Background: Impaired localized epithelial immune system leads to oral cancer. Langerhans Cells (LCs) act as regulators of immune response which are regulated by Transforming Growth Factor β. But their association in a potentially malignant disorder like Oral Submucous Fibrosis (OSF), has not been researched enough. The aim of this paper was to assess the relationship between TGF β and LCs in OSF and whether TGF β can be successfully used as a therapeutic target. Context: TGF β has been a known regulator of immune response through its action on LCs which is proven in some in –vitro studies and also some of the clinical trials targeting TGF β. Aims: The aim of this paper was to assess the relationship between TGF β and LCs in OSF and whether TGF β can be successfully used as a therapeutic target. Methods & Material: Forty OSF and nine normal buccal mucosa were sectioned and subsequently stained immunohistochemically stained anti CD1a and anti (CD105) antibody respectively. Statistical Analysis Used: Student’s-t-test and One way ANOVA was applied. Results: Overall reduction of LCs in the epithelium of OSF than normal mucosa. There was no association seen between the expression of TGFβ and LCs in different stages or grades of OSF or in normal mucosa. Conclusion: Reduced number of LCs in OSF indicates that it does not correlate with the expression of TGF β. Areca itself may have cytotoxic/genotoxic effects on LCs.
| Published in | International Journal of Clinical Oral and Maxillofacial Surgery (Volume 11, Issue 1) |
| DOI | 10.11648/j.ijcoms.20251101.15 |
| Page(s) | 40-52 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Oral Submucous Fibrosis, Langerhans cells, CD1a, TGF β, Potentially Malignant
Group | N | Mean | Std. Deviation | t | Df | P VALUE | |
|---|---|---|---|---|---|---|---|
LCs LABELLING INDEX | OSF | 40 | 6.500608 | 5.669041 | -2.224 | 20.705 | 0.037 |
CONTROL | 10 | 9.802986 | 3.743874 |
GROUPS | N | Mean | Std. Deviation | Statistics/ mean squares | df2(welch) / F(Anova) | P VALUE | |
|---|---|---|---|---|---|---|---|
LCs LABELLING INDEX | STAGE 1 | 14 | 7.163871 | 5.978992 | 10.474 | 0.323 | 0.726 |
STAGE 2 | 22 | 5.653461 | 5.356824 | ||||
STAGE 3 | 3 | 6.959327 | 7.066192 | ||||
Total | 39 | 6.296111 | 5.591688 |
GROUPS | N | Mean | Std. Deviation | Statistics/ mean squares | df2(welch) / F(Anova) | P VALUE | |
|---|---|---|---|---|---|---|---|
LCs LABELLING INDEX | GRADE 1 | 4 | 6.54749 | 5.19401 | 19.908 | 0.624 | 0.541 |
GRADE 2 | 24 | 5.547857 | 5.341275 | ||||
GRADE 3 | 11 | 7.837253 | 6.412671 | ||||
Total | 39 | 6.296111 | 5.591688 |
Dependent Variable | (I) group | (J) group | Mean Difference (I-J) | Std. Error | P VALUE |
|---|---|---|---|---|---|
LCs LABELLING INDEX | GRADE 1 | GRADE 2 | 0.999633 | 3.050179 | 0.943 |
GRADE 3 | -1.28976 | 3.297624 | 0.919 | ||
GRADE 2 | GRADE 3 | -2.2894 | 2.05643 | 0.512 |
Crosstab | Group | Total | P value | |||
|---|---|---|---|---|---|---|
NBM | OSF | |||||
TGF-BETA % EPI | NEGATIVE | Count | 0 | 3 | 3 | 0.633 |
% within group | 0.0% | 7.5% | 6.1% | |||
<1/3 | Count | 2 | 14 | 16 | ||
% within group | 22.2% | 35.0% | 32.7% | |||
1/3 - 2/3 | Count | 4 | 9 | 13 | ||
% within group | 44.4% | 22.5% | 26.5% | |||
>2/3 | Count | 3 | 14 | 17 | ||
% within group | 33.3% | 35.0% | 34.7% | |||
Total | Count | 9 | 40 | 49 | ||
% within group | 100.0% | 100.0% | 100.0% | |||
Crosstab | Group | Total | P value | |||
|---|---|---|---|---|---|---|
NBM | OSF | |||||
TGF BETA % CT | NEGATIVE | Count | 0 | 3 | 3 | 0.257 |
% within group | 0.0% | 7.5% | 6.4% | |||
<1/3 | Count | 1 | 15 | 16 | ||
% within group | 14.3% | 37.5% | 34.0% | |||
1/3 - 2/3 | Count | 4 | 8 | 12 | ||
% within group | 57.1% | 20.0% | 25.5% | |||
>2/3 | Count | 2 | 14 | 16 | ||
% within group | 28.6% | 35.0% | 34.0% | |||
Total | Count | 7 | 40 | 47 | ||
% within group | 100.0% | 100.0% | 100.0% | |||
Crosstab | STAGE OF OSF | Total | P VALUE | ||||
|---|---|---|---|---|---|---|---|
STAGE 1 | STAGE 2 | STAGE 3 | |||||
TGF-BETA % EPI | NEGATIVE | Count | 1 | 2 | 0 | 3 | 0.332 |
% within STAGE OF OSF | 7.1% | 9.1% | 0.0% | 7.7% | |||
<1/3 | Count | 6 | 7 | 1 | 14 | ||
% within STAGE OF OSF | 42.9% | 31.8% | 33.3% | 35.9% | |||
1/3 - 2/3 | Count | 5 | 3 | 0 | 8 | ||
% within STAGE OF OSF | 35.7% | 13.6% | 0.0% | 20.5% | |||
>2/3 | Count | 2 | 10 | 2 | 14 | ||
% within STAGE OF OSF | 14.3% | 45.5% | 66.7% | 35.9% | |||
Total | Count | 14 | 22 | 3 | 39 | ||
% within STAGE OF OSF | 100.0% | 100.0% | 100.0% | 100.0% | |||
Crosstab | STAGE OF OSF | Total | P value | ||||
|---|---|---|---|---|---|---|---|
STAGE 1 | STAGE 2 | STAGE 3 | |||||
TGF BETA % CT | NEGATIVE | Count | 1 | 2 | 0 | 3 | 0.240 |
% within STAGE OF OSF | 7.1% | 9.1% | 0.0% | 7.7% | |||
<1/3 | Count | 6 | 8 | 1 | 15 | ||
% within STAGE OF OSF | 42.9% | 36.4% | 33.3% | 38.5% | |||
1/3 - 2/3 | Count | 5 | 2 | 0 | 7 | ||
% within STAGE OF OSF | 35.7% | 9.1% | 0.0% | 17.9% | |||
>2/3 | Count | 2 | 10 | 2 | 14 | ||
% within STAGE OF OSF | 14.3% | 45.5% | 66.7% | 35.9% | |||
Total | Count | 14 | 22 | 3 | 39 | ||
% within STAGE OF OSF | 100.0% | 100.0% | 100.0% | 100.0% | |||
Crosstab | H/P GRADES | Total | P value | ||||
|---|---|---|---|---|---|---|---|
GRADE 1 | GRADE 2 | GRADE 3 | |||||
TGF-BETA % EPI | NEGATIVE | Count | 0 | 3 | 0 | 3 | 0.152 |
% within H/P GRADES | 0.0% | 13.0% | 0.0% | 7.9% | |||
<1/3 | Count | 1 | 11 | 2 | 14 | ||
% within H/P GRADES | 25.0% | 47.8% | 18.2% | 36.8% | |||
1/3 - 2/3 | Count | 1 | 5 | 2 | 8 | ||
% within H/P GRADES | 25.0% | 21.7% | 18.2% | 21.1% | |||
>2/3 | Count | 2 | 4 | 7 | 13 | ||
% within H/P GRADES | 50.0% | 17.4% | 63.6% | 34.2% | |||
Total | Count | 4 | 24 | 11 | 39 | ||
% within H/P GRADES | 100.0% | 100.0% | 100.0% | 100.0% | |||
Crosstab | H/P GRADES | Total | P value | ||||
|---|---|---|---|---|---|---|---|
GRADE 1 | GRADE 2 | GRADE 3 | |||||
TGF BETA % CT | NEGATIVE | Count | 0 | 3 | 0 | 3 | 0.118 |
% within H/P GRADES | 0.0% | 13.0% | 0.0% | 7.9% | |||
<1/3 | Count | 1 | 12 | 2 | 15 | ||
% within H/P GRADES | 25.0% | 52.2% | 18.2% | 39.5% | |||
1/3 - 2/3 | Count | 1 | 4 | 2 | 7 | ||
% within H/P GRADES | 25.0% | 17.4% | 18.2% | 18.4% | |||
>2/3 | Count | 2 | 4 | 7 | 13 | ||
% within H/P GRADES | 50.0% | 17.4% | 63.6% | 34.2% | |||
Total | Count | 4 | 24 | 11 | 39 | ||
% within H/P GRADES | 100.0% | 100.0% | 100.0% | 100.0% | |||
OSF | Ral Submucous Fibrosis |
DCs | Dendritic Cells |
LCs | Langerhans Cells |
TGFβ | Transforming Growth Factor Beta |
PG | Prostaglandins |
BQ | Betel Quid |
CD1a | Cluster of Differentiation1a |
CD105 | Cluster of Differentiation 105 (Anti TGFβ1, TGFβ3) |
CD4+ | Cluster of Differentiation 4 |
CD8+ | Cluster of Differentiation 8 |
HPF | High Power Field |
IHC | Immunohistochemistry |
| [1] | Arakeri G, Brennan PA. Oral submucous fibrosis: an overview of the etiology, pathogenesis, classification, and principles of management Br J Oral Maxillofac Surg 2013 Oct; 51(7): 587-93. |
| [2] | Kale AD, Mane DR, Shukla D. Expression of transforming growth factor beta and its correlation with lipodystrophy in oral submucous fibrosis: an immunohistochemical study. Med Oral Patol Oral Cir Bucal 2013 Jan; 18(1): e12-18. |
| [3] | Borkowski TA, Letterio JJ, Mackall CL, Saitoh A, Wang XJ, Roop DR. A role for TGFβ1 in langerhans cell biology. Further characterization of the epidermal langerhans cell defect in TGFβ1 Null Mice. J of Clin Invest 1997; 100(3): 575–581. |
| [4] | Rajalalitha P, Vali S. Molecular pathogenesis of oral submucous fibrosis – a collagen metabolic disorder. J Oral Pathol Med 2005; 34: 321–8. |
| [5] | Upadhyay J, Upadhyay RB, Agrawal P, Jaitley S, Shekhar R. Langerhans cells and their role in oral mucosal diseases. N Am J Med Sci 2013; 5: 505–14. |
| [6] | Jaitley S, Gopu S, Rajasekharan ST, Sivapathasundaram B. Immunohistochemical analysis of Langerhans cells in chronic gingivitis using anti-CD1a antibody. Dent Res J 2014; 11(2): 173-9. |
| [7] | Chiang CP, Wu HY, Liu BY, Wang JT, Kuo MY. Quantitative analysis of immunocompetent cells in oral submucous fibrosis in Taiwan. Oral Oncol 2002; 38(1): 56-63. |
| [8] | Sundqvist K, Liu Y, Nair J, Bartsch H, Arvidson K, Grafström RC. Cytotoxic and genotoxic effects of areca nut-related compounds in cultured human buccal epithelial cells. Can Res 1989; 40(19): 5294-98. |
| [9] | Jeng JH, Kuo ML, Hahn LJ, Kuo MY. Genotoxic and non-genotoxic effects of betel quid ingredients on oral mucosal fibroblasts in vitro. J Dent Res 1994; 73(5): 1043-49. |
| [10] | Lasisi TJ, Oluwasola AO, Lasisi OA, Akang EE. Association between langerhans cells population and histological grade of oral squamous cell carcinoma. J Oral Maxillofac Pathol 2013; 17: 329-33. |
| [11] | Prime SS, Pring M, Davies M, Paterson IC. TGF-beta signal transduction in oro-facial health and non-malignant disease (part I). Crit Rev Oral Biol Med 2004; 15: 324-36. |
| [12] | Li C, Issa R, Kumar P, Hampson IN, Lopez-Novoa JM, Bernabeu C, Kumar S. CD105 prevents apoptosis in hypoxic endothelial cells. J Cell Sci 2003 Jul; 116(1): 2677–2685. |
