were identified using standard microbiological and molecular techniques available during each respective period. Mathematical modeling, particularly through regression analysis, is a powerful tool for uncovering relationships between variables in clinical research. Patterns and quantify of different factors influence outcomes were identified, such as treatment effectiveness or disease prevalence. Regression equation was created for better predictive model that not only describes the current dataset but can also be used to estimate outcomes under different conditions. A total of 3,600 patients were e treated across various infertility types, yielding an overall cure rate of 11.5%. Azoospermia and Oligospermia showed the highest recovery rates, while Oligoteratoasthenozoospermia had the lowest. Pathogen prevalence data from 1980 to 2012 was analyzed to understand shifts in microbial contributors to infertility. The presented data revealed a decline in classic sexually transmitted infections like Neisseria gonorrhoeae and Treponema pallidum, with increasing presence of opportunistic pathogens such as Escherichia coli and Streptococcus faecalis. Azoospermia showed the highest treatment success rate, while Oligoteratoasthenozoospermia showed the lowest. The regression model captured the general trend of patient cure rates. Conclusion, significance and impact of study: The present study highlights evolving trends in pathogen prevalence among infertile male patients over 32 years. While classic sexual transmitted infectants like Neisseria gonorrhoeae have declined and opportunistic and uropathogenic bacteria like E. coli and S. faecalis have become more prominent. Outliers showed larger deviations suggesting a possible non-linearity in the real relationship using linear regression equation Y= a + bX + εi. VL - 10 IS - 4 ER -
Department of Medical Laboratory Technology, Al-Qalam University College, Kirkuk, Iraq
Civil Engineering Department, Al-Qalam University College, Kirkuk, Iraq
Information