Introduction: It has been established that homosexuality plays a considerable role in the persistence of the Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), and Hepatitis C Virus (HCV) infections, but data related to their extent remains paradoxically fragmentary. Objectives: This study aimed to determine the prevalence and determinants of viral infection (Human Immunodeficiency Virus and hepatic viral infections) among homosexuals, bisexuals, and transgenders in Kinshasa, Democratic Republic of the Congo. Methods: Between February 1 and March 30, 2022, an analytical cross-sectional study was conducted among Kinshasa's homosexual, bisexual, and transgender populations. The snowball method was used to choose participants from homosexuals’ organisations. Sociodemographic information and the prevalence of viral infections (HIV, HBV, and HCV) were included as study parameters. The determinants of viral infections were found using multivariate logistic regression. Results: A total of 555 participants (mean age: 28.5±7.8 years, unmarried: 44.9%) were enrolled. Human immunodeficiency virus, hepatitis B, and hepatitis C infection rates were, respectively, 31.5%, 6.3%, and 9.7% prevalent. HIV-HCV, HIV-HBV, and HIV-HBV-HCV coinfection rates were 4.7%, 4.1%, and 0.7%, respectively. HIV and HBV infection had the same risk factors namely piercing, incarceration, prostitution, and non-condom usage. HCV infection was more pronounced among individuals with piercing, STIs and a previous occurrence of jaundice. Conclusion: In Kinshasa, HIV, HBV, and HCV infections were widespread among homosexuals, bisexuals, and transgender people. Actions targeting LBGTs are essential to reduce HIV, HCV and HBV infections transmission in the community.
| Published in | Central African Journal of Public Health (Volume 10, Issue 2) |
| DOI | 10.11648/j.cajph.20241002.15 |
| Page(s) | 100-110 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Profile, HIV, Hepatitis, Homosexuality, Bisexuality, Transgender, Kinshasa
2.1. Study Design
2.2. Study Setting
2.3. Study Population and Sampling Strategy
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
All n=555 | Born in Kinshasa n=207 | Born outside Kinshasa n=348 | p | |
|---|---|---|---|---|
Age (mean±sd) | 28,5±7,8 | 27,1±7,0 | 29,3±8,1 | 0,002 |
Age group (years) | 0,001 | |||
13–19 | 80 (14,4) | 32 (15,5) | 48 (13,8) | |
20–29 | 235 (42,3) | 97 (46,9) | 138 (39,7) | |
30–39 | 188 (33,9) | 72 (34,8) | 116 (33,3) | |
40–49 | 52 (9,4) | 6 (2,9) | 46 (13,2) | |
Marital status | 0,748 | |||
Married | 49 (8,8) | 22 (10,6) | 27 (7,8) | |
Single | 249 (44,9) | 88 (42,5) | 161 (46,3) | |
Civil union | 56 (10,1) | 20 (9,7) | 36 (10,3) | |
Cohabitation | 175 (31,5) | 68 (32,9) | 107 (30,7) | |
Homosexual couple | 26 (4,7) | 9 (4,3) | 17 (4,9) | |
Education | 0,221 | |||
Primary school | 48 (8,6) | 21 (10,1) | 27 (7,8) | |
Secondary school | 407 (73,3) | 143 (69,1) | 264 (75,9) | |
University | 100 (18,0) | 43 (20,8) | 57 (16,4) | |
Occupation | 0,730 | |||
Unemployed | 115 (20,7) | 46 (22,2) | 69 (19,8) | |
Sex workers | 110 (19,8) | 39 (18,8) | 71 (20,4) | |
Private employee | 245 (44,1) | 94 (45,4) | 151 (43,4) | |
Government employee | 85 (15,3) | 28 (13,5) | 57 (16,4) | |
Religion | 0,188 | |||
Catholic | 96 (17,3) | 25 (12,1) | 71 (20,4) | |
Protestant | 54 (9,7) | 18 (8,7) | 36 (10,3) | |
Kimbanguist | 59 (10,6) | 20 (9,7) | 39 (11,2) | |
Pentecostal Church | 270 (48,6) | 118 (57,0) | 152 (43,7) | |
Islamic | 11 (2,0) | 4 (1,9) | 7 (2,0) | |
Buddhist | 13 (2,3) | 8 (3,9) | 5 (1,4) | |
Atheist | 37 (6,7) | 11 (5,3) | 26 (7,5) | |
Other | 15 (2,7) | 3 (1,4) | 12 (3,4) |
3.1. Prevalence of HIV, HBV, and HCV Infections Among Homosexuals, Bisexuals, and Transgender People
Infection profile | Number | % |
|---|---|---|
Not infected | 348 | 62,7 |
Infected with at least one virus | 207 | 37,3 |
Mono infected | 154 | 27,8 |
HIV-HCV | 26 | 4,7 |
HIV-HBV | 23 | 4,1 |
HIV-HBV-HCV | 4 | 0,7 |
3.2. Prevalence of HIV, HBV, and HCV Infections
3.2.1. Prevalence of HIV, HBV, and HCV Infections According to Age
3.2.2. Frequency of HIV, HBV, and HCV According to Sexual Orientation
3.3. Determinants of HIV, HBV and HCV Infections
3.3.1. Determinants of HIV Infection
Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
p | OR (IC95%) | p | QRa (IC95%) | |
Piercing | ||||
No | 1 | 1 | ||
Yes | 0,005 | 3,69 (1,70-4,45) | 0,007 | 3,56 (1,52-4,32) |
Incarceration | ||||
No | 1 | 1 | ||
Yes | 0,016 | 1,95 (1,01-2,86) | 0,012 | 2,06 (1,14-2,57) |
STI | ||||
No | 1 | 1 | ||
Yes | 0,012 | 2,41 (1,12-3,18) | 0,356 | 1,24 (0,78-1,98) |
Prostitution | ||||
No | 1 | 1 | ||
Yes | 0,025 | 2,23 (1,86-3,77) | 0,044 | 1,97 (1,29-2,63) |
No-use of condom | ||||
No | 1 | 1 | ||
Yes | 0,002 | 3,21 (1,83-5,75) | 0,002 | 3,09 (1,73-4,60) |
3.3.2. Determinants of HCV Infection
Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
p | OR (IC95%) | p | QRa (IC95%) | |
Piercing | ||||
No | 1 | 1 | ||
Yes | 0,002 | 2,72 (1,42-5,20) | 0,005 | 2,59 (1,34-5,00) |
Surgery | ||||
No | 1 | 1 | ||
Yes | 0,005 | 2,88 (1,66-4,50) | 0,779 | 1,10 (0,56-2,17) |
STI | ||||
No | 1 | 1 | ||
Yes | 0,012 | 2,45 (1,71-3,96) | 0,017 | 2,17 (1,56-3,45) |
Jaundice | ||||
No | 1 | 1 | ||
Yes | 0,027 | 2,80 (1,75-4,81) | 0,030 | 2,24 (1,63-4,46) |
3.3.3. Determinants of HBV Infection
Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
p | OR (IC95%) | p | QRa (IC95%) | |
Piercing | ||||
No | 1 | 1 | ||
Yes | 0,006 | 3,06 (1,97-4,38) | 0,025 | 2,61 (1,71-3,62) |
Incarceration | ||||
No | 1 | 1 | ||
Yes | 0,006 | 2,92 (1,96-3,384) | 0,022 | 2,56 (1,74-3,29) |
STI | ||||
No | 1 | 1 | ||
Yes | 0,032 | 1,82 (1,41-3,89) | 0,781 | 1,15 (0,44-2,98) |
Prostitution | ||||
No | 1 | 1 | ||
Yes | 0,016 | 2,26 (1,32-4,49) | 0,015 | 2,09 (1,54-3,23) |
No-use condom | ||||
No | 1 | 1 | ||
Yes | 0,002 | 3,56 (1,74-5,32) | 0,014 | 3,39 (1,63-5,02) |
Alcohol intake | ||||
No | 1 | 1 | ||
Yes | 0,042 | 1,57 (1,04-4,52) | 0,536 | 1,41 (0,48-4,15) |
4.1. Sociodemographic Characteristics of Homosexuals, Bisexuals, and Transgenders
4.2. Prevalence and Associated Factors of HIV Infection
4.3. Prevalence and Risk Factors of HCV Infection
4.4. Prevalence and Associated Factors of HBV Infection
4.5. Co-infections
4.6. Strengths and Limitations of the Study
| [1] |
Katsura R. [Congo-Kinshasa: An open heart with Patou, Congo's most open homosexual]. [podcast on the Internet]. Available from:
https://fr.allafrica.com/stories/201709150953.html [Accessed 8 August 2023]. |
| [2] |
Canada: Immigration and Refugee Board of Canada, Democratic Republic of Congo: information on the situation of sexual minorities, including laws and treatment by society and authorities; state protection and support services (2011-February 2014). [Internet]. Available from:
https://www.refworld.org/docid/53733bce4.html [Accessed 8 August 2023]. |
| [3] |
International Lesbian, Gay, Bisexual, Trans and Intersex Association. Sexual orientation laws in the world-overview. [Internet]. Available from:
https://ilga.org/downloads/2017/ILGA_WorldMap_ENGLISH_Overview_2017.pdf [Accessed 8 August 2023]. |
| [4] |
American Psychological Association. Understanding Sexual Orientation and Homosexuality. Sexual orientation and gender diversity [Serial Online]. Available from:
https://www.apa.org/topics/lgbtq/orientation [Accessed 8 August 2023]. |
| [5] | Awondo P, Geschiere P, Graeme R. [Homophobic Africa? Towards a More Nuanced View On Some Trajectories of the Politicization of Homosexuality: Cameroon, Uganda, Senegal, and South Africa]. Raisons politiques. 2013, 49(1), 95-118. |
| [6] | Lippa RA. Gender, Nature, and Nurture. 2nd Edition. New York: Routledge; 2014, pp. 358. |
| [7] | Jones C, Ciais D, Davis P, et al. Simulating the Earth system response to negative emissions. Environmental Research Letters. 2016, 11(9). |
| [8] |
Cortina C, Festy P. Identification of same-sex couples and famillies in censuses, registers and surveys. Families And Societies, Working paper series 8. [Internet]. Available from:
http://www.familiesandsocieties.eu/wp-content/uploads/2014/12/WP8CortinaFesty2014.pdf [Accessed 8 August 2023]. |
| [9] |
Bruers A. [Same-sex marriage worldwide: only 15% of the population] [Internet]. Available from:
https://www.uat.rtbf.be/article/le-mariage-homosexuel-dans-le-monde-seulement-15-de-la-population-10223143 [Accessed 8 August 2023]. |
| [10] |
Balthasar H. [Special populations for HIV/AIDS prevention, Young homosexual and bisexual males: a review of the literature]. [Internet]. Available from:
https://serval.unil.ch/resource/serval:BIB_98E0F8792338.P001/REF.pdf [Accessed 8 August 2023]. |
| [11] | Twenge JM, Sherman RA, Wells BE. Changes in American Adults’ Reported Same-Sex Sexual Experiences and Attitudes, 1973-2014. Arch Sex Behav. 2016, 45(7), 1713-30. |
| [12] | Smith C, E. Rissel J, Richters A, et al. Sex in Australia: Sexual identity, sexual attraction and sexual experience among a representative sample of adults. Australian and New Zeland Journal of Public Health. 2003, 27(2), 138-45. |
| [13] | Mor Z, Davidovich U. Sexual Orientation and Behavior of Adult Jews in Israel and the Association With Risk Behavior. Arch Sex Behav. 2016 Aug; 45(6): 1563-71. |
| [14] | Mouret-Fourme E, Messiah A. [Homosexuality and bisexuality: elements of sexual socio-biography]. Population. 1993, 48(5), 1353-1379. |
| [15] | Gwénola R. [Investigating homosexuality and sexual violence in detention]. Déviance et Société. 2004, 28(2), 233-253. |
| [16] | Lagrange H, Lhomond B. [Sexual debut. Young people's behaviour in the context of AIDS]. Paris: Editions La Découverte, Collection Recherches; 1997, pp. 431. |
| [17] |
Dah T, Larmarange J, Guiatd-Schmid J, et al. [Factors associated with non-use of condoms at last homo and heterosexual intercourse among MSM in Ouagadougou, Burkina Faso (oral communication n°SO7.2), presented at the 7th International Francophone Conference on HIV and Hepatitis (AFRAVIH), Montpellier. 2014]. [Internet]. Available from:
https://joseph.larmarange.net/Facteurs-associes-a-la-non [Accessed 8 August 2023]. |
| [18] | Farny C-C. [The Hite report on men.]. Paris: R. Laffont; 1983, pp. 847. |
| [19] |
Loukabou M, Niama R, Pembe I, et al. [HIV prevalence and associated factors among men who have sex with men in the Republic of Congo]. Health Sci. Dis. 2021, 22(8). Available from:
https://www.hsd-fmsb.org/index.php/hsd/article/view/2877 [Accessed 8 August 2023]. |
| [20] |
Lhomond B, Michaels Stuart. [Homosexuality/heterosexuality: surveys of sexual behaviour in France and the US]. Journal des anthropologues. 2000, 82-83. Available from:
http://journals.openedition.org/jda/3300 [Accessed 8 August 2023]. |
| [21] | Wade A, Kane C, Diallo P et al. HIV infection and sexually transmitted infections among men who have sex with men in Senegal. AIDS. 2005, 19(18), 2133-40. |
| [22] |
UNAIDS. Democratic Republic of the Congo. [Internet]. Available from:
https://www.unaids.org/en/regionscountries/countries/democraticrepublicofthecongo [Accessed 8 August 2023]. |
| [23] |
Centers for Disease Control and Prevention. HIV and Gay and Bisexual Men: Differences in Knowledge of Status, Prevention, Treatment, and Stigma Exist by Race/Ethnicity. [Internet]. Available from:
https://www.cdc.gov/vitalsigns/hivgaybimen/index.html [Accessed 8 August 2023]. |
| [24] | Billong S, Fokam J, Essi M, et al. [Prevalence of HIV Infection and Sexual Behaviour in Homosexual Men in the City of Yaoundé, Cameroon]. Health Sci. Dis. 2013, 14(2). |
| [25] | Mbeko S, Longo J, Camengo-Police S, et al. Persistent high-risk behavior and escalating HIV, syphilis and hepatitis B incidences among men who have sex with men living in Bangui, Central African Republic. Pan African Medical Journal. 2018, 29, 132. |
| [26] | Rapid Response Service. Rapid response: HIV risks associated with tattooing, piercing, scarification and acupuncture. Toronto, ON: Ontario HIV Treatment Network; 2012. |
| [27] |
United Nations Office on Drugs and Crime. Technical brief: Transgender people and HIV in prisons and other closed settings [Internet]. Available from:
https://www.unodc.org/documents/hiv-aids/publications/Prisons_and_other_closed_settings/22-03088_Transgender_HIV_E_ebook.pdf [Accessed 8 August 2023]. |
| [28] | Bhunu CP, Mhlanga AN, Mushayabasa S. Exploring the Impact of Prostitution on HIV/AIDS Transmission. Int Sch Res Notices. 2014, 651025. |
| [29] | Muzembo BA, Akita T, Matsuoka T, Tanaka J. Systematic review and meta-analysis of hepatitis C virus infection in the Democratic Republic of Congo. Public Health. 2016, 139, 13-21. |
| [30] | Moradi G, Soheili M, Rashti R, Dehghanbanadaki H, Nouri E, Zakaryaei F, Amini EE, Baiezeedi S, Ahmadi S, Moradi Y. The prevalence of hepatitis C and hepatitis B in lesbian, gay, bisexual and transgender populations: a systematic review and meta-analysis. Eur J Med Res. 2022, 27(1), 47. |
| [31] | Tohme RA, Holmberg SD. Transmission of hepatitis C virus infection through tattooing and piercing: a critical review. Clin Infect Dis. 2012, 54(8), 1167-78. |
| [32] |
Osella AR, Massa MA, Joekes S, Blanch N, Yacci MR, Centonze S, Sileoni S. Hepatitis B and C virus sexual transmission among homosexual men. Am J Gastroenterol. 1998, 93(1), 49-52.
https://doi.org/10.1111/j.1572-0241.1998.049_c.x PMID: 9448173. |
| [33] | Page K, Mirzazadeh A, Rice TM, Grebely J, Kim AY, Cox AL, Morris MD, Hellard M, Bruneau J, Shoukry NH, Dore GJ, Maher L, Lloyd AR, Lauer G, Prins M, McGovern BH. Interferon Lambda 4 Genotype Is Associated With Jaundice and Elevated Aminotransferase Levels During Acute Hepatitis C Virus Infection: Findings From the InC3 Collaborative. Open Forum Infect Dis. 2016, 3(1), ofw024. |
| [34] | Jin F, Dore GJ, Matthews G, Luhmann N, Macdonald V, Bajis S, Baggaley R, Mathers B, Verster A, Grulich AE. Prevalence and incidence of hepatitis C virus infection in men who have sex with men: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021, 6(1), 39-56. |
| [35] | Shindano, T. A., Kabinda, J. M., Mitashi, P. et al. Hepatitis B virus infection in the Democratic Republic of Congo: a systematic review of prevalence studies (2000–2016). J Public Health (Berl.). 2018, 26, 595–603. |
| [36] | Sadio A, Gbeasor-Komlanvi F, Konu, et al. [Prevalence and factors associated with HIV infection and hepatitis B among men who have sex with men in Togo in 2017] Médecine et Santé Tropicales. 2019, 29(3), 294-301. |
| [37] |