| [13] | Kamath VV, Krishnamurthy S, Satelur KP, Rajkumar K. Transforming growth factor-β1 and TGF-β2 act synergistically in the fibrotic pathway in oral submucous fibrosis: An immunohistochemical observation. Indian J Med Paediatr Oncol 2015; 36: 111-6. |
| [14] | Wrzesinski SH, Wan YY, Flavell RA. Transforming growth factor-beta and the immune response: implications for anticancer therapy. Clin Cancer Res 2007 Sep15: 5262-70. |
APA Style
Elangovan, E., E, E. (2025). Correlation of CD1a Positive Langerhans Cells and Transforming Growth Factor β in Oral Submucuous Fibrosis - An Immunohistochemical Study. International Journal of Clinical Oral and Maxillofacial Surgery, 11(1), 40-52. https://doi.org/10.11648/j.ijcoms.20251101.15
ACS Style
Elangovan, E.; E, E. Correlation of CD1a Positive Langerhans Cells and Transforming Growth Factor β in Oral Submucuous Fibrosis - An Immunohistochemical Study. Int. J. Clin. Oral Maxillofac. Surg. 2025, 11(1), 40-52. doi: 10.11648/j.ijcoms.20251101.15
@article{10.11648/j.ijcoms.20251101.15,
author = {Elampavai Elangovan and Elanangai E},
title = {Correlation of CD1a Positive Langerhans Cells and Transforming Growth Factor β in Oral Submucuous Fibrosis - An Immunohistochemical Study
},
journal = {International Journal of Clinical Oral and Maxillofacial Surgery},
volume = {11},
number = {1},
pages = {40-52},
doi = {10.11648/j.ijcoms.20251101.15},
url = {https://doi.org/10.11648/j.ijcoms.20251101.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcoms.20251101.15},
abstract = {Background: Impaired localized epithelial immune system leads to oral cancer. Langerhans Cells (LCs) act as regulators of immune response which are regulated by Transforming Growth Factor β. But their association in a potentially malignant disorder like Oral Submucous Fibrosis (OSF), has not been researched enough. The aim of this paper was to assess the relationship between TGF β and LCs in OSF and whether TGF β can be successfully used as a therapeutic target. Context: TGF β has been a known regulator of immune response through its action on LCs which is proven in some in –vitro studies and also some of the clinical trials targeting TGF β. Aims: The aim of this paper was to assess the relationship between TGF β and LCs in OSF and whether TGF β can be successfully used as a therapeutic target. Methods & Material: Forty OSF and nine normal buccal mucosa were sectioned and subsequently stained immunohistochemically stained anti CD1a and anti (CD105) antibody respectively. Statistical Analysis Used: Student’s-t-test and One way ANOVA was applied. Results: Overall reduction of LCs in the epithelium of OSF than normal mucosa. There was no association seen between the expression of TGFβ and LCs in different stages or grades of OSF or in normal mucosa. Conclusion: Reduced number of LCs in OSF indicates that it does not correlate with the expression of TGF β. Areca itself may have cytotoxic/genotoxic effects on LCs.
