Abstract
Background: Self-medication (SM) is defined by the World Health Organization (WHO) as the self-administration of medication without a valid prescription or without consulting a healthcare professional. This study aims to examine the Prevalence of self-medication and the associated factors in Ado-Odo-Ota Ogun state Nigeria Methods: The study utilised a descriptive cross-sectional study that used a questionnaire to elicit responses from residents of Ado-Odo Ota Local Government Area (LGA). The study employed a multi-stage sampling approach, and data were analysed using IBM-Statistical Package for Social Sciences (IBM-SPSS) version 28.0. Results: The prevalence of self-medication in Ado Odo Ota over the past year was 78.4%. About 51.6% of respondents reported self-medicating occasionally, with 24.8% doing so within the last week. Previous prescriptions were the most common source of drug information (40.2%), while big pharmacies were the primary source of drugs. The majority (54.2%) self-medicated because they perceived their illnesses as minor and not requiring a doctor’s attention. Drug selection was mainly based on symptoms (51.9%). The leading reasons for self-medication included financial constraints, with lack of money to pay hospital bills (mean = 4.81 ± 0.7) and the high cost of treatment and tests (mean = 4.64 ± 0.89) strongly influencing this behavior. Conclusion: These findings underscore the need for improved access to healthcare facilities in rural areas and increase awareness about the potential risks and limitations of self-medication.
Keywords
Prevalence, Self-medication, Drugs, Prescription
1. Introduction
Self-medication (SM), as defined by the World Health Organization (WHO), refers to the use of medications without a valid prescription or consultation with a healthcare professional
| [1] | Aqeel T, Shabbir A, Basharat H, Bukhari M, Mobin S, Shahid H, et al. Prevalence of self-medication among urban and rural population of Islamabad, Pakistan. Trop J Pharm Res 2014; 13: 627-33. https://doi.org/10.4314/tjpr.v13i4.22 |
| [2] | Eticha, T., & Mesfin K. Self-Medication practices in Mekelle, Ethiopia. Plos One, 9(5), 1-5 2014. |
| [3] | Oyediran OO, Ayandiran EO, Olatubi MI, Olabode O. Awareness of risks associated with Self-medication among Patients attending General Out-patient Department of a Tertiary Hospital in South Western Nigeria. Int J Africa Nurs Sci 2019; 10: 110-5. https://doi.org/10.1016/j.ijans.2019.03.001 |
| [4] | Akande-Sholabi W, Ajamu AT, Adisa R. Prevalence, knowledge and perception of self-medication practice among undergraduate healthcare students. J Pharm Policy Pract 2021; 14: 1-11. https://doi.org/10.1186/s40545-021-00331-w |
[1-4]
. This is a widespread practice in many developing countries as well as some developed ones, involving both over-the-counter (OTC) and prescription drugs, including antibiotics
| [5] | Shaghaghi A, Asadi M, Allahverdipour H. Predictors of self-medication behavior: A systematic review. Iran J Public Health 2014; 43: 136-46. |
[5]
. Many factors have been identified as motivating factors for people to engage in self-medication practices in developing countries, including a lack of medical insurance, high costs of hospital visits and consultations, easy public access to prescribed medications, recommendations from friends, low cost of the practice, and previous experience among others
| [5] | Shaghaghi A, Asadi M, Allahverdipour H. Predictors of self-medication behavior: A systematic review. Iran J Public Health 2014; 43: 136-46. |
| [6] | Lukovic JA, Miletic V, Pekmezovic T, Trajkovic G, Ratkovic N, Aleksic D, et al. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS One 2014; 9. https://doi.org/10.1371/journal.pone.0114644 |
[5, 6]
.
SM is commonly used to treat minor ailments such as headaches, fevers, sore throats, gastrointestinal tract difficulties, respiratory problems, skin diseases, and ear complaints among others
| [7] | Babatunde OA, Fadare JO, Ojo OJ, Durowade KA, Atoyebi OA, Ajayi PO, et al. Self-medication among health workers in a tertiary institution in South-West Nigeria. Pan Afr Med J 2016; 24. https://doi.org/10.11604/pamj.2016.24.312.8146 |
| [8] | Gelayee DA. Self-Medication Pattern among Social Science University Students in Northwest Ethiopia. J Pharm 2017; 2017: 1-5. https://doi.org/10.1155/2017/8680714 |
| [9] | Kumar N, Kanchan T, Unnikrishnan B, Rekha T, Mithra P, Kulkarni V, et al. Perceptions and Practices of Self-Medication among Medical Students in Coastal South India. PLoS One 2013; 8. https://doi.org/10.1371/journal.pone.0072247 |
| [10] | Helal RM, Abou-Elwafa HS. Self-medication in university students from the city of mansoura, Egypt. J Environ Public Health 2017; 2017. https://doi.org/10.1155/2017/9145193 |
| [11] | Ahmadi SM, Jamshidi K, Sadeghi K, Abdi A, Vahid MP. The prevalence and affecting factors on self-medication among students of Kermanshah University of Medical Science in 2014. J Clin Diagnostic Res 2016; 10: IC01-4. https://doi.org/10.7860/JCDR/2016/18018.7847 |
[7-11]
. Aside from its uses, self-medication may also provide several benefits to patients, including rapid access to treatment, self-reliance in alleviating symptoms, cost savings and decreased frequency of visits to health centres. It may also benefit the community by conserving medical resources, reducing absenteeism from work, relieving pressure on medical services, and providing additional time for critical conditions
]. Despite its numerous benefits, self-medication, particularly when unguided, may pose potential hazards at the individual level, including inaccurate diagnosis, significant adverse effects, increasing antibiotic resistance, harmful food and drug interactions, and drug misuse and addiction. According to Bennadi et al.
| [12] | Bennadi D. Self-medication: A current challenge. J Basic Clin Pharmacy, 5(1), 19 2014. |
[12]
unguided self-medication may also contribute to a rise in drug-induced disease and public expenditures at the community level.
The negative implications of SM are felt primarily on many developing countries with inadequate resources, low literacy levels, poverty, and restricted access to healthcare, as well as among a vast population that lacks adequate knowledge about therapy, dosage and duration of usage, and side effects
| [13] | Chouhan K, Prasad SB. Self-medication and their consequences: A challenge to health professional. Asian J Pharm Clin Res 2016; 9: 314-7. |
| [14] | Uzochukwu BSC, Onwujekwe OE, Okwuosa C, Ibe OP. Patent medicine dealers and irrational use of medicines in children: The economic cost and implications for reducing childhood mortality in southeast Nigeria. PLoS One 2014; 9. https://doi.org/10.1371/journal.pone.0091667 |
[13, 14]
. In Nigeria, for example, roadside hawkers and various unregistered and registered proprietary and patent medicine vendors frequently sell both OTC and prescription-only medicine, owing mainly to a lack of enforcement of drug regulations
| [15] | Erhun WO, Babalola OO, M. O. MO. Drug Regulation and Control in Nigeria: the Challenge of Counterfeit Drugs. World Health Popul 2013; 4. https://doi.org/10.12927/whp.17597 |
| [16] | Wabe N, Ahmed D, Angamo M. Self-Medication with Antibiotics and Antimalarials in the Community of Silte Zone, South Ethiopia. TAF Prev Med Bull 2012; 11: 529. https://doi.org/10.5455/pmb.1-1314892446 |
[15, 16]
. The unregulated sales of these products may incessantly trigger self-medication practices among the general populace.
Moreover, there has been a growing trend in self-medication across several countries, driven by factors such as economic challenges, lifestyle changes, increased access to medications, greater confidence in managing minor illnesses independently, and the wider availability of medical products. In many low-income nations like Nigeria, numerous medications can be obtained over the counter (OTC), and self-medication accounts for an estimated 60% to 80% of health issues, as it is often viewed as a more affordable healthcare option
| [17] | Bassi PU, Osakwe AI, Builders M, Ettebong E, Kola G, Oreagbai I. Prevalence and Determinants of Self-Medication Practices among Nigerians 2021; 34: 634-49. |
| [18] | Gbadebo AM, Taiwo AM, Ayedun H, Adeola AJ. Geochemical analysis of groundwater quality in Agbara and environs. Appl Ecol Environ Res 2012; 10: 375-84. https://doi.org/10.15666/aeer/1003_375384 |
[17, 18]
.
Recent national and regional studies show differing self-medication rates, but there is limited up-to-date, community-specific data from semi-urban and peri-urban industrial areas like Ado-Odo/Ota in Ogun State. This research is important as it addresses a key research gap by providing localized insights into how socio-economic factors, healthcare access, and personal beliefs drive self-medication, to guide targeted interventions and policies. Therefore, this study aims to examine the Prevalence of self-medication and the associated factors in Ado-Odo-Ota Ogun state Nigeria.
2. Methods
2.1. Study Design
This study employed a descriptive cross-sectional design to assess the prevalence and associated factors of self-medication among residents of Ado-Odo Ota Local Government Area (LGA) in Ogun State, Nigeria (
Figure 1). A structured, interviewer-administered questionnaire was used to collect data from participants. A cross-sectional descriptive approach was employed in this study, as it enabled the researcher to collect essential data in line with the study objectives.
2.2. Study Area
Figure 1. Map of Ogun State showing Ado-Odo Ota LGA.
This research was conducted in Ado Odo Ota, one of Ogun State's 19 local government areas. It shares a border with metropolitan Lagos State, and it is the second-largest LGA in Ogun State, with its headquarters at Ota (or Otta), which is located at 6°41'00" N 3°41'00" E to the north of the area. Ado Odo Ota LGA has several towns and cities, including Ado-Odo, Agbara, Iju-Ota, Igbesa, Itele, Kooko Ebiye Town, Owode, and the popular Sango Ota, which borders the Lagos metropolitan area, among others. Ado-Odo/Ota is the state's most populous industrial area with the greatest number of factories.
2.3. Study Population
The target population comprises all selected participants who reside within the Ado-Odo Ota Local Government Area. The study did not exclude any participants based on their level of education, ethnicity, complexion, or socio-economic status.
2.4. Inclusion Criteria
All selected respondents living in Ado-Odo Ota LGA and were willing to participate in the study were included in this research.
2.5. Exclusion Criteria
All respondents who were not selected, those who do not reside in Ado-Odo-Ota, and those who were unwilling to participate in the study were excluded from this research.
2.6. Sampling Technique
The study employed a multi-stage sampling approach. In the first stage, stratification was carried out by dividing Ado-Odo Ota LGA into its sixteen administrative wards to ensure geographic representation. In the second stage, within each ward, a quota-based random walk method was used to approach households according to predefined demographic quotas (e.g., age, gender) to enhance diversity and representation
| [20] | Omolase CO, Adeleke OE, Afolabi AO AO. Self-medication among General Outpatient in Nigerian community hospital. Annu J Postgrad Med 2007; 5 64-6 2007. |
[20]
. This combination allowed for both structured stratification at the LGA level and controlled household selection within wards, aligning with the study’s representativeness objectives.
2.7. Sample Size
The Prevalence of self-medication used for the sample size for this study was adapted from Omolase et al.
on self-medication amongst general out-patients in a Nigerian community hospital.
Where z = 1.96
P = Prevalence of self-medication amongst general out-patients in Nigeria community hospitals = 85%. P = 0.85; 1-p = 1-0.85 = 0.15; d = marginal error = 0.05
= = 195.92 = 196. 10% attrition = 196 + 10% of 196 = 196+20 = 216
Although the calculated minimum sample size was 216, the final number of respondents included in the study was 273. This adjustment was due to field conditions inherent in the quota-based random walk approach, where interviewers continued data collection to meet demographic and geographic representation targets across all wards. The extended sample improved the balance across subgroups and enhanced the representativeness of the study within the limitations of a non-probability sampling method.
2.8. Data Collection Instrument
In order to collect information from the respondents, structured questionnaires were utilised. This strategy technique involves categorising population participants into wards. A structured questionnaire was translated into the Yoruba language, widely spoken in this country region, and was used to gather information from all participants. Respondents were interviewed to ascertain their prevalence and factors associated with self-medication. Respondents' background information, such as age, residence, religion, and educational background, was obtained.
2.9. Data Collection in the Field and Analysis
The questionnaires were provided to the investigators daily, after the number of households in the selected villages had been updated according to the quotas. To comply with COVID-19 safety protocols, were administered after obtaining informed consent and collected the following day, ensuring participation from both literate and illiterate residents. This approach ensured that the study was accessible to educated and uneducated respondents. This approach was adopted because an online survey would accommodate the bias of showing learned viewpoints while excluding the illiterates, who would not reflect the general public's opinion.
The completed questionnaires were coded, and all entries were checked for completeness. Missing data were excluded from the final analysis using pairwise deletion to maximize the use of available responses for each variable. Data were analysed using IBM Statistical Package for Social Sciences (IBM-SPSS) version 28.0. Only descriptive statistical analyses were performed, including frequencies, percentages, means, and standard deviations. No inferential statistical tests were conducted for this study. The internal consistency of the 11-item scale assessing factors influencing self-medication was evaluated using Cronbach’s alpha, which produced a value of 0.84.
2.10. Ethical Considerations
Ethical approval for this study was obtained from the National Health Research Ethics Committee of Nigeria (Approval number: NHREC/01/01/2007/-21/04/2023). The Ado-Odo Ota Local Government Authority also granted approval. Participation was voluntary, with informed consent obtained from all respondents. Data were anonymized and kept strictly confidential and sused solely for research purposes.
3. Results
3.1. Prevalence of Self-medication Among Respondents of Ado-Odo Ota Ogun State
Table 1 presents the sociodemographic profiles of the study respondents, with females comprising 56.4% (154) and males accounting for 43.2% (118). The largest age group was 20-29 years (34.4%), followed by 30-39 years (26.4%) and 40-49 years (17.6%). The remaining age groups (15-19, 50-59, and 60+) ranged from 4.8% to 8.8%. Most respondents were Christians (72.9%), while 27.1% identified as Muslim. In terms of marital status, 53.1% were married, 44.3% single, and 2.6% separated, divorced, or widowed. Most participants had at least a secondary education, with 42.9% attaining higher education and 39.2% completing secondary school. Only 11.0% had primary education, and 7.0% had none. Regarding employment, 66.7% were self-employed or ran personal businesses, 22.0% worked in private companies, 7.0% were government employees, and 4.0% were unemployed or students. Monthly income varied, with 46.9% earning between 21,000-50,000 units, 25.3% earning 20,000 or less, 18.7% earning 51,000-100,000, and 5.9% earning above 100,000 units.
Table 1. Demographic profiles of the study respondents.
Variables | Parameter | Frequency (n = 273) | Percentage |
Gender | Male | 118 | 43.2 |
Female | 154 | 56.4 |
Age Category (years) | 15-19 | 22 | 8.1 |
20-29 | 94 | 34.4 |
30-39 | 72 | 26.4 |
40-49 | 48 | 17.6 |
50-59 | 24 | 8.8 |
60 and above | 13 | 4.8 |
Religion | Christianity | 199 | 72.9 |
Islam | 74 | 27.1 |
Marital status | Single | 121 | 44.3 |
Married | 145 | 53.1 |
Separated/ divorced/ widowed | 7 | 2.6 |
Education | Higher | 117 | 42.9 |
Secondary | 107 | 39.2 |
primary | 30 | 11.0 |
No formal education | 19 | 7.0 |
Work | Government worker | 19 | 7.0 |
Private company | 60 | 22.0 |
Personal business/self-employed | 182 | 66.7 |
Unemployed/ students | 11 | 4.0 |
Monthly income | 20,000 | 69 | 25.3 |
21,000-50,000 | 128 | 46.9 |
51,000-100,000 | 51 | 18.7 |
> 100,000 | 16 | 5.9 |
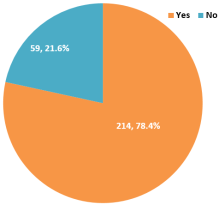
3.2. Prevalence of Self-medication in Ado Odo Ota in the Past Year
The Prevalence of self-medication in the last year was 78.4% compared to 21.6% who took drugs only on prescribed. (
Figure 2).
Figure 2. Prevalence of self-medication in Ado Odo Ota in the past year.
3.3. Self-medication Practices and Drug Information Sources Among Respondents
The self-medication practices and drug information sources among respondents were assessed in
Table 2. Over half of the respondents (51.6%) reported self-medicating sometimes, while 23.0% admitted to always self-medicating. Only a quarter (25.4%) did so rarely or occasionally. When asked about the recency of their last self-medication, nearly a quarter (24.8%) had done so less than a week ago, and another 23.8% reported doing so a month ago. Additionally, 17.8% had self-medicated within the past two weeks, while 21.0% reported doing so over three months ago. In terms of sources of information used for self-medicating, the majority relied on previous prescriptions (40.2%) or their own personal knowledge (29.4%). Others turned to friends (23.4%) or family members (12.1%). A smaller proportion was influenced by advertisements (7.9%) or other sources (1.4%). Big pharmacies were the most common source of drugs for self-medication, used by 67.8% of respondents, while 43.5% obtained their medications from local medicine shops. Fewer participants got drugs from friends (13.1%), commercial bus sellers (7.5%), or hawkers (1.4%). When it came to choosing which drugs to use, more than half of the respondents (51.9%) made their decisions based on self-assessment of their symptoms. Others relied on advice from medicine shop owners (35.5%), suggestions from people around them (22.9%), or consultations with auxiliary nurses (20.1%).
Table 2. Self-Medication Practices and Drug Information Sources Among Respondents.
Variable | Frequency (n) | Percentage (%) |
Frequency of Self-Medication (n=287) |
Sometimes | 148 | 51.6 |
Once in a while / Rarely | 73 | 25.4 |
Always | 66 | 23.0 |
Last Self-Medication (n=214) |
Less than a week ago | 53 | 24.8 |
A month ago | 51 | 23.8 |
1-2 weeks ago | 38 | 17.8 |
1-3 months ago | 26 | 12.1 |
Over 3 months ago | 45 | 21.0 |
Source of Drug Info (n=287) |
Previous prescription | 115 | 40.2 |
Personal knowledge | 84 | 29.4 |
Friends | 67 | 23.4 |
Family members | 35 | 12.1 |
Advertisements | 23 | 7.9 |
Others | 4 | 1.4 |
Source of Drugs (n=287) |
Big pharmacy | 195 | 67.8 |
Local medicine shop | 125 | 43.5 |
Friends | 38 | 13.1 |
Commercial bus sellers | 22 | 7.5 |
Hawkers | 4 | 1.4 |
Drug Choice Method (n=287) |
Based on symptoms (self-judgment) | 149 | 51.9 |
Medicine shop owners’ advice | 102 | 35.5 |
Suggestions from people around | 66 | 22.9 |
Consulted auxiliary nurse | 58 | 20.1 |
3.4. Reasons for Self-medication
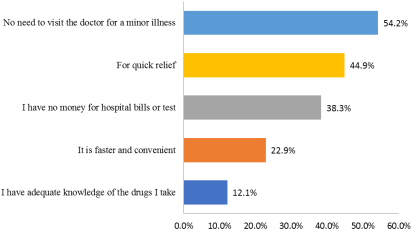
Figure 3 highlights the key reasons behind self-medication among participants. The most common reason, cited by 54.2%, was the belief that visiting a doctor for minor illnesses is unnecessary. Financial constraints were also a major factor, with 38.3% reporting they couldn't afford hospital bills or medical tests. Many participants (44.9%) said they self-medicated to get quick relief from symptoms, while 22.9% preferred it for the convenience and speed. A smaller group (12.1%) felt confident enough in their knowledge of medications to manage treatment on their own.
Figure 3. Reasons for self-medication. Reasons for self-medication.
3.5. Factors Influencing Self-medication
Respondents moderately agreed that long distances to hospitals (mean = 3.67 ± 1.68) and the lack of hospital access (3.85 ± 1.63) could drive self-medication. They strongly agreed that the high cost of treatment and tests (4.64 ± 0.89) and the inability to pay hospital bills (4.81 ± 0.70) were major contributing factors. The unavailability of hospitals (3.85 ± 1.53), lack of drugs (3.81 ± 1.56), and insufficient health workers (3.72 ± 1.61) also received moderate agreement. Lack of health insurance (4.14 ± 1.26) and insufficient information on the dangers of self-medication (4.06 ± 1.41) were seen as significant factors. Participants also noted that a poor economy and low standard of living (4.57 ± 1.06), as well as the absence of policies regulating self-medication (3.64 ± 1.62), contribute to the practice. The factors influencing self-medication were derived from participants’ responses on an 11-item scale measured using a five-point Likert scale (1 = Strongly Disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly Agree).
Table 3. Factors influencing self-medication.
SN | Factors | Overall (n = 273) |
1 | Long-distance to Hospitals can cause self-medication | 3.67 ± 1.68 |
2 | Lack of access to hospitals can cause self-medication | 3.85 ± 1.63 |
3 | High costs of healthcare services/treatment and test costs can cause self-medication | 4.64 ± 0.89 |
4 | Non-availability of hospitals can cause self-medication | 3.85 ± 1.53 |
5 | Lack of drugs in hospitals can cause self-medication | 3.81 ± 1.56 |
6 | Lack of sufficient health workers in hospitals can cause self-medication | 3.72 ± 1.61 |
7 | Lack of health insurance can cause self-medication | 4.14 ± 1.26 |
8 | The lack of policies regulating self-medication can cause self-medication | 3.64 ± 1.62 |
9 | Poor economy and standard of living in this country can cause self-medication | 4.57 ± 1.06 |
10 | Lack of money to pay hospital bills can cause self-medication | 4.81 ± 0.7 |
11 | Insufficient information about the dangers of self-medication can make one engage in self-medication | 4.06 ± 1.41 |
4. Discussion
Based on the findings from this study, a significant proportion of participants (78%) were self-medicating. This shows that self-medication is on the high side. The finding from this study was similar to the findings of previous studies in Nigeria by Bassi et al.
| [17] | Bassi PU, Osakwe AI, Builders M, Ettebong E, Kola G, Oreagbai I. Prevalence and Determinants of Self-Medication Practices among Nigerians 2021; 34: 634-49. |
[17]
69.4%, Yusuff & Omarusehe
63.8% and Afolabi et al.
85%, all of which reported high prevalence rates of self-medication. When compared to the findings from other countries in Africa, the findings of this study were consistent with studies by Teke and Suh
(86.50%) in Cameroon Awad and Capps
81.8% in Khartoum State Sudan,
. The possible reason for this could be that healthcare facilities are scarce, especially in rural areas, and people often have to travel long distances to access medical care. As a result, individuals may resort to self-medication as a more convenient and immediate solution to their health
| [25] | Abrha S, Molla F, Melkam W. Self-medication Practice : the Case of Kolladiba Town, North West Ethiopia. Int J Pharma Sci Res 2014; 5: 670-7. |
| [26] | Abdallah, Salisu & Vanessa P. HEALTH CARE IN GHANA: A Report of the Austrian Centre for Country of Origin & Asylum Research and Development 2009. |
[25, 26]
. The similarities between this study and previous literature may be due to common socio-economic and healthcare system constraints in low- and middle-income settings, where high poverty rates, inadequate health insurance coverage, and weak enforcement of drug regulations create an environment conducive to self-medication. The high reliance on self-medication warrant the urgent need to strengthen healthcare accessibility, particularly in rural and peri-urban areas, and to implement public education campaigns on the potential risks of unguided medication use. ss.
Most participants reported self-medicating occasionally (51.4%), while 25.2% did so rarely and 22.9% always self-medicated. Also, this study's findings show that most respondents reported self-medicating within a relatively short timeframe. These findings indicate that a substantial proportion of self-medication instances among the participants are relatively recent, suggesting an ongoing reliance on self-medication for healthcare needs. These results align with the findings of Chautrakarn and Phutrakool
| [27] | Chautrakarn S, Khumros W, Phutrakool P. Self-Medication With Over-the-counter Medicines Among the Working Age Population in Metropolitan Areas of Thailand. Front Pharmacol 2021; 12: 1-9. https://doi.org/10.3389/fphar.2021.726643 |
[27]
, who observed that most respondents in their Thailand study purchased drugs within a month, reflecting a similar frequency of self-medication practices. The similarity in findings may be due to shared factors such as ease of access to medications, previous experience with specific drugs, and the perception that common ailments can be managed without professional consultation. The recency and frequency of self-medication observed highlight the need for interventions to promote safe medication practices. Strengthening public health education, improving access to affordable healthcare, and enforcing drug dispensing regulations could help reduce potential health risks associated with frequent self-medication.
Based on this study findings, most common source of information for self-medication was previous prescriptions (40.2%), indicating that individuals relied on their prior experiences and prescriptions to guide their self-medication practices. The study's findings indicate that the previous prescription was the primary source of information for self-medication among participants. This study result differed from a study by Namvar and Gerayeli
| [28] | Namvar MA, Mansori K, Gerayeli M. Self-Medication for Oral Health Problems in COVID-19 Outbreak: Prevalence and Associated Factors. Odovtos - Int J Dent Sci 2022; 24: 191-9. https://doi.org/10.15517/IJDS.2022.50876 |
[28]
on self-medication for oral health problems during the COVID-19 outbreak. The study found that most respondents got information from friends and relatives. The possible reason why a previous prescription is the main source of information for self-medication in this study could be that individuals who have previously received a prescription for a specific medication may be familiar with its name, dosage, and usage instructions. The difference in findings may be due to variations in health-seeking behaviours, types of ailments, social network, and accessibility to formal healthcare services across contexts. This finding has important implications for public health interventions such as targeting prescription retention practices and educating the public on the dangers of using old prescriptions without updated medical advice could help reduce inappropriate self-medication and its potential risks.
Majority of participants in this study got the drugs they used for self-medication from big pharmacies (67.8%), followed by medicine shops from the environment (43.5%). This finding is consistent with Bassi et al.
| [17] | Bassi PU, Osakwe AI, Builders M, Ettebong E, Kola G, Oreagbai I. Prevalence and Determinants of Self-Medication Practices among Nigerians 2021; 34: 634-49. |
[17]
, who reported that community pharmacy shops were the primary source of self-medicated drugs among Nigerians. Similarly, Akande-Sholabi and Adisa
] observed that undergraduate healthcare students also relied mainly on community pharmacies for self-medication. The high reliance on big pharmacies underscores the need for stricter regulation of drug sales and enhanced pharmacist-led counselling in these settings. By ensuring proper dispensing practices, policymakers can help reduce inappropriate self-medication and its associated risks.
This study found that the leading reasons for self-medication among respondents were the perception that illnesses were minor and did not require a doctor’s attention (54.2%), the need for quick relief (44.9%), financial constraints (38.3%), convenience (22.9%), and confidence in personal drug knowledge (12.1%). These findings are consistent with studies by Selvaraj and Ramalingam
| [29] | S G, Selvaraj K, Ramalingam A. Prevalence of self-medication practices and its associated factors in Urban Puducherry, India. Perspect Clin Res 2014; 5: 32. https://doi.org/10.4103/2229-3485.124569 |
[29]
in India, Chautrakarn et al.
| [27] | Chautrakarn S, Khumros W, Phutrakool P. Self-Medication With Over-the-counter Medicines Among the Working Age Population in Metropolitan Areas of Thailand. Front Pharmacol 2021; 12: 1-9. https://doi.org/10.3389/fphar.2021.726643 |
[27]
in Thailand, and Akande-Sholabi and Adisa
| [4] | Akande-Sholabi W, Ajamu AT, Adisa R. Prevalence, knowledge and perception of self-medication practice among undergraduate healthcare students. J Pharm Policy Pract 2021; 14: 1-11. https://doi.org/10.1186/s40545-021-00331-w |
[4]
in Nigeria, which all reported similar motivations for self-medication. However, they contrast with Namvar et al.
| [28] | Namvar MA, Mansori K, Gerayeli M. Self-Medication for Oral Health Problems in COVID-19 Outbreak: Prevalence and Associated Factors. Odovtos - Int J Dent Sci 2022; 24: 191-9. https://doi.org/10.15517/IJDS.2022.50876 |
[28]
research in Nigeria, where financial constraints were identified as the primary reason, and Abdelwahed et al.
| [30] | Abdelwahed AE, Abd-elkader MM, Mahfouz A, Abdelmawla MO, Kabeel M, Elkot AG, et al. Prevalence and influencing factors of self-medication during the COVID-19 pandemic in the Arab region: a multinational cross-sectional study. BMC Public Health 2023; 23: 1-11. https://doi.org/10.1186/s12889-023-15025-y |
[30]
in the Arab region, where prior experience with similar conditions was the most common driver. Most participants may choose to self-medicate due to minor illnesses because access to healthcare facilities and healthcare professionals can be challenging, especially in rural areas or underserved communities. Long distances, transportation issues, financial constraints and the cost of treatment and consultations can make it difficult for individuals to seek medical attention for minor illnesses. As a result, self-medication becomes a more accessible and immediate option. Another reason could be that minor sicknesses such as common colds, coughs, headaches, and mild digestive issues are often familiar to individuals based on their previous experiences. These findings implication shows that self-medication is often a rational choisce in settings where healthcare access is limited, but they also underscore the potential health risks when practiced without professional guidance. Addressing financial and geographic barriers, alongside public education on the risks of self-medication, could reduce unsafe practices while improving timely access to appropriate care.
Furthermore this study found that most respondents (51.9%) selected drugs for self-medication based on their symptom assessment, followed by obtaining prescriptions from medicine shops (35.5%), advice from people around them (22.9%), and, least frequently, guidance from auxiliary nurses (20.1%). These findings align with studies by Bassi et al.
| [17] | Bassi PU, Osakwe AI, Builders M, Ettebong E, Kola G, Oreagbai I. Prevalence and Determinants of Self-Medication Practices among Nigerians 2021; 34: 634-49. |
[17]
and Akande-Sholabi & Adisa
], where symptom-based decisions and community pharmacy input were common. The similarity with Nigerian studies may stem from comparable healthcare system challenges. These patterns have significant implications for public health interventions, as they underscore the need for targeted community education, enhanced regulation of pharmaceutical sales, and increased access to professional medical advice to promote safe and informed self-medication practices.
Based on the outcome of this study, the majority of respondents agreed that the following factors influence self-medication: long distance to the hospital, lack of access to the hospital, high cost of healthcare services, non-availability of a hospital, lack of drugs in the hospital, lack of healthcare workers in the hospital, lack of health insurance, lack of policies regulating self-medication, poor economy and standard of living in this country, lack of money to pay hospital bills, and insufficient information about the dangers of self-medication can all cause self-medication. However, most of the respondents were more convinced that lack of money to pay hospital bills can cause self-medication, with a mean score of 4.81 ± 0.7, followed by high costs of healthcare services/treatment and test costs can cause self-medication with a mean score of 4.64 ± 0.89. The possible reason for this could be that Nigeria has a high poverty rate, with a significant portion of the population living below the poverty line. Limited financial resources and a lack of disposable income make it challenging for individuals to afford regular medical consultations and prescribed medications. In such circumstances, self-medication becomes a practical option for managing minor health issues. These factors differ from those in a study by Donald et al.
| [31] | Donald B, et al. Perception and practice of self-medication among non-clinical students. Niger Heal J 2016; 16. |
[31]
in Nigeria. Previous experience was noted as the most cmmon factor of self-medication among respondents in their study. These findings imply that reducing the financial burden of healthcare through subsidized services, expanded health insurance, and affordable drug pricing could significantly lower the prevalence of self-medication and encousrage safer, evidence-based health-seeking behaviours.
5. Policy Relevance and Recommendations
The high prevalence of self-medication observed in this study underscores the urgent need for targeted public health interventions in Ado-Odo/Ota and similar semi-urban industrial communities. Policymakers should strengthen the enforcement of drug dispensing regulations to reduce the unregulated sale of prescription-only medicines. Expanding health insurance coverage and subsidizing essential healthcare services could help alleviate the financial constraints that drive self-medication. Furthermore, public health campaigns, especially community-based and multilingual outreach, should be implemented to educate residents on the potential dangers ofss unguided self-medication. Strengthening primary healthcare facilities in underserved areas, increasing the availability of trained health workers, and improving the supply chain for essential medicines will reduce the need for individuals to rely on self-treatment. Such measures will not only improve health-seeking behaviors but also help curb the risks of drug resistance and adverse health outcomes associated with unsafe self-medication practices.
6. Conclusion
The findings of this study show that many participants turn to self-medication as a convenient and immediate way to manage their health, largely due to limited access to healthcare facilities in rural areas. Most reported self-medicating occasionally, with a significant number doing so within the past month. Participants often relied on past prescriptions and personal experience when choosing medications, which they typically obtained from major pharmacies offering a wide range of options. Many viewed their illnesses as minor and believed a doctor’s visit was unnecessary. Drug choices were mainly based on symptoms, and financial limitations (especially the inability to afford hospital bills) emerged as a key factor driving self-medication. These insights highlight the urgent need to improve healthcare access and raise awareness about the risks of self-medication. Addressing financial and systemic barriers through targeted policies can help encourage safer, more informed health-seeking behaviours in underserved communities.
Abbreviations
SM | Self-medication |
WHO | World Health Organization |
OTC | Over the Counter |
LGA | Local Government Area |
IBM-SPSS | IBM Statistical Package for Social Sciences |
Acknowledgments
The authors thank the participants and community members of Ado Odo Ota for their support, and colleagues for their valuable input.
Author Contributions
Qali Hashi Shire: Conceptualization, Methodology, Project administration, Writing – review & editing
Olaniyi Felix Sanni: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Software, Supervision, Writing – original draft, Writing – review & editing
Michael Olabode Tomori: Investigation, Methodology, Visualization, Writing – review & editing
Funding
No External funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Aqeel T, Shabbir A, Basharat H, Bukhari M, Mobin S, Shahid H, et al. Prevalence of self-medication among urban and rural population of Islamabad, Pakistan. Trop J Pharm Res 2014; 13: 627-33.
https://doi.org/10.4314/tjpr.v13i4.22
|
| [2] |
Eticha, T., & Mesfin K. Self-Medication practices in Mekelle, Ethiopia. Plos One, 9(5), 1-5 2014.
|
| [3] |
Oyediran OO, Ayandiran EO, Olatubi MI, Olabode O. Awareness of risks associated with Self-medication among Patients attending General Out-patient Department of a Tertiary Hospital in South Western Nigeria. Int J Africa Nurs Sci 2019; 10: 110-5.
https://doi.org/10.1016/j.ijans.2019.03.001
|
| [4] |
Akande-Sholabi W, Ajamu AT, Adisa R. Prevalence, knowledge and perception of self-medication practice among undergraduate healthcare students. J Pharm Policy Pract 2021; 14: 1-11.
https://doi.org/10.1186/s40545-021-00331-w
|
| [5] |
Shaghaghi A, Asadi M, Allahverdipour H. Predictors of self-medication behavior: A systematic review. Iran J Public Health 2014; 43: 136-46.
|
| [6] |
Lukovic JA, Miletic V, Pekmezovic T, Trajkovic G, Ratkovic N, Aleksic D, et al. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS One 2014; 9.
https://doi.org/10.1371/journal.pone.0114644
|
| [7] |
Babatunde OA, Fadare JO, Ojo OJ, Durowade KA, Atoyebi OA, Ajayi PO, et al. Self-medication among health workers in a tertiary institution in South-West Nigeria. Pan Afr Med J 2016; 24.
https://doi.org/10.11604/pamj.2016.24.312.8146
|
| [8] |
Gelayee DA. Self-Medication Pattern among Social Science University Students in Northwest Ethiopia. J Pharm 2017; 2017: 1-5.
https://doi.org/10.1155/2017/8680714
|
| [9] |
Kumar N, Kanchan T, Unnikrishnan B, Rekha T, Mithra P, Kulkarni V, et al. Perceptions and Practices of Self-Medication among Medical Students in Coastal South India. PLoS One 2013; 8.
https://doi.org/10.1371/journal.pone.0072247
|
| [10] |
Helal RM, Abou-Elwafa HS. Self-medication in university students from the city of mansoura, Egypt. J Environ Public Health 2017; 2017.
https://doi.org/10.1155/2017/9145193
|
| [11] |
Ahmadi SM, Jamshidi K, Sadeghi K, Abdi A, Vahid MP. The prevalence and affecting factors on self-medication among students of Kermanshah University of Medical Science in 2014. J Clin Diagnostic Res 2016; 10: IC01-4.
https://doi.org/10.7860/JCDR/2016/18018.7847
|
| [12] |
Bennadi D. Self-medication: A current challenge. J Basic Clin Pharmacy, 5(1), 19 2014.
|
| [13] |
Chouhan K, Prasad SB. Self-medication and their consequences: A challenge to health professional. Asian J Pharm Clin Res 2016; 9: 314-7.
|
| [14] |
Uzochukwu BSC, Onwujekwe OE, Okwuosa C, Ibe OP. Patent medicine dealers and irrational use of medicines in children: The economic cost and implications for reducing childhood mortality in southeast Nigeria. PLoS One 2014; 9.
https://doi.org/10.1371/journal.pone.0091667
|
| [15] |
Erhun WO, Babalola OO, M. O. MO. Drug Regulation and Control in Nigeria: the Challenge of Counterfeit Drugs. World Health Popul 2013; 4.
https://doi.org/10.12927/whp.17597
|
| [16] |
Wabe N, Ahmed D, Angamo M. Self-Medication with Antibiotics and Antimalarials in the Community of Silte Zone, South Ethiopia. TAF Prev Med Bull 2012; 11: 529.
https://doi.org/10.5455/pmb.1-1314892446
|
| [17] |
Bassi PU, Osakwe AI, Builders M, Ettebong E, Kola G, Oreagbai I. Prevalence and Determinants of Self-Medication Practices among Nigerians 2021; 34: 634-49.
|
| [18] |
Gbadebo AM, Taiwo AM, Ayedun H, Adeola AJ. Geochemical analysis of groundwater quality in Agbara and environs. Appl Ecol Environ Res 2012; 10: 375-84.
https://doi.org/10.15666/aeer/1003_375384
|
| [19] |
Hoffmeyer-Zlotnik JHP. Harmonisation of demographic and socio-economic variables in cross-national survey research. Bull Méthodologie Sociol 2008; 98: 5-24.
https://doi.org/10.1177/075910630809800103
|
| [20] |
Omolase CO, Adeleke OE, Afolabi AO AO. Self-medication among General Outpatient in Nigerian community hospital. Annu J Postgrad Med 2007; 5 64-6 2007.
|
| [21] |
Yusuff KB, Omarusehe LD. Determinants of self medication practices among pregnant women in Ibadan, Nigeria. Int J Clin Pharm 2011; 33: 868-75.
https://doi.org/10.1007/s11096-011-9556-4
|
| [22] |
Afolabi AO. Factors influencing the pattern of self-medication in an adult Nigerian population. Ann Afr Med 2008; 7: 120-7.
https://doi.org/10.4103/1596-3519.55666
|
| [23] |
Teke GN, Nde SL, Suh MB. Self medication practice and associated factors at the regional hospital Bamenda, Cameroon: a prospective study. Int J Basic Clin Pharmacol 2017; 6: 1560.
https://doi.org/10.18203/2319-2003.ijbcp20172716
|
| [24] |
Awad AI, Eltayeb IB, Capps PA. Self-medication practices in Khartoum State, Sudan. Eur J Clin Pharmacol 2006; 62: 317-24.