Semaille C, Michel A, Lot F, et al. [Summary of epidemiological data on HIV/AIDS and sexually transmitted infections in the male homosexual population in France. The fight against HIV/AIDS and sexually transmitted infections in France - 10 years of surveillance, 1996-2005]. [Internet]. Available from:
http://mediatheque.lecrips.net/docs/PDF_GED/S56680.pdf [Accessed 8 August 2023]. |
APA Style
Kamuanga, M. K., Lubaki, J. F., Ngangu, P. N., Natuhoyila, A. N., Kiswaya, E. S., et al. (2024). Profile of Homosexuals, Bisexuals, and Transgender People in Kinshasa, the Democratic Republic of the Congo: A Cross-Sectional Study. Central African Journal of Public Health, 10(2), 100-110. https://doi.org/10.11648/j.cajph.20241002.15
ACS Style
Kamuanga, M. K.; Lubaki, J. F.; Ngangu, P. N.; Natuhoyila, A. N.; Kiswaya, E. S., et al. Profile of Homosexuals, Bisexuals, and Transgender People in Kinshasa, the Democratic Republic of the Congo: A Cross-Sectional Study. Cent. Afr. J. Public Health 2024, 10(2), 100-110. doi: 10.11648/j.cajph.20241002.15
AMA Style
Kamuanga MK, Lubaki JF, Ngangu PN, Natuhoyila AN, Kiswaya ES, et al. Profile of Homosexuals, Bisexuals, and Transgender People in Kinshasa, the Democratic Republic of the Congo: A Cross-Sectional Study. Cent Afr J Public Health. 2024;10(2):100-110. doi: 10.11648/j.cajph.20241002.15
@article{10.11648/j.cajph.20241002.15,
author = {Michael Kapitene Kamuanga and Jean-Pierre Fina Lubaki and Patrick Ntontolo Ngangu and Aliocha Nkodila Natuhoyila and Ernest Sumaili Kiswaya and Philippe Lukanu Ngwala},
title = {Profile of Homosexuals, Bisexuals, and Transgender People in Kinshasa, the Democratic Republic of the Congo: A Cross-Sectional Study
},
journal = {Central African Journal of Public Health},
volume = {10},
number = {2},
pages = {100-110},
doi = {10.11648/j.cajph.20241002.15},
url = {https://doi.org/10.11648/j.cajph.20241002.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20241002.15},
abstract = {Introduction: It has been established that homosexuality plays a considerable role in the persistence of the Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), and Hepatitis C Virus (HCV) infections, but data related to their extent remains paradoxically fragmentary. Objectives: This study aimed to determine the prevalence and determinants of viral infection (Human Immunodeficiency Virus and hepatic viral infections) among homosexuals, bisexuals, and transgenders in Kinshasa, Democratic Republic of the Congo. Methods: Between February 1 and March 30, 2022, an analytical cross-sectional study was conducted among Kinshasa's homosexual, bisexual, and transgender populations. The snowball method was used to choose participants from homosexuals’ organisations. Sociodemographic information and the prevalence of viral infections (HIV, HBV, and HCV) were included as study parameters. The determinants of viral infections were found using multivariate logistic regression. Results: A total of 555 participants (mean age: 28.5±7.8 years, unmarried: 44.9%) were enrolled. Human immunodeficiency virus, hepatitis B, and hepatitis C infection rates were, respectively, 31.5%, 6.3%, and 9.7% prevalent. HIV-HCV, HIV-HBV, and HIV-HBV-HCV coinfection rates were 4.7%, 4.1%, and 0.7%, respectively. HIV and HBV infection had the same risk factors namely piercing, incarceration, prostitution, and non-condom usage. HCV infection was more pronounced among individuals with piercing, STIs and a previous occurrence of jaundice. Conclusion: In Kinshasa, HIV, HBV, and HCV infections were widespread among homosexuals, bisexuals, and transgender people. Actions targeting LBGTs are essential to reduce HIV, HCV and HBV infections transmission in the community.
},
year = {2024}
}
TY - JOUR T1 - Profile of Homosexuals, Bisexuals, and Transgender People in Kinshasa, the Democratic Republic of the Congo: A Cross-Sectional Study AU - Michael Kapitene Kamuanga AU - Jean-Pierre Fina Lubaki AU - Patrick Ntontolo Ngangu AU - Aliocha Nkodila Natuhoyila AU - Ernest Sumaili Kiswaya AU - Philippe Lukanu Ngwala Y1 - 2024/04/11 PY - 2024 N1 - https://doi.org/10.11648/j.cajph.20241002.15 DO - 10.11648/j.cajph.20241002.15 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 100 EP - 110 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20241002.15 AB - Introduction: It has been established that homosexuality plays a considerable role in the persistence of the Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), and Hepatitis C Virus (HCV) infections, but data related to their extent remains paradoxically fragmentary. Objectives: This study aimed to determine the prevalence and determinants of viral infection (Human Immunodeficiency Virus and hepatic viral infections) among homosexuals, bisexuals, and transgenders in Kinshasa, Democratic Republic of the Congo. Methods: Between February 1 and March 30, 2022, an analytical cross-sectional study was conducted among Kinshasa's homosexual, bisexual, and transgender populations. The snowball method was used to choose participants from homosexuals’ organisations. Sociodemographic information and the prevalence of viral infections (HIV, HBV, and HCV) were included as study parameters. The determinants of viral infections were found using multivariate logistic regression. Results: A total of 555 participants (mean age: 28.5±7.8 years, unmarried: 44.9%) were enrolled. Human immunodeficiency virus, hepatitis B, and hepatitis C infection rates were, respectively, 31.5%, 6.3%, and 9.7% prevalent. HIV-HCV, HIV-HBV, and HIV-HBV-HCV coinfection rates were 4.7%, 4.1%, and 0.7%, respectively. HIV and HBV infection had the same risk factors namely piercing, incarceration, prostitution, and non-condom usage. HCV infection was more pronounced among individuals with piercing, STIs and a previous occurrence of jaundice. Conclusion: In Kinshasa, HIV, HBV, and HCV infections were widespread among homosexuals, bisexuals, and transgender people. Actions targeting LBGTs are essential to reduce HIV, HCV and HBV infections transmission in the community. VL - 10 IS - 2 ER -
Department of Family Medicine and Primary Health Care, Protestant University of Congo, Kinshasa, Democratic Republic of the Congo
Department of Family Medicine and Primary Health Care, Protestant University of Congo, Kinshasa, Democratic Republic of the Congo
Department of Family Medicine and Primary Health Care, Protestant University of Congo, Kinshasa, Democratic Republic of the Congo; Institut Médical Evangélique (IME), Kimpese, Democratic of the Congo
Department of Family Medicine and Primary Health Care, Protestant University of Congo, Kinshasa, Democratic Republic of the Congo
Department of Family Medicine and Primary Health Care, Protestant University of Congo, Kinshasa, Democratic Republic of the Congo; Department of Internal Medicine, University of Kinshasa, Kinshasa, Democratic Republic of the Congo
Department of Family Medicine and Primary Health Care, Protestant University of Congo, Kinshasa, Democratic Republic of the Congo
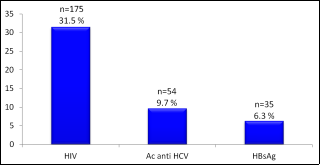
Figure 1. Prevalence HIV, HBV, and HCV infections among homosexuals, bisexuals, and transgender communities in Kinshasa.
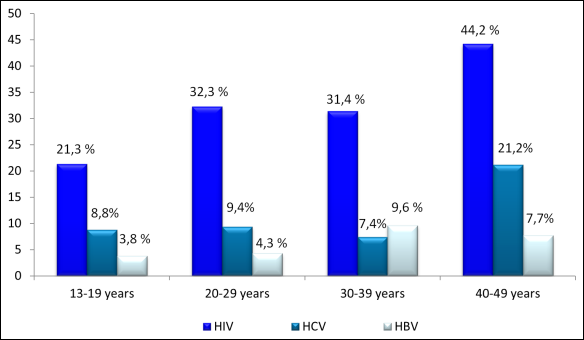
Figure 2. Frequency of HIV, HBV, and HCV infections among homosexuals, bisexuals, and transgender communities according to age.
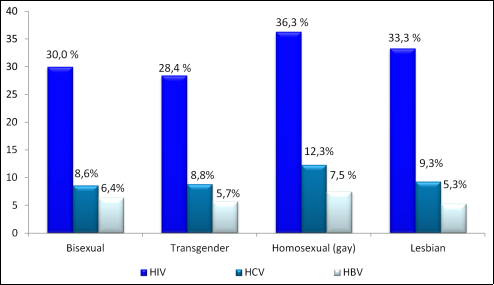
Figure 3. Frequency of HIV, HBV, and HCV infections according to sexual orientation.
Information