},
year = {2025}
}
TY - JOUR T1 - Correlation of CD1a Positive Langerhans Cells and Transforming Growth Factor β in Oral Submucuous Fibrosis - An Immunohistochemical Study AU - Elampavai Elangovan AU - Elanangai E Y1 - 2025/06/23 PY - 2025 N1 - https://doi.org/10.11648/j.ijcoms.20251101.15 DO - 10.11648/j.ijcoms.20251101.15 T2 - International Journal of Clinical Oral and Maxillofacial Surgery JF - International Journal of Clinical Oral and Maxillofacial Surgery JO - International Journal of Clinical Oral and Maxillofacial Surgery SP - 40 EP - 52 PB - Science Publishing Group SN - 2472-1344 UR - https://doi.org/10.11648/j.ijcoms.20251101.15 AB - Background: Impaired localized epithelial immune system leads to oral cancer. Langerhans Cells (LCs) act as regulators of immune response which are regulated by Transforming Growth Factor β. But their association in a potentially malignant disorder like Oral Submucous Fibrosis (OSF), has not been researched enough. The aim of this paper was to assess the relationship between TGF β and LCs in OSF and whether TGF β can be successfully used as a therapeutic target. Context: TGF β has been a known regulator of immune response through its action on LCs which is proven in some in –vitro studies and also some of the clinical trials targeting TGF β. Aims: The aim of this paper was to assess the relationship between TGF β and LCs in OSF and whether TGF β can be successfully used as a therapeutic target. Methods & Material: Forty OSF and nine normal buccal mucosa were sectioned and subsequently stained immunohistochemically stained anti CD1a and anti (CD105) antibody respectively. Statistical Analysis Used: Student’s-t-test and One way ANOVA was applied. Results: Overall reduction of LCs in the epithelium of OSF than normal mucosa. There was no association seen between the expression of TGFβ and LCs in different stages or grades of OSF or in normal mucosa. Conclusion: Reduced number of LCs in OSF indicates that it does not correlate with the expression of TGF β. Areca itself may have cytotoxic/genotoxic effects on LCs. VL - 11 IS - 1 ER -
Oral and Maxillofacial Pathology, Sri Venkateswara Dental College and Hospitals, Bangalore, India
Sri Sai Lakshmi Dental Clinics, Bangalore, India
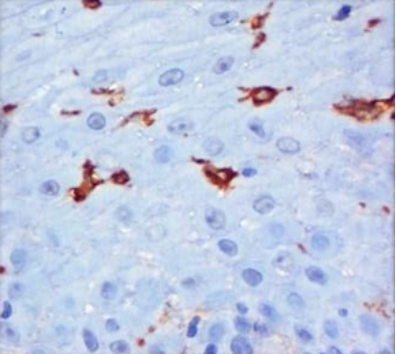
Figure 1. Photomicrograph showing CD1a stained Langerhans cells in (X400).
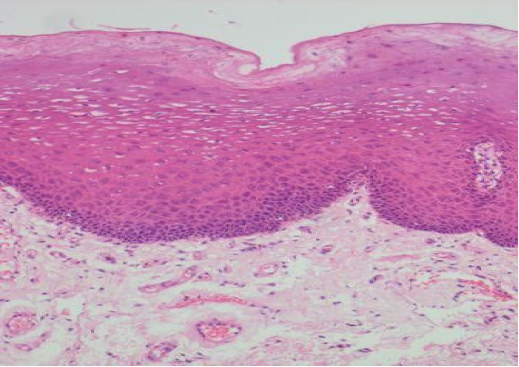
Figure 2. Photomicrograph showing Hematoxylin and Eosin stained normal buccal mucosa in (X100).
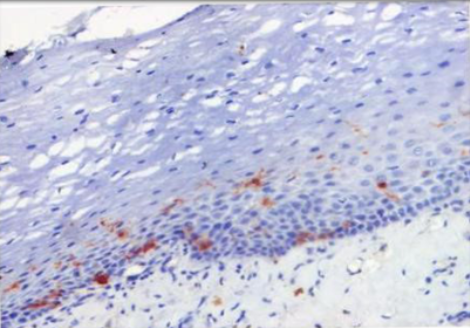
Figure 3. Photomicrograph showing CD1a stained normal buccal mucosa (X200).
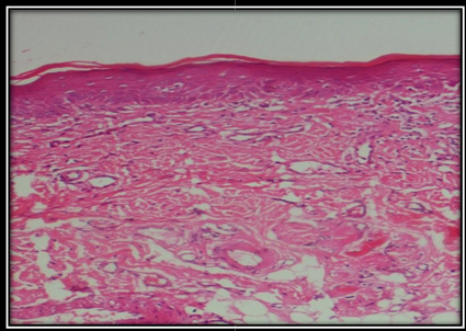
Figure 4. Photomicrograph showing Hematoxylin and Eosin stained OSF (X100).
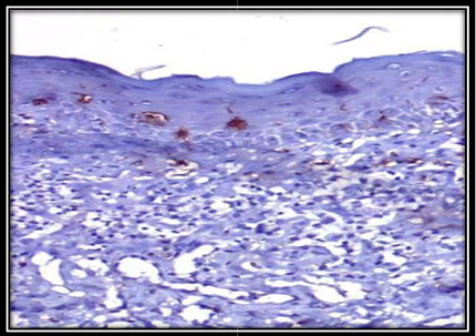
Figure 5. Photomicrograph showing CD1a stained LCs in OSF(X200).
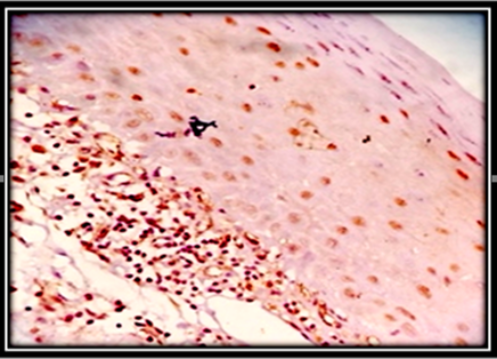
Figure 6. Photomicrograph of OSF showing MILD expression of TGF β (X200).
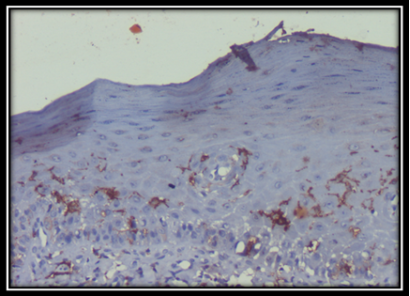
Figure 7. Photomicrograph of OSF showing LCs in cases of MILD TGFβ expression (X200).
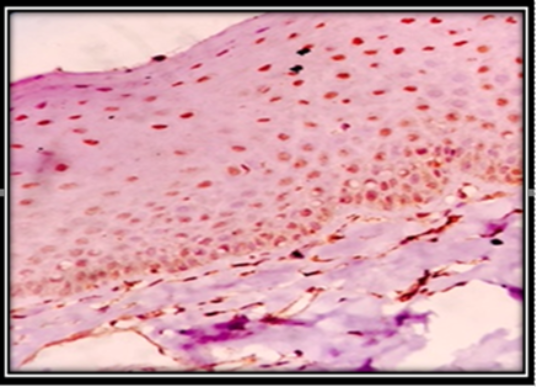
Figure 8. Photomicrograph of OSF showing MODERATE expression of TGFβ (X200).
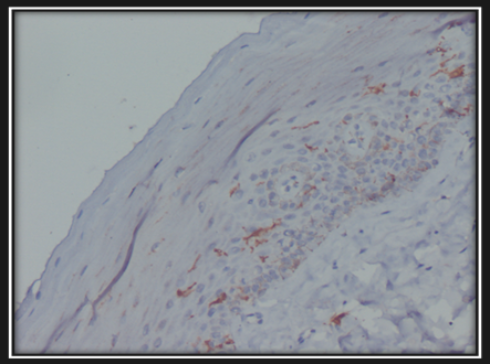
Figure 9. Photomicrograph of OSF showing LCs in cases of MODERATE TGFβ expression (X200):
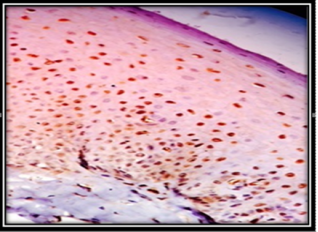
Figure 10. Photomicrograph of OSF showing SEVERE expression of TGFβ (X200).
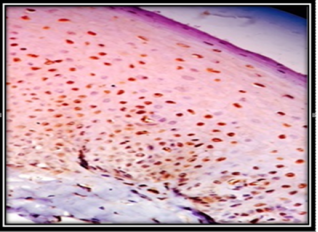
Figure 11. Photomicrograph of OSF showing LCs in cases of SEVERE TGFβ expression (X200).
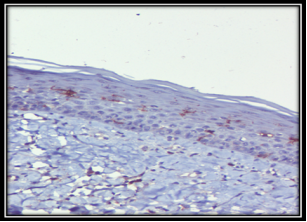
Figure 12. Photomicrograph of normal mucosa showing MILD expression of TGF β (X200):
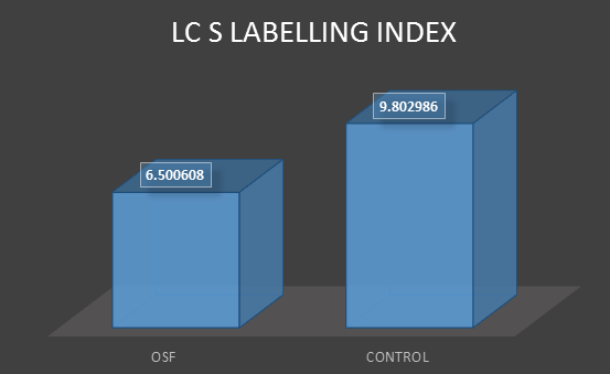
Figure 13. An overall reduction of LCs was found in OSF compared to normal oral mucosa.
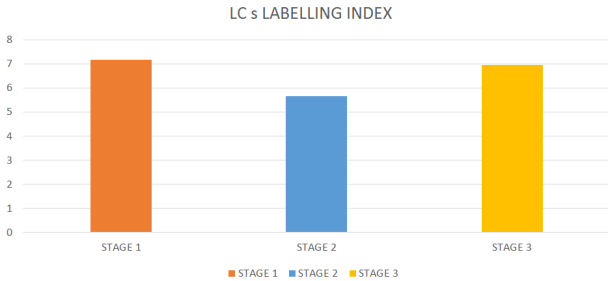
Figure 14. There was no significant difference in the number of LCs in different stages of OSF.
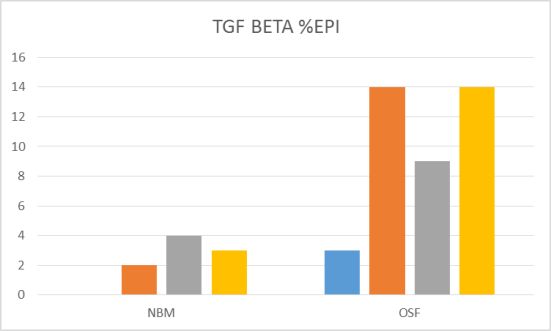
Figure 15. There was no significant difference in the epithelial expression of TGF β between normal buccal mucosa and OSF.
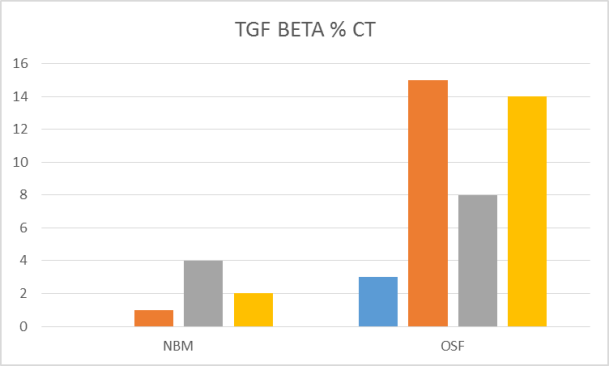
Figure 16. There was no significant difference in the expression of TGF β between connective tissue of normal buccal mucosa and OSF. While higher proportion of cases of normal mucosa showed moderate distribution, higher proportion of cases of OSF showed mild or severe distribution.
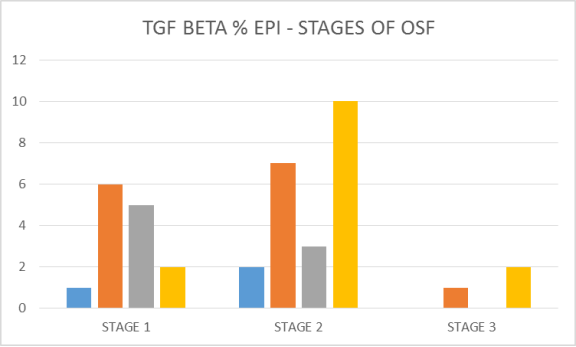
Figure 17. While in initial stage (stage I), higher proportion of cases showed mild expression, with advancing stages of OSF (stage II and stage III), a higher proportion of cases showed severe expression of TGF β in the epithelium.
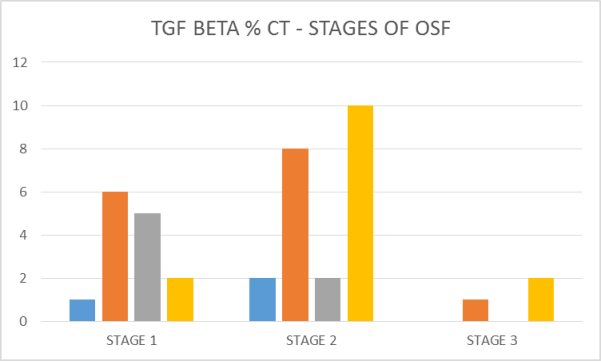
Figure 18. While in initial stage (stage I), higher proportion of cases showed mild expression, with advancing stages of OSF (stage II and stage III), a higher proportion of cases showed severe expression of TGFβ in the connective tissue.
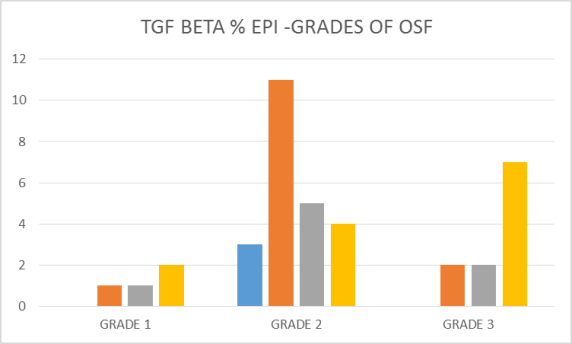
Figure 19. Severe expression of TGF β was seen in epithelium in initial (grade I) and in later stages (grade III) compared to grade II.
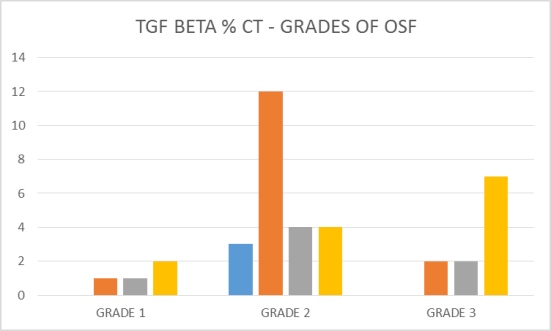
Figure 20. Severe expression of TGF β was seen in connective tissue in initial (grade I) and in later stages (grade III) compared to grade II.
Information