https://doi.org/10.1007/s00228-006-0107-1
|
| [25] |
Abrha S, Molla F, Melkam W. Self-medication Practice : the Case of Kolladiba Town, North West Ethiopia. Int J Pharma Sci Res 2014; 5: 670-7.
|
| [26] |
Abdallah, Salisu & Vanessa P. HEALTH CARE IN GHANA: A Report of the Austrian Centre for Country of Origin & Asylum Research and Development 2009.
|
| [27] |
Chautrakarn S, Khumros W, Phutrakool P. Self-Medication With Over-the-counter Medicines Among the Working Age Population in Metropolitan Areas of Thailand. Front Pharmacol 2021; 12: 1-9.
https://doi.org/10.3389/fphar.2021.726643
|
| [28] |
Namvar MA, Mansori K, Gerayeli M. Self-Medication for Oral Health Problems in COVID-19 Outbreak: Prevalence and Associated Factors. Odovtos - Int J Dent Sci 2022; 24: 191-9.
https://doi.org/10.15517/IJDS.2022.50876
|
| [29] |
S G, Selvaraj K, Ramalingam A. Prevalence of self-medication practices and its associated factors in Urban Puducherry, India. Perspect Clin Res 2014; 5: 32.
https://doi.org/10.4103/2229-3485.124569
|
| [30] |
Abdelwahed AE, Abd-elkader MM, Mahfouz A, Abdelmawla MO, Kabeel M, Elkot AG, et al. Prevalence and influencing factors of self-medication during the COVID-19 pandemic in the Arab region: a multinational cross-sectional study. BMC Public Health 2023; 23: 1-11.
https://doi.org/10.1186/s12889-023-15025-y
|
| [31] |
Donald B, et al. Perception and practice of self-medication among non-clinical students. Niger Heal J 2016; 16.
|
Cite This Article
-
ACS Style
Shire, Q. H.; Sanni, O. F.; Tomori, M. O. Prevalence and Factors Associated with Self-medication in a Nigerian Rural Community. World J. Public Health 2025, 10(4), 467-475. doi: 10.11648/j.wjph.20251004.14
 Copy
|
Copy
|
 Download
Download
-
@article{10.11648/j.wjph.20251004.14,
author = {Qali Hashi Shire and Olaniyi Felix Sanni and Michael Olabode Tomori},
title = {Prevalence and Factors Associated with Self-medication in a Nigerian Rural Community
},
journal = {World Journal of Public Health},
volume = {10},
number = {4},
pages = {467-475},
doi = {10.11648/j.wjph.20251004.14},
url = {https://doi.org/10.11648/j.wjph.20251004.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251004.14},
abstract = {Background: Self-medication (SM) is defined by the World Health Organization (WHO) as the self-administration of medication without a valid prescription or without consulting a healthcare professional. This study aims to examine the Prevalence of self-medication and the associated factors in Ado-Odo-Ota Ogun state Nigeria Methods: The study utilised a descriptive cross-sectional study that used a questionnaire to elicit responses from residents of Ado-Odo Ota Local Government Area (LGA). The study employed a multi-stage sampling approach, and data were analysed using IBM-Statistical Package for Social Sciences (IBM-SPSS) version 28.0. Results: The prevalence of self-medication in Ado Odo Ota over the past year was 78.4%. About 51.6% of respondents reported self-medicating occasionally, with 24.8% doing so within the last week. Previous prescriptions were the most common source of drug information (40.2%), while big pharmacies were the primary source of drugs. The majority (54.2%) self-medicated because they perceived their illnesses as minor and not requiring a doctor’s attention. Drug selection was mainly based on symptoms (51.9%). The leading reasons for self-medication included financial constraints, with lack of money to pay hospital bills (mean = 4.81 ± 0.7) and the high cost of treatment and tests (mean = 4.64 ± 0.89) strongly influencing this behavior. Conclusion: These findings underscore the need for improved access to healthcare facilities in rural areas and increase awareness about the potential risks and limitations of self-medication.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Prevalence and Factors Associated with Self-medication in a Nigerian Rural Community
AU - Qali Hashi Shire
AU - Olaniyi Felix Sanni
AU - Michael Olabode Tomori
Y1 - 2025/09/30
PY - 2025
N1 - https://doi.org/10.11648/j.wjph.20251004.14
DO - 10.11648/j.wjph.20251004.14
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 467
EP - 475
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20251004.14
AB - Background: Self-medication (SM) is defined by the World Health Organization (WHO) as the self-administration of medication without a valid prescription or without consulting a healthcare professional. This study aims to examine the Prevalence of self-medication and the associated factors in Ado-Odo-Ota Ogun state Nigeria Methods: The study utilised a descriptive cross-sectional study that used a questionnaire to elicit responses from residents of Ado-Odo Ota Local Government Area (LGA). The study employed a multi-stage sampling approach, and data were analysed using IBM-Statistical Package for Social Sciences (IBM-SPSS) version 28.0. Results: The prevalence of self-medication in Ado Odo Ota over the past year was 78.4%. About 51.6% of respondents reported self-medicating occasionally, with 24.8% doing so within the last week. Previous prescriptions were the most common source of drug information (40.2%), while big pharmacies were the primary source of drugs. The majority (54.2%) self-medicated because they perceived their illnesses as minor and not requiring a doctor’s attention. Drug selection was mainly based on symptoms (51.9%). The leading reasons for self-medication included financial constraints, with lack of money to pay hospital bills (mean = 4.81 ± 0.7) and the high cost of treatment and tests (mean = 4.64 ± 0.89) strongly influencing this behavior. Conclusion: These findings underscore the need for improved access to healthcare facilities in rural areas and increase awareness about the potential risks and limitations of self-medication.
VL - 10
IS - 4
ER -
Copy
|
Download